Hyponatremia
Reading File
Finding Sources
Searching PubMed
"hyponatremia"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to write a thorough answer. Let me compile everything.
Hyponatremia
Definition and Epidemiology
Hyponatremia is defined as a serum sodium concentration below 135 mmol/L, corresponding to a plasma osmolality <280 mOsm/kg H₂O. It is one of the most common electrolyte disorders in clinical practice - with an incidence of 15-30% in hospitalized patients using the <135 mmol/L threshold, and 1-4% using the more clinically significant <130-131 mmol/L threshold. In the non-hospitalized general population, prevalence is approximately 1.7%.
- Goldman-Cecil Medicine, p. 1201; Rosen's Emergency Medicine, p. 2519
Classification by Osmolality
| Type | Serum Na | Plasma Osmolality | Cause |
|---|---|---|---|
| Hypo-osmolar | <135 | Low (<280) | Volume depletion (true/effective) |
| Iso-osmolar | <135 | Normal (280-295) | Hyperlipidemia, paraproteinemia, hyperglycemia, alcohols - pseudohyponatremia |
| Hyper-osmolar | <135 | High (>295) | Hyperglycemia, mannitol, severe dehydration |
- Goldman-Cecil Medicine, Table 102-5
Pathophysiology
In every case of hypo-osmolar hyponatremia, free water intake exceeds output, renal free water excretion is impaired, or both. The kidney dilutes urine by reabsorbing sodium in segments with low water permeability (thick ascending limb of Henle, distal tubule, collecting tubules). ADH (vasopressin/AVP) governs water permeability of collecting ducts - excess ADH is central to most causes.
When neurons are subjected to a hyponatremic environment, they lose sodium and potassium to limit intracellular osmolality and prevent cell swelling. This adaptation takes 24-48 hours and explains why chronic hyponatremia is better tolerated than acute - but also why rapid correction is dangerous.
- Goldman-Cecil Medicine, p. 1201; Rosen's Emergency Medicine, p. 2520
Classification by Volume Status
1. Hypovolemic Hyponatremia
- Decreased total body water and sodium, with relatively greater sodium loss
- Non-renal causes (urine Na <20 mEq/L): vomiting, diarrhea, sweating, GI suction, third-spacing (burns, pancreatitis, bowel obstruction)
- Renal causes (urine Na >20 mEq/L): thiazide diuretics, mineralocorticoid deficiency, osmotic diuresis, renal tubular acidosis, salt-wasting nephropathy
Note on thiazides: Thiazides are 12-fold more likely than loop diuretics to cause hyponatremia. They inhibit urinary dilution (loop diuretics inhibit both dilution and concentration). ~80% of thiazide-induced hyponatremia occurs in older females with low body mass and typically develops in the first 2 weeks of therapy.
2. Euvolemic Hyponatremia
- Increased total body water with near-normal total body sodium
- SIADH (most common)
- Drugs causing SIADH: diuretics, carbamazepine, chlorpropamide, scopolamine, opioids, vincristine, cyclophosphamide, cisplatin, SSRIs, antipsychotics, desmopressin, MDMA
- Psychogenic polydipsia
- Beer potomania
- Hypothyroidism
- Adrenal insufficiency
- Postoperative state
3. Hypervolemic Hyponatremia
-
Increased total body sodium with relatively greater total body water increase
-
Heart failure (urine Na <20 mEq/L - renal hypoperfusion)
-
Cirrhosis/hepatic failure (urine Na <20 mEq/L)
-
Chronic renal failure (urine Na >20 mEq/L)
-
Nephrotic syndrome
-
Rosen's Emergency Medicine, Box 114.5 and Table 114.3
SIADH - Diagnostic Criteria
