14 year male boy with complaints of diminished vision both eyes since 6 months and redness off and on. vision uncorrected 6//18 in right eye and 6/12 in left eye . On examination whitish infiltrate in superior limbus with superficial corneal vascularisation in left eye more than right eye . What is the differential diagnosis and what would be the management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching PubMed
vernal keratoconjunctivitis management
Loading Image
Loading Image
Excellent — I now have all the textbook content and images needed. Let me compile the comprehensive clinical answer.
Clinical Analysis: 14-Year-Old Male with Bilateral Diminished Vision + Superior Limbal Whitish Infiltrate + Superficial Corneal Vascularization
Most Likely Diagnosis
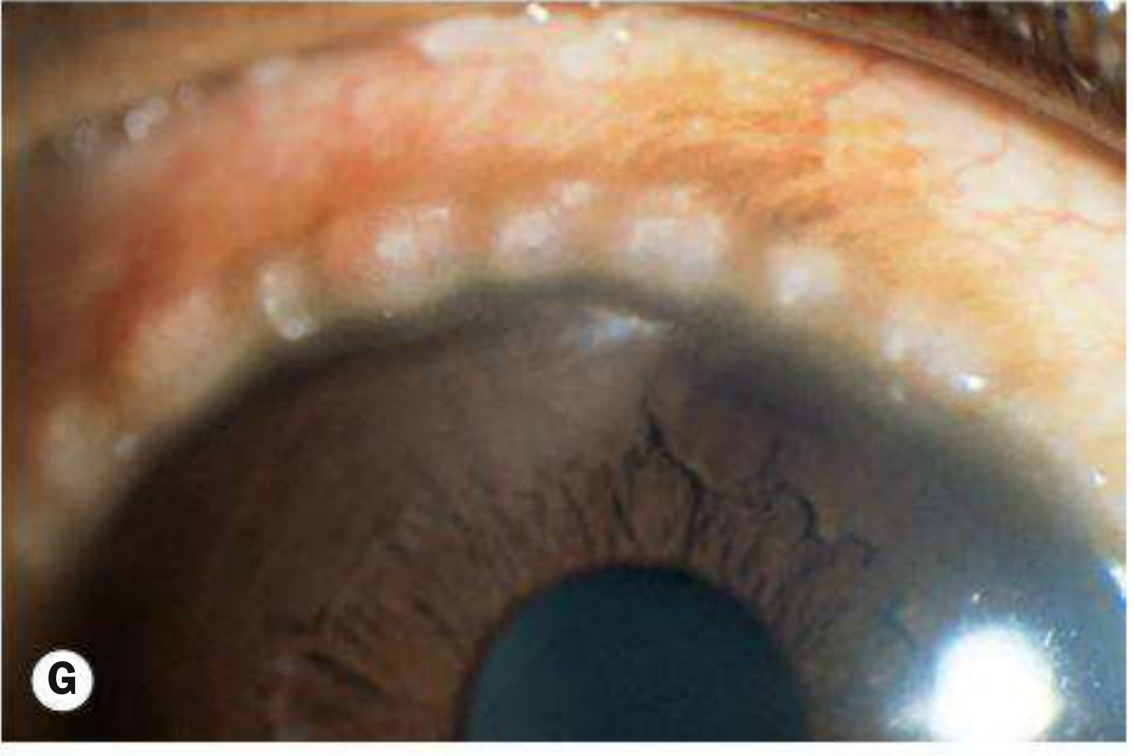
The combination of age (14 years), male sex, bilateral involvement, superior limbal whitish infiltrate, and superficial corneal vascularization is highly characteristic of Limbal Vernal Keratoconjunctivitis (VKC).
The whitish infiltrates at the superior limbus represent Horner–Trantas dots — white cellular collections (predominantly eosinophils and degenerated epithelial cells) situated at the apex of gelatinous limbal papillae. This is a pathognomonic finding of limbal VKC.
