Accessory navicular
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"accessory navicular" treatment outcomes
Loading Image
Loading Image
Here is a comprehensive overview of the accessory navicular:
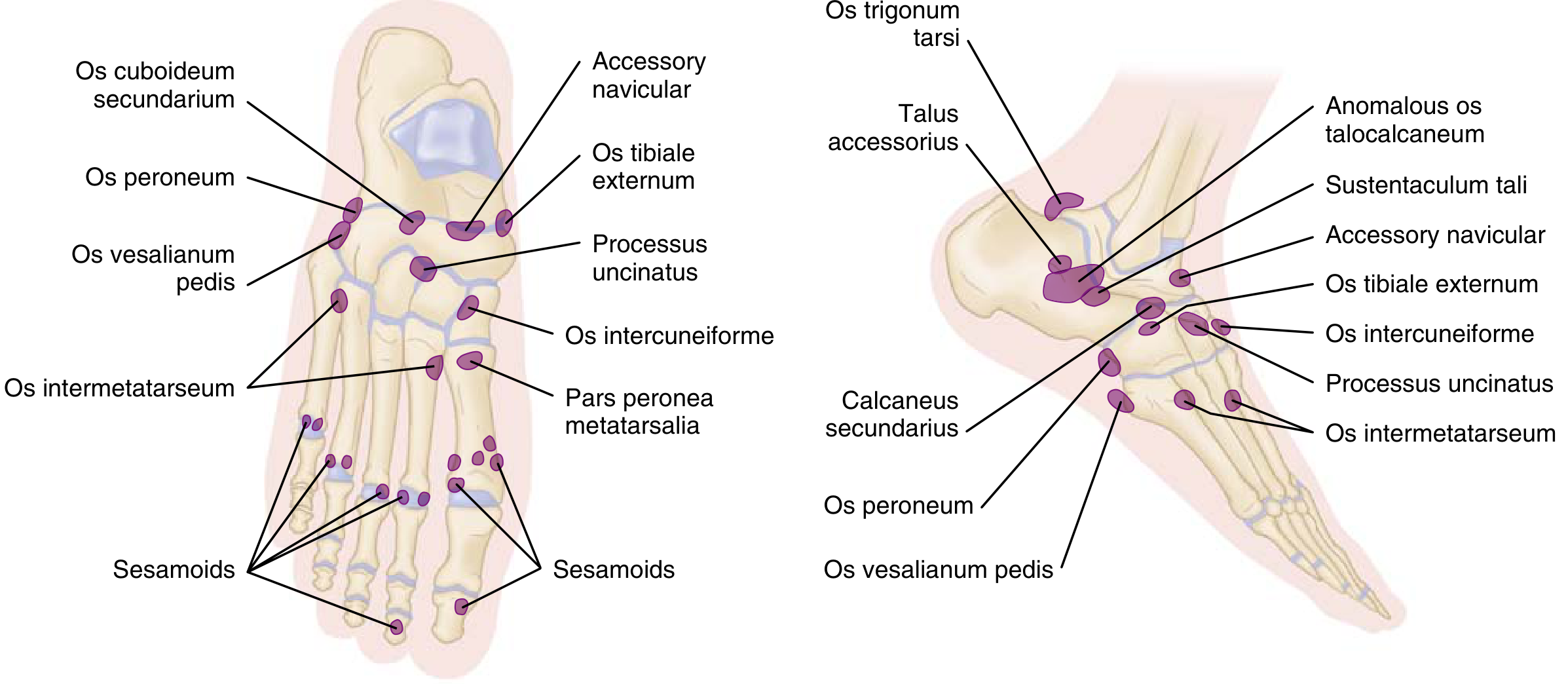
Accessory Navicular (Os Tibiale Externum)
Epidemiology & Anatomy
- Present in 10–14% of the normal population (some sources cite up to 12%)
- Located along the proximal/medial aspect of the navicular tuberosity, within the direct insertion of the tibialis posterior tendon
- Also called os tibiale externum
- ~50% of individuals with an accessory navicular have flexible flatfoot
Classification (3 Types)
| Type | Description |
|---|---|
| Type 1 | Small sesamoid-like ossicle, no articulation with navicular (likely a true sesamoid); incidental finding |
| Type 2 | Larger ossicle connected to the navicular tuberosity by a fibrous/fibrocartilaginous union (synchondrosis/syndesmosis); most symptomatic type — instability of the synchondrosis causes pain |
| Type 3 | Osseous fusion to the navicular, creating a "cornuate navicular"; may be prominent and cause shoe friction |
Clinical Features
- Typically presents with medial arch/midfoot pain aggravated by activity
- Tenderness and prominence over the medial navicular
- The posterior tibial tendon typically inserts into the accessory bone rather than the native navicular, which can alter biomechanics and contribute to flatfoot deformity
- Symptoms may be triggered by direct shoe pressure (Types 2 and 3) or synchondrosis stress/micro-instability (Type 2)
Imaging