| Criterion |
|---|
| Hypotonic hyponatremia (P |
| Inappropriately elevated urine osmolality (usually >200 mOsm/kg) |
| Elevated urine Na⁺ (typically >20 mEq/L) |
| Clinical euvolemia |
| Normal adrenal, renal, cardiac, hepatic, and thyroid function |
Causes of SIADH:
-
Pulmonary: Pneumonia, TB, lung abscess, aspergillosis, positive pressure ventilation, acute respiratory failure
-
CNS: Brain tumor, encephalitis, meningitis, subarachnoid hemorrhage, head injury, Guillain-Barré
-
Malignancy: Small cell lung cancer (10-15% of cases - most common paraneoplastic cause), head and neck tumors, CNS tumors
-
Drugs: AVP analogs (desmopressin), chemotherapy (cyclophosphamide, cisplatin, vincristine, vinblastine), carbamazepine, antipsychotics, antidepressants, opiates, nicotine, MDMA
-
Tintinalli's Emergency Medicine, Table 17-6; Goldman-Cecil Medicine, p. 1202
Urine Studies for Diagnosis
| Urine Na | Scenario |
|---|---|
| <20 mEq/L | Hypovolemic (non-renal loss): diarrhea, vomiting, sweating |
| <20 mEq/L | Hypervolemic (CHF, cirrhosis) - renal hypoperfusion |
| >20 mEq/L | Hypovolemic (renal loss): diuretics, salt-wasting |
| >20 mEq/L | Euvolemic (SIADH, endocrinopathies) - volume expansion |
| >20 mEq/L | Hypervolemic - renal failure |
| <20 mEq/L | Psychogenic polydipsia - maximally dilute urine |
- Rosen's Emergency Medicine, Table 114.3
Clinical Manifestations
Symptoms depend on duration, severity, and rate of development:
- Mild-moderate: Headache, nausea, vomiting, malaise, lethargy, confusion
- Severe/acute: Seizures, decreased consciousness, coma, respiratory arrest, brain herniation
- Most patients presenting to the ED are asymptomatic
- Hyponatremia in cancer patients doubles length of stay and increases 90-day mortality 3-5 fold
Most patients with chronic hyponatremia are asymptomatic unless serum Na <125 mmol/L because of cerebral adaptation (electrolyte and organic osmolyte loss from neurons).
- Rosen's Emergency Medicine, p. 2520; Brenner & Rector's The Kidney
Treatment
General Principles
Treatment is guided by four variables:
- Severity of symptoms (most important)
- Rate of onset (acute <48h vs. chronic >48h)
- Volume status
- Current serum Na
When duration is unknown, assume chronic and treat accordingly.
Acute Symptomatic Hyponatremia (Seizures, Coma, Herniation Risk)
3% Hypertonic Saline Protocol (European guidelines / US expert consensus):
| Step | Action |
|---|---|
| 1 | Infuse 100-150 mL of 3% NaCl IV over 10-20 minutes |
| 2 | Measure serum Na after each infusion |
| 3 | Stop when symptoms improve or Na rises by 4-6 mEq/L |
| 4 | May repeat up to 3 total doses (max 450 mL total) |
| 5 | Limit total correction to ≤8-12 mEq/L in first 24h; ≤18 mEq/L in 48h |
A rise of only 5 mEq/L is typically sufficient to improve severe neurologic symptoms and prevent herniation.
- Tintinalli's Emergency Medicine, Table 17-7; Goldman-Cecil Medicine, p. 1203
Chronic Hyponatremia - Correction Rate Limits
| Risk Level | Max correction / 24h | Max correction / 48h |
|---|---|---|
| High risk for ODS* | ≤4-6 mEq/L/day | - |
| High risk for ODS | ≤8 mEq/L | - |
| Normal risk | ≤10-12 mEq/L | ≤18 mEq/L |
| High-risk patients (cancer) | ≤6-8 mEq/L/day | - |
*High risk for osmotic demyelination syndrome (ODS): serum Na <120 mmol/L of >48h duration, chronic thiazide use, hospital-acquired hyponatremia of known >48h duration, alcoholism, cirrhosis, malnutrition, hypokalemia.
