Hill's sach and bankiart lession
Reading File
Finding Sources
Searching Images
Hill-Sachs lesion Bankart lesion shoulder dislocation
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information. Let me compile a thorough answer.
Hill-Sachs Lesion & Bankart Lesion
These two injuries are the classic "bipolar" bony/soft-tissue sequelae of anterior glenohumeral dislocation. They typically occur together and are pathognomonic for anterior shoulder instability.
Bankart Lesion
Definition
An avulsion of the anteroinferior glenoid labrum from the glenoid rim, originally identified by Bankart as "the essential lesion" creating shoulder instability. — Rockwood & Green's Fractures in Adults, 10th ed.
Types
| Type | Description |
|---|---|
| Soft-tissue (classic) Bankart | Detachment of the fibrocartilaginous labrum + tear of the glenoid periosteum from the anteroinferior glenoid rim |
| Bony (osseous) Bankart | Avulsion fracture with a bone fragment carrying the attached capsulolabral structures off the anterior glenoid rim |
Epidemiology of Glenoid Bone Loss
- Present in 40% of first dislocations, and 85% of recurrent dislocations
- Significant bone loss = >20–25% of glenoid width (~6–8 mm) — associated with higher recurrence rates after Bankart repair (recurrence rate jumps from 4% to 67%) — Miller's Review of Orthopaedics, 9th ed.
- Bone fragments in bony Bankart lesions undergo rapid absorption within 1 year of injury
Hill-Sachs Lesion
Definition
An impaction fracture of the posterolateral humeral head caused by forceful impact against the harder glenoid rim during anterior dislocation. Named after the two radiologists who first described it. — Miller's Review of Orthopaedics, 9th ed.
Incidence
- 40% of patients with recurrent subluxations (no frank dislocation)
- 90% of first-time dislocations
- Nearly 100% of recurrent dislocations
Engaging vs. Non-Engaging
- An engaging Hill-Sachs lesion is oriented such that, when the shoulder is placed in abduction + external rotation, the defect engages the anterior glenoid rim — causing the humeral head to slip off the glenoid → recurrent instability
On-Track vs. Off-Track Concept (Bipolar Bone Loss)
This newer concept evaluates the combined effect of glenoid and humeral bone loss to predict failure risk:
Glenoid Track = 0.84 × glenoid diameter Hill-Sachs Interval = distance from rotator cuff footprint to medial margin of the Hill-Sachs lesion
- On-track: Hill-Sachs interval ≤ glenoid track → low failure risk → arthroscopic Bankart repair alone is appropriate
- Off-track: Hill-Sachs interval > glenoid track → high recurrence risk → requires remplissage (filling in the Hill-Sachs defect) or Latarjet procedure (bone block to glenoid)
Reversed Lesions (Posterior Dislocation)
- Reverse Hill-Sachs lesion (also called McLaughlin lesion): impaction fracture on the anterior humeral head
- Reverse Bankart: fracture/labral tear at the posterior glenoid rim
MRI Appearance
The axial MR arthrogram below shows both lesions together — the classic "kissing lesions":
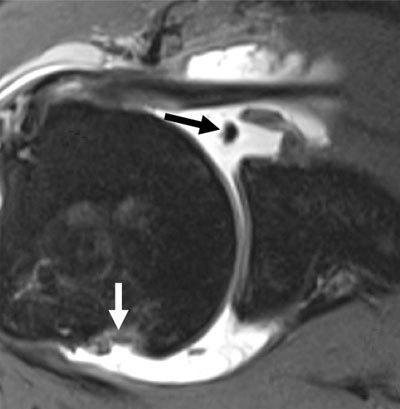
Axial MR arthrogram: black arrow = Hill-Sachs impaction defect on posterolateral humeral head; white arrow = soft-tissue Bankart lesion with labral detachment at anteroinferior glenoid. Intra-articular contrast accentuates the labral discontinuity.
Imaging Summary
| Modality | Finding |
|---|---|
| X-ray (Stryker notch view) | Hill-Sachs deformity |
| X-ray (West Point / Didiée view) | Glenoid rim / Bankart fracture |
| CT with 3D reconstruction | Best for quantifying bone loss; glenoid defect sizing for surgical planning |
| MRI arthrogram ± ABER view | Best for labral (soft-tissue Bankart) and cartilaginous Hill-Sachs; ABER increases sensitivity |
Recurrence Risk After First Dislocation
| Age Group | Redislocation Rate |
|---|---|
| Open physes | ~100% |
| <20 years | 70–95% |
| 20–30 years | 60–80% |
| >40 years | 15–20% |
Treatment Principles
- Arthroscopic Bankart repair (ABR): Standard for soft-tissue lesions with adequate bone stock (on-track)
- Remplissage: Arthroscopic procedure that fills the Hill-Sachs defect with posterior capsule/infraspinatus tendon — for off-track lesions
- Latarjet procedure: Coracoid transfer to the anterior glenoid — for >25% glenoid bone loss or off-track lesions
- Bipolar lesions: Prevalence rises from 33% (primary instability) to 62% (recurrent instability); postoperative recurrence is 29% when both lesions are present — Rockwood & Green's Fractures in Adults, 10th ed.
Physiotherapy for the same
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent — I now have detailed phase-by-phase rehabilitation data directly from the textbooks. Let me compile a comprehensive answer.
Physiotherapy for Hill-Sachs & Bankart Lesion (Anterior Shoulder Instability)
Rehabilitation is structured differently depending on whether management is conservative or post-operative.
Conservative (Non-Surgical) Physiotherapy
Who qualifies for conservative management?