Differential Diagnosis
1. ⭐ Limbal Vernal Keratoconjunctivitis (Most Likely)
Key features supporting this diagnosis:
- Age 5–25 years; predominantly males; onset in childhood
- Bilateral (asymmetric is common — left > right here)
- Warm dry climates, sub-Saharan Africa, Middle East, South Asia (typical demographic)
- Whitish limbal infiltrates = Horner–Trantas dots at superior limbus
- Superficial corneal vascularization (peripheral vessel ingrowth)
- Recurrent redness, photophobia, intense itching
- Limbal disease typically affects Black and Asian patients; palpebral type is more common in White patients
What to look for on examination:
- Evert the upper eyelid: gelatinous limbal papillae ± cobblestone papillae on tarsal conjunctiva
- Superior punctate epithelial erosions
- Thick mucoid discharge
- Possible shield ulcer (if keratopathy advanced)

2. Superior Limbic Keratoconjunctivitis (SLK) — Theodore's SLK
- Bilateral, superior bulbar conjunctival hyperemia with limbal infiltration
- Superior pannus and fine punctate keratitis
- Associated with thyroid disease in adults
- Less likely in a 14-year-old without thyroid history; more common in middle-aged women
3. Atopic Keratoconjunctivitis (AKC)
- Similar limbal involvement including Horner–Trantas dots possible
- Inferior conjunctival predilection (unlike VKC which is superior)
- Associated with atopic dermatitis, asthma, eczema
- Peak 30–50 years; perennial symptoms; more severe corneal vascularization and scarring
- Less likely at age 14 without prominent eyelid eczema
4. Phlyctenular Keratoconjunctivitis
- Whitish nodular lesion(s) at limbus with vascularization
- Typically unilateral or asymmetric; associated with TB hypersensitivity, staphylococcal blepharitis
- Phlycten migrates centrally leaving a vascular leash
- No seasonal variation; no itching predominance
5. Marginal (Catarrhal) Keratitis
- Whitish peripheral stromal infiltrates with a clear zone between infiltrate and limbus
- Associated with staphylococcal blepharitis
- Usually adults; not primarily superior
6. Trachoma (Chlamydia trachomatis) — Herbert's Pits
- Superior pannus and limbal follicles
- In endemic regions; follicular tarsal conjunctivitis; cicatricial entropion in late disease
- Follicles at the limbus resolve leaving Herbert's pits (pathognomonic)
- Possible differential in endemic/developing world setting
7. Infectious Crystalline/Microbial Keratitis
- Unilateral typically; stromal infiltrate with epithelial defect
- Marked pain, discharge, hypopyon possible
- Less consistent with bilateral symmetric limbal presentation
Summary Differential Table
| Condition | Age | Laterality | Site | Key Feature |
|---|---|---|---|---|
| Limbal VKC | <25 yrs, male | Bilateral | Superior limbus | Horner–Trantas dots, itching |
| SLK (Theodore's) | Middle-aged female | Bilateral | Superior limbus | Thyroid association |
| AKC | 30–50 yrs | Bilateral | Inferior > superior | Eczema, perennial |
| Phlyctenular keratitis | Young | Usually unilateral | Any sector | Migrating ulcer + leash |
| Trachoma | Endemic areas | Bilateral | Superior | Herbert's pits, pannus |
| Marginal keratitis | Adults | Usually unilateral | Peripheral, NOT superior | Clear zone, staphylococcal lid |
Management
Step 1: Complete Workup
- History: Atopy (asthma, eczema), family history, seasonality, itching (cardinal VKC symptom)
- Slit lamp: Evert upper eyelid (tarsal papillae), assess Trantas dots, corneal fluorescein staining, vascularization extent
- Investigations: Conjunctival scraping — look for eosinophils (confirms allergic/VKC; not usually needed clinically)
- IOP baseline before starting steroids
Step 2: Medical Management (VKC)
Mild-to-Moderate Disease
| Drug Class | Examples | Role |
|---|---|---|
| Mast cell stabilizers | Sodium cromoglicate 2%, lodoxamide 0.1% (q.i.d.) | First-line; prevent degranulation; need 2–4 weeks onset |
| Dual-action antihistamine/mast cell stabilizer | Olopatadine 0.1%, azelastine, ketotifen | Faster onset; useful for breakthrough symptoms |
| Topical antihistamines | Emedastine, epinastine, levocabastine | Acute symptomatic relief |
| NSAIDs (topical) | Ketorolac, diclofenac | Supplement mast cell stabilizers |
| Lubricants/cool compresses | Preservative-free tears | Symptomatic; reduce allergen load |
Severe Exacerbations / Significant Keratopathy
- Topical corticosteroids: Fluorometholone 0.1%, loteprednol 0.5%, prednisolone 0.5% — short intensive courses (e.g. 2-hourly initially, rapid taper). Always monitor IOP. Do NOT use long-term.
- Acetylcysteine (mucolytic): For mucus filaments and early plaque formation
Steroid-Refractory / Steroid-Sparing
- Topical cyclosporin 0.05–2% (2–6 times daily) — effective steroid-sparing agent; takes weeks to act; irritation common
- Topical tacrolimus 0.1% ointment — particularly useful for shield ulcers and corneal epitheliopathy; can be used without steroids
- Supratarsal steroid injection: 0.1 mL triamcinolone 40 mg/mL or betamethasone 4 mg/mL into everted upper eyelid — for severe palpebral disease or non-compliant patients
Systemic
- Oral antihistamines (loratadine, cetirizine): reduce itching and nocturnal eye rubbing
- ⚠️ Aspirin — traditionally used in VKC but contraindicated in patients <16 years (Reye syndrome risk)
- Allergen desensitization in selected cases
Step 3: Management of Corneal Complications
| Complication | Management |
|---|---|
| Shield ulcer / plaque | Superficial keratectomy (debridement); maintain topical anti-inflammatories until re-epithelialization |
| Persistent epithelial defect | Amniotic membrane grafting; lubricants; botulinum-induced ptosis (tarsorrhaphy) if severe |
| Keratoconus (from chronic rubbing) | Rigid contact lens; corneal collagen cross-linking |
| Subepithelial scarring | If affecting visual axis: optical correction; consider excimer laser PTK |
Step 4: Optical Correction
- Both eyes have reduced VA (RE 6/18, LE 6/12)
- Perform refraction — VKC-associated irregular astigmatism (especially if keratoconus developing) or irregular corneal surface from scarring/vascularization reduces VA
- Consider spectacles/RGP lenses once inflammation is controlled
Follow-up
- Next 1–2 weeks to assess response to therapy; IOP monitoring if on steroids
- Reassess for disease activity, corneal complications, and vision monthly during active phase
- Long-term: disease typically remits by late teens in 95% of cases
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 198–202 | The Wills Eye Manual, 8th ed.
Recent evidence: A 2023 systematic review on VKC management confirms the above approach (PMID 37658939).
This is a shared conversation. Sign in to Orris to start your own chat.