By Volume Status
| Volume Status | Treatment |
|---|---|
| Hypovolemic | Isotonic (0.9%) NaCl to restore volume; correct underlying cause |
| Euvolemic (SIADH) | Fluid restriction (500 mL less than urine output); treat underlying cause; salt tablets; loop diuretics + oral NaCl; vaptans |
| Hypervolemic (HF, cirrhosis) | Treat underlying condition; loop diuretics; fluid restriction; vaptans (tolvaptan for SIADH, heart failure) |
Chronic SIADH - Specific Options
- Fluid restriction - first-line (typically restrict to 500 mL less than daily urine output)
- Urea - oral urea 15-60 g/day is effective and cheap; a recent systematic review (Am J Kidney Dis, 2025) confirmed its efficacy for SIADH-related hyponatremia
- Vaptans (tolvaptan, conivaptan) - V2 receptor antagonists; block ADH action in collecting duct; use with caution (risk of overcorrection); contraindicated in liver disease (tolvaptan)
- Demeclocycline - causes nephrogenic DI; less commonly used due to nephrotoxicity
Osmotic Demyelination Syndrome (ODS)
Mechanism: Rapid correction raises extracellular Na too quickly - water shifts out of neurons (which have already lost organic osmolytes) - causing pontine and extrapontine demyelination.
Risk factors: Na <120 mEq/L, alcoholism, cirrhosis, malnutrition, hypokalemia, chronic duration, vasopressin antagonists.
Symptoms: Dysarthria, dysphagia, lethargy, paraparesis/quadriparesis, seizures, coma - often delayed 2-6 days after correction.
If overcorrection occurs: Administer D5W at 3 mL/kg/h + loop diuretics + desmopressin to lower serum Na back to the recommended level. This re-lowering intervention is important if starting Na was <120 mmol/L.
- Tintinalli's Emergency Medicine, p. 127; Goldman-Cecil Medicine, p. 1203
Recent Evidence (2025)
- A JAMA Internal Medicine systematic review and meta-analysis (2025) examined correction rates and clinical outcomes in hospitalized adults with severe hyponatremia - one of the most comprehensive recent analyses of this topic (PMID 39556338)
- A systematic review of urea for SIADH (Am J Kidney Dis, 2025) confirms urea as an effective treatment option (PMID 39362395)
- A systematic review of beer potomania (Nutrients, 2025) characterizes this low-solute hyponatremia variant (PMID 40573123)
Quick Reference: Infusate Sodium Content
| Infusate | Na (mmol/L) |
|---|---|
| 3% Hypertonic saline | 513 |
| 0.9% Normal saline | 154 |
| Lactated Ringer's | 130 |
| 0.45% Half-normal saline | 77 |
| D5W | 0 |
- Rosen's Emergency Medicine, Table 114.4
Hypocalcemia workup
Finding Sources
Searching PubMed
"hypocalcemia"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Both diagnostic flowcharts are excellent. I now have everything needed for a comprehensive answer.
Hypocalcemia Workup
Definition
| Measure | Threshold |
|---|---|
| Total serum calcium | <8.5 mg/dL (<2.12 mmol/L) |
| Ionized (free) calcium | <4.65 mg/dL (<1.16 mmol/L) |
| Mild hypocalcemia | Total Ca 8.0-8.5 mg/dL |
| Severe hypocalcemia | Total Ca <7.6 mg/dL (<1.9 mmol/L) |
| Neonates | <8 mg/dL |
| Preterm infants | <7 mg/dL |
- Goldman-Cecil Medicine, p. 2645; Brenner & Rector's The Kidney
Step 1 - Confirm True Hypocalcemia (Rule Out Pseudohypocalcemia)
Most common artifactual cause: hypoalbuminemia
Calcium is ~50% protein-bound (mainly albumin), ~10% complexed to anions, and ~40% ionized (active).