- Primary dislocation in patients under 14 years — physical therapy + rotator cuff/deltoid strengthening
- Low-demand patients over 30 years — physical therapy is treatment of choice
- Active patients aged 14–30 without a Bankart lesion on MRI arthrogram — trial of PT + strengthening
- Multidirectional instability (AMBRII) — rehabilitation is the first-line treatment, focusing on rotator cuff and deltoid strengthening before considering surgery — Rockwood & Green's Fractures in Adults, 10th ed.
Surgery is indicated for patients who have recurrence of instability after a trial of physical therapy.
Post-Reduction Protocol
| Timeframe | Action |
|---|---|
| Immediately after reduction | Sling immobilization (sling and swathe bandage) |
| Duration of immobilization | Individualised by age and instability type |
| Younger patients (<30 yrs) | Longer immobilization beneficial (capsular stiffening reduces recurrence) |
| Older patients (>50 yrs) | Early ROM exercises to prevent adhesive capsulitis |
"The most important post-reduction therapy is a rehabilitation program aimed at restoring the static and dynamic stabilizers of the GHJ." — Rosen's Emergency Medicine
Goals of Conservative Physiotherapy
1. Restore Static Stabilizers
- Posterior capsule stretching (if tight)
- Avoid excessive anterior capsule stretching
2. Restore Dynamic Stabilizers (Core of rehab)
- Rotator cuff strengthening — subscapularis (primary dynamic anterior stabilizer), infraspinatus, teres minor, supraspinatus
- Deltoid strengthening — provides superior compressive force
- Periscapular muscle strengthening — trapezius, serratus anterior, rhomboids (for scapular control)
3. Neuromuscular / Proprioceptive Training
- Closed kinetic chain exercises (wall push-ups, quadruped rhythmic stabilization)
- Joint position sense retraining
- Perturbation training
Post-Operative Physiotherapy (After Bankart Repair or Latarjet)
After arthroscopic or open Bankart repair / Latarjet procedure, the patient is placed in a sling with abduction pillow for 4–6 weeks. Formal physical therapy begins 2 weeks post-surgery. — Rockwood & Green's Fractures in Adults, 10th ed.
Phase I — Weeks 0–4 (Protection Phase)
Goals: Pain/edema control, protect repair, initiate gentle ROM
- Sling with abduction pillow
- Passive ROM (supine):
- Forward flexion → goal 90°
- External rotation → goal 25°
- Elbow and wrist active + passive ROM
- Modalities: ice, TENS, ultrasound for pain and edema control
- No active shoulder movement
- Scapular retraction exercises (pain-free)
Phase II — Weeks 4–8 (Active Assisted ROM Phase)
Goals: Wean from sling, increase ROM, begin muscle activation
- Gradually wean from sling
- Transition passive ROM → active assisted ROM
- Forward flexion → goal 120°
- External rotation progressed carefully
- Begin submaximal isometric rotator cuff exercises
- Pendulum exercises
- Scapular stabilization exercises
- Closed kinetic chain exercises (wall slides)
- Hydrotherapy if available
Phase III — Weeks 8–14 (Active ROM / Early Strengthening Phase)
Goals: Restore full ROM, begin progressive strengthening
- Restore full ROM in flexion and external rotation
- Begin isotonic rotator cuff strengthening:
- Internal rotation (subscapularis)
- External rotation (infraspinatus, teres minor)
- Abduction, scaption (supraspinatus)
- Periscapular strengthening (rows, lat pulldowns)
- Proprioceptive neuromuscular facilitation (PNF) patterns
- Progress to light resistance band exercises
Phase IV — Weeks 14–22 (Advanced Strengthening & Functional Phase)
Goals: Sport/activity-specific training, return to function
- Progressive resistance training
- Plyometric shoulder exercises (light ball throws, rhythmic stabilization)
- Sport-specific drills
- Overhead activity progression (if applicable)
- Return-to-sport criteria:
- Full pain-free ROM
- Strength symmetry ≥90% compared to contralateral side
- Negative apprehension/relocation test
- Satisfactory neuromuscular control
Phase V — Weeks 22+ (Return to Sport)
- Full unrestricted activity typically at 5–6 months post Bankart repair
- Contact athletes may require up to 9–12 months
- Maintenance strengthening program ongoing
Key Muscles to Target
| Muscle | Role in Stability |
|---|---|
| Subscapularis | Primary anterior dynamic stabilizer; resists anterior translation |
| Infraspinatus / Teres minor | External rotation force couple; posterior compression |
| Supraspinatus | Superior compression of humeral head into glenoid |
| Serratus anterior | Scapular protraction, upward rotation |
| Lower trapezius | Scapular depression and posterior tilt |
| Deltoid | Compressive humeral head force |
Special Considerations
| Scenario | PT Modification |
|---|---|
| Hill-Sachs + Remplissage | Restrict external rotation more strictly in early phases |
| Latarjet procedure | Earlier mobilization allowed as coracoid graft is more robust |
| Multidirectional instability (AMBRII) | Emphasis on all directions of rotator cuff + deltoid; avoid large ROM stretching |
| Axillary nerve injury | Address deltoid weakness specifically; monitor recovery |
| Older patient (>50 yrs) | Aggressive early ROM to prevent frozen shoulder |
Immobilization Position — A Note
- Traditional position: internal rotation sling
- Newer evidence: external rotation bracing showed initial promise in reducing redislocation by keeping subscapularis taut and reducing strain on anterior capsule — however, meta-analyses show no definitive difference between IR and ER immobilization — Miller's Review of Orthopaedics, 9th ed.
Sources: Rockwood & Green's Fractures in Adults, 10th ed. | Miller's Review of Orthopaedics, 9th ed. | Rosen's Emergency Medicine
Osteoarthritis
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.