Chronic eczema management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content to deliver a thorough, well-structured answer on chronic eczema management.
Chronic Eczema (Atopic Dermatitis) Management
Chronic eczema/atopic dermatitis (AD) is managed through a proactive, stepwise strategy — not just reactive treatment of flares. The goal is to control subclinical inflammation, prevent recurrence, and modify overall disease course.
Management Plan Overview
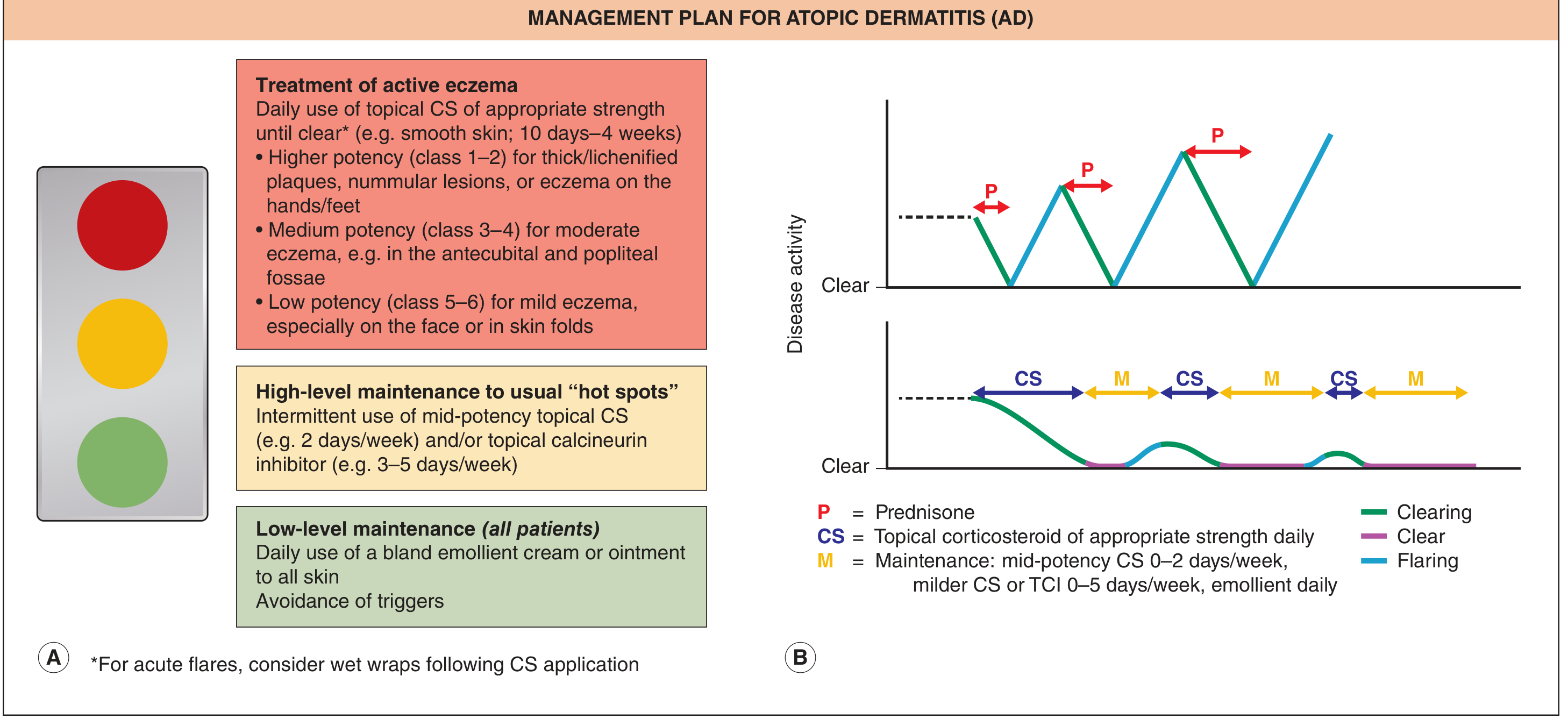
Fig. 12.22 — Dermatology 2-Volume Set 5e
The three-tier framework (traffic-light model):
| Tier | Action |
|---|---|
| Red (active disease) | Daily topical corticosteroid (TCS) of appropriate potency until clear (10 days–4 weeks); wet wraps for acute flares |
| Yellow (hot-spot maintenance) | Intermittent mid-potency TCS 2×/week and/or topical calcineurin inhibitor (TCI) 3–5×/week |
| Green (baseline — all patients) | Daily emollient to all skin + trigger avoidance |
1. Patient Education
Education is a cornerstone of management and has been shown to improve outcomes. Key elements:
- Disease mechanism, course, and triggers
- Correct use of topical therapies
- Goals of management (control, not cure)
- Written action plans
- Psychological support: cognitive-behavioral therapy, biofeedback, stress management
Resources such as structured "eczema school" programs and patient portals (e.g., nationaleczema.org) improve adherence.