Correction formula:
Corrected Ca = Measured Ca + 0.8 × (4.0 - serum albumin in g/dL)
- For every 1 g/dL fall in serum albumin, measured total calcium falls ~0.8 mg/dL, but ionized calcium is unaffected
- Seen in: cirrhosis, nephrotic syndrome, malnutrition, sepsis
- If albumin is low: measure ionized (free) calcium directly to confirm true hypocalcemia
Other causes of false hypocalcemia: freezing/thawing of specimens, hemodialysis patients (plasma sample artifact)
Also note: alkalosis shifts calcium to the bound form, lowering ionized Ca without affecting total Ca - important in hyperventilating patients.
- Rosen's Emergency Medicine, p. 2703; Brenner & Rector's The Kidney
Diagnostic Algorithm
Goldman-Cecil Flowchart (Adults)
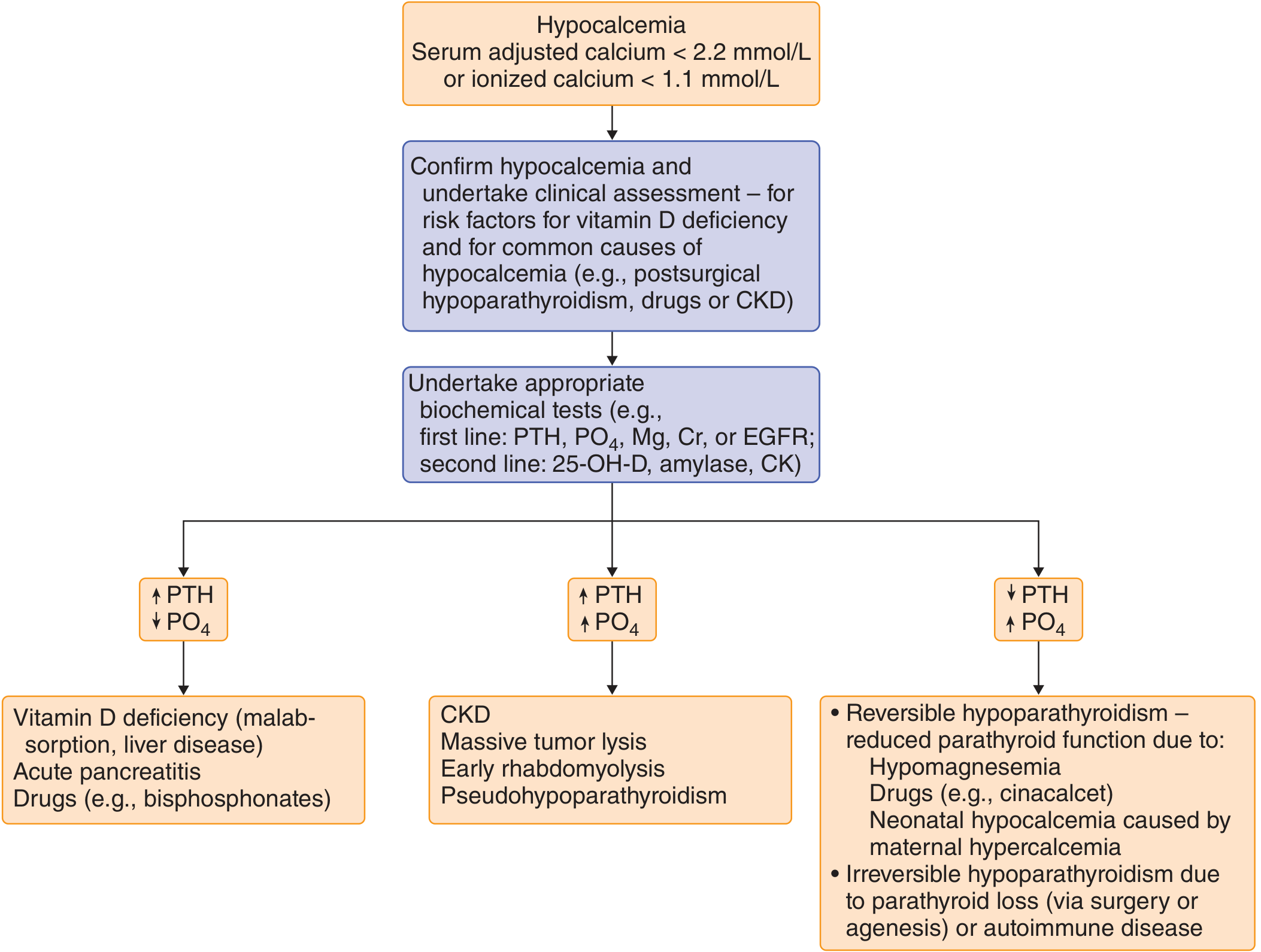
Goldman-Cecil Medicine - Clinical approach to hypocalcemia investigation
Brenner & Rector Flowchart (Neonates/Children and Adults)
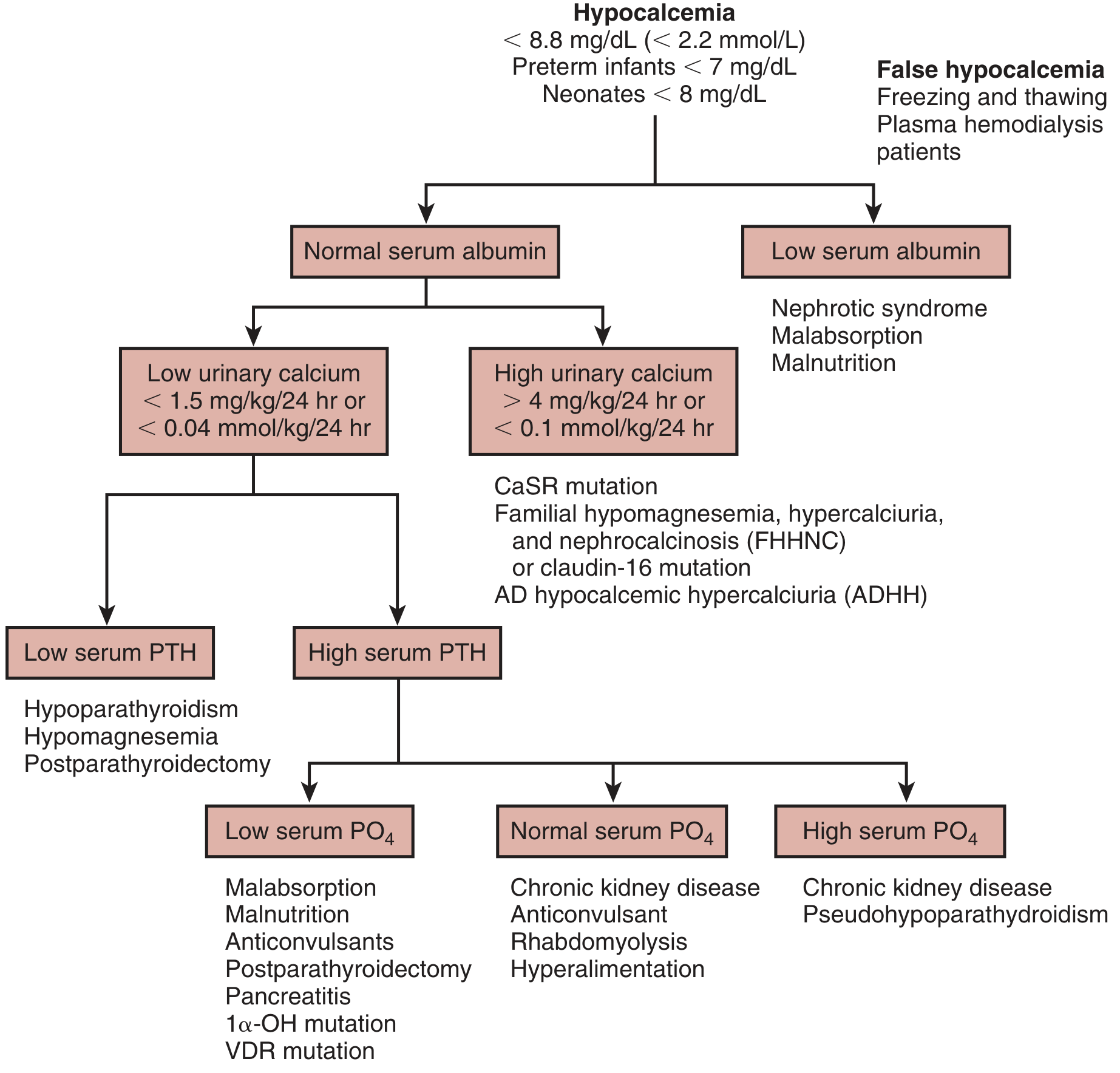
Brenner & Rector's The Kidney - Algorithm for diagnosis of hypocalcemia
Step 2 - First-Line Labs
| Test | Why |
|---|---|
| PTH (intact) | Central branch point of workup |
| Serum phosphate (PO4) | Distinguishes causes once PTH is known |