- Weight-bearing foot X-rays are the primary modality; an external oblique (supination oblique) view is most helpful for demonstrating the accessory bone
- Type 1 on CT scan: small separate ossicle; Type 2 shows the articulation clearly on oblique radiograph
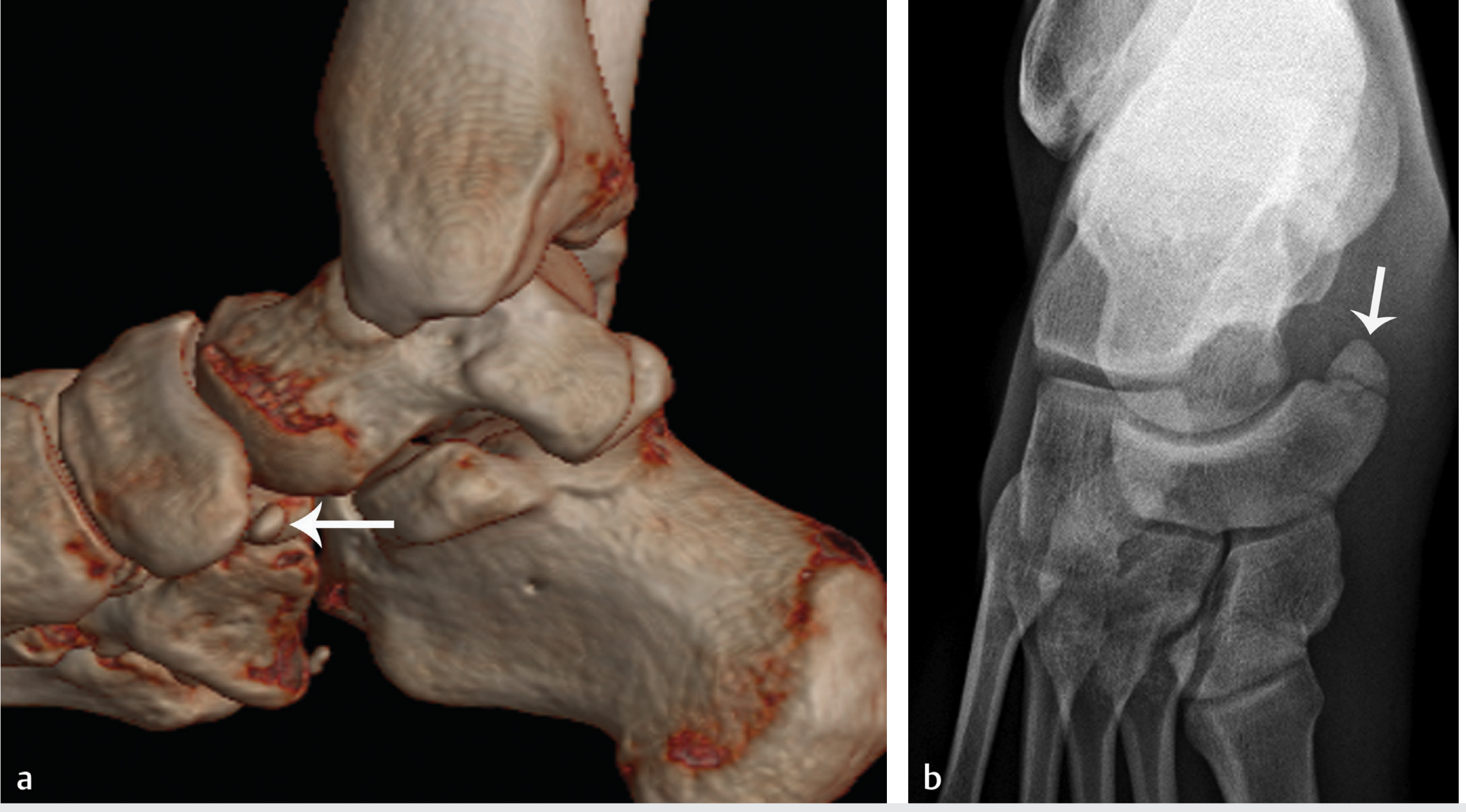
- MRI is useful when soft tissue assessment is needed (posterior tibial tendon integrity, synchondrosis edema, bone marrow edema)
Treatment
Conservative (First-line)
- Activity restriction and shoe modification (avoid pressure over the medial prominence)
- Orthosis — UCBL (University of California at Berkeley Laboratory) orthosis to control hindfoot valgus
- Short-leg cast immobilization for 4–6 weeks
- Most cases resolve spontaneously
Surgical (if conservative fails)
- Kidner procedure: excision of the accessory bone with repair and advancement of the posterior tibial tendon back to the native navicular
- In adolescents with flexible flatfoot, combined procedures (e.g., subtalar arthroereisis + Kidner procedure) have been studied — a 2025 systematic review and meta-analysis (PMID: 41137245) assessed efficacy of this combined approach
Key Differentials
- Navicular stress fracture — acute onset, different location; must not be confused on plain films
- Avulsion fracture of the navicular tuberosity
- Posterior tibial tendon dysfunction (may coexist)
Sources:
- Miller's Review of Orthopaedics, 9th Ed., pp. 244, 566
- Imaging Anatomy Text and Atlas, Vol. 3, pp. 839, 875
- Rosen's Emergency Medicine, block 8
This is a shared conversation. Sign in to Orris to start your own chat.