— Dermatology 2-Volume Set 5e, p. 264
2. Skin Care Basics
Bathing: Lukewarm baths/showers followed immediately by moisturizer application ("soak and seal"). Harsh soaps should be avoided; gentle, fragrance-free cleansers preferred.
Emollients: Daily application of bland emollient cream or ointment to all skin — the foundation of all AD management regardless of disease activity.
Trigger avoidance: Common triggers include:
- Irritants (soaps, detergents, wool, sweat)
- Aeroallergens (dust mites, pet dander, pollens)
- Foods (especially in children — eggs, milk, peanuts, wheat)
- Stress, temperature extremes
- Secondary infections (S. aureus, HSV)
3. Topical Anti-inflammatory Therapy
Topical Corticosteroids (TCS) — First-line
Potency selection is site- and severity-dependent:
| Potency | Use |
|---|---|
| Class 1–2 (high) | Thick/lichenified plaques, nummular lesions, hands/feet |
| Class 3–4 (medium) | Moderate eczema in antecubital/popliteal fossae |
| Class 5–6 (low) | Mild eczema; face and skin folds |
Apply daily until clear, then transition to maintenance (2×/week to the same "hot spots").
Topical Calcineurin Inhibitors (TCIs) — Steroid-sparing
- Tacrolimus ointment (0.03% for children, 0.1% for adults) and pimecrolimus cream — particularly useful for face, eyelids, and intertriginous areas where steroids carry atrophy risk
- Maintenance use 2–3×/week prevents flares without increasing total medication burden
- Main side effect: transient local stinging/burning, which diminishes with continued use
- No evidence of systemic immunosuppression; no confirmed cancer risk in clinical/post-marketing data (>15 years)
— Dermatology 2-Volume Set 5e
Crisaborole (PDE-4 inhibitor)
- 2% ointment, FDA-approved for mild-to-moderate AD ≥3 months of age
- ~30% achieve clear/almost clear skin after 4 weeks twice daily
- Side effect: application-site stinging
Topical JAK Inhibitors
- Ruxolitinib 1.5% cream (JAK1/2 inhibitor) — FDA-approved for short-term/non-continuous chronic treatment of mild-to-moderate AD in patients ≥12 years
- 50–55% achieve clear/almost clear skin at 8 weeks vs. 7–15% with vehicle
- Maximum use: ≤60 g/week
4. Systemic Therapy (Moderate–Severe Disease)
Phototherapy: Narrowband UVB is first-line systemic option; PUVA for refractory cases.
Biologics:
- Dupilumab (anti-IL-4Rα) — the most established biologic; blocks IL-4 and IL-13 signaling; approved for moderate-to-severe AD ≥6 months of age
- Tralokinumab, lebrikizumab (anti-IL-13)
- Increasingly used as maintenance therapy to reduce TCS dependence
Systemic JAK inhibitors (oral):
- Upadacitinib, abrocitinib (JAK1-selective) — approved for moderate-to-severe AD in adults/adolescents; faster itch relief than dupilumab in head-to-head trials
- Monitoring required: lipid panel, CBC, herpes zoster vaccination before initiation
Traditional immunosuppressants (second-line, off-label):
- Cyclosporine (rapid onset, short-term use)
- Methotrexate, azathioprine, mycophenolate mofetil (slower onset, longer-term options)
- Systemic corticosteroids only for short bridging; avoid long-term use due to rebound flares
5. Managing Comorbidities and Complications
- Secondary bacterial infection (S. aureus): topical mupirocin for localized; oral anti-staphylococcal antibiotics for widespread impetiginization
- Eczema herpeticum (HSV superinfection): systemic acyclovir/valacyclovir — treat promptly, especially in children
- Atopic march: screen for and co-manage asthma, allergic rhinitis, food allergy
- Prurigo nodularis in severe chronic disease: dupilumab or nemolizumab
6. Special Subtypes Relevant to Chronic Eczema
- Hand eczema: Alitretinoin (oral retinoid, not available in the US) can achieve complete or near-complete clearance in ~50% of chronic refractory cases — Andrews' Diseases of the Skin, p. 248
- Nummular eczema: High-potency TCS; exclude contact allergy
- Seborrheic dermatitis: Antifungal shampoos/creams (ketoconazole, ciclopirox), low-potency TCS
Summary Algorithm
All patients → Daily emollient + trigger avoidance
↓
Active flare → TCS (potency per site/severity) ± wet wraps
↓
Clearing → Step down to TCS 2×/week + TCI maintenance
↓
Inadequate control → Phototherapy → Biologics (dupilumab) or oral JAK inhibitors
↓
Severe/refractory → Specialist referral, cyclosporine bridging, clinical trials
The shift from reactive to proactive maintenance is the most important modern change in chronic eczema management — preventing sub-clinical inflammation between visible flares is as important as treating overt disease. — Dermatology 2-Volume Set 5e, p. 262
This is a shared conversation. Sign in to Orris to start your own chat.