| Serum magnesium (Mg) | Hypomagnesemia blocks PTH secretion AND action |
| Creatinine / eGFR | Chronic kidney disease is the most common cause |
| Serum albumin | Rule out pseudohypocalcemia |
| Spot urine Ca:Cr ratio | Distinguish hypocalciuria from hypercalciuria |
Step 3 - Second-Line Labs (Based on First Results)
| Test | Indication |
|---|---|
| 25-OH-D (25-hydroxyvitamin D) | If PTH elevated + low PO4 - vitamin D deficiency suspected |
| 1,25-(OH)₂D (calcitriol) | If CKD confirmed (will be low) or vitamin D resistance suspected |
| Amylase/lipase | If acute pancreatitis suspected |
| CK (creatine kinase) | If rhabdomyolysis suspected |
| Serum/urine protein electrophoresis | If paraproteinemia considered |
| 24-hr urine calcium | To quantify hypocalciuria vs. hypercalciuria |
| PTHrP | If malignancy suspected |
Step 4 - Interpret PTH + Phosphate Pattern
Low PTH + High Phosphate = Hypoparathyroidism
PTH is low or undetectable despite hypocalcemia - parathyroid gland failure or suppression.
Causes:
- Post-surgical (most common acquired) - after thyroidectomy (1-2%), parathyroidectomy, or radical neck dissection
- Autoimmune - isolated or as part of autoimmune polyglandular syndrome (APS-1: hypoparathyroidism + Addison's + mucocutaneous candidiasis)
- Genetic/hereditary - DiGeorge syndrome (22q11 deletion - absent parathyroid + thymus), familial isolated hypoparathyroidism (PTH gene mutations), Kenny-Caffey syndrome, Sanjad-Sakati syndrome
- Activating mutations of calcium-sensing receptor (CaSR) - receptor is hypersensitive, suppresses PTH at normal or low Ca levels (autosomal dominant hypocalcemia)
- Infiltrative - iron overload (hemochromatosis, thalassemia), copper deposition (Wilson's), granulomas, metastatic tumor
- Toxic - high-dose radiation, asparaginase, ethiofos
- Hypomagnesemia - reversible; profound hypoMg impairs PTH secretion AND end-organ response; must correct Mg first or hypocalcemia will not respond to treatment
- Neonatal - caused by maternal hypercalcemia (suppresses fetal PTH), prematurity, diabetic mothers, asphyxia, citrated blood transfusions
High PTH + Low Phosphate = Secondary Hyperparathyroidism with Vitamin D-Related Causes
PTH is appropriately elevated (compensating) but calcium remains low - inadequate vitamin D-mediated intestinal Ca absorption or Ca loss.
Causes:
- Vitamin D deficiency - inadequate sunlight, poor dietary intake, malabsorption (celiac disease, Crohn's, post-bariatric surgery, pancreatic insufficiency), liver disease (impaired 25-hydroxylation), check 25-OH-D
- 1α-hydroxylase deficiency (Vitamin D-dependent rickets type 1) - 25-OH-D normal, 1,25-(OH)₂D low
- Vitamin D receptor defects (VDR mutation / Vitamin D-dependent rickets type 2) - 25-OH-D normal, 1,25-(OH)₂D markedly elevated
- Acute pancreatitis - saponification of calcium in peripancreatic fat
- Drugs inhibiting vitamin D metabolism - anticonvulsants (phenytoin, phenobarbital), rifampin
- Malnutrition, malabsorption, post-parathyroidectomy "hungry bone syndrome"
High PTH + High Phosphate = CKD or Pseudohypoparathyroidism
- Chronic kidney disease (most common overall cause of hypocalcemia) - reduced 1α-hydroxylase activity → low 1,25-(OH)₂D → reduced intestinal Ca absorption; phosphate retention; labs: high Cr, high PO4, high PTH, high alkaline phosphatase, normal 25-OH-D, low 1,25-(OH)₂D
- Pseudohypoparathyroidism (PHP / Albright hereditary osteodystrophy) - PTH markedly elevated, end-organ resistance (defect in Gαs subunit of adenylate cyclase); PTH infusion → subnormal urine cAMP and phosphaturia response; phenotype: round face, short stature, brachydactyly, subcutaneous calcifications, mental retardation
- Massive tumor lysis syndrome - massive phosphate release complexes calcium
- Early rhabdomyolysis - phosphate release from muscle
High PTH + High Urinary Calcium = Hypercalciuric Conditions
- Activating CaSR mutation / familial hypocalcemia with hypercalciuria (ADHH)
- Familial hypomagnesemia with hypercalciuria and nephrocalcinosis (FHHNC / claudin-16 mutations)
Acute/Other Causes
- Acute pancreatitis - calcium soap deposition in retroperitoneum
- Massive blood transfusion - citrate chelates ionized Ca
- Drugs: heparin, glucagon, protamine, bisphosphonates, cinacalcet, foscarnet, denosumab
- Sepsis, burns, critical illness - multifactorial
- HIV/AIDS - medication effects + infiltration
- Osteoblastic metastases (e.g., prostate, breast) - increased bone uptake
- Hungry bone syndrome post-parathyroidectomy - bone avidly takes up calcium
Lab Pattern Summary Table
| Cause | PTH | PO4 | Mg | 25-OH-D | 1,25-(OH)₂D | Cr |
|---|---|---|---|---|---|---|
| Hypoparathyroidism (surgical/autoimmune) | ↓/absent | ↑ | N | N | Low (lack of PTH) | N |
| Hypomagnesemia | ↓ (functional) | N/↑ | ↓↓ | N | N | N |
| CKD | ↑ | ↑ | N/↓ | N | ↓↓ | ↑↑ |
| Vitamin D deficiency | ↑ | ↓ | N | ↓↓ | ↓ | N |
| Vit D-dep rickets type 1 (1α-OHase def) | ↑ | ↓ | N | N | ↓↓ | N |
| Vit D-dep rickets type 2 (VDR mutation) | ↑ | ↓ | N | N | ↑↑ | N |
| Pseudohypoparathyroidism | ↑↑ | ↑ | N | N | Low | N |
| Acute pancreatitis | ↑ | ↑/N | N | N | N | N/↑ |
| Hypoalbuminemia (pseudohypocalcemia) | N | N | N | N | N | N |
Clinical Features to Guide Workup
Symptoms of neuromuscular irritability (severity correlates with ionized Ca and rate of fall):
- Perioral, fingertip, and toe paresthesias
- Muscle cramps, carpopedal spasm, tetany
- Chvostek sign - tap facial nerve anterior to ear → circumoral/facial twitching (present in ~10% of normals - less specific)
- Trousseau sign - inflate BP cuff 20 mmHg above systolic for 3 minutes → carpal spasm (more specific)
- Seizures (focal, grand mal, or syncope)
- Prolonged QT interval, ST-T changes, ventricular arrhythmias, cardiac failure
- Laryngospasm, bronchospasm
Chronic hypocalcemia features (suggest hypoparathyroidism or long-standing disease):
-
Cataracts (subcapsular)
-
Basal ganglia calcifications (extrapyramidal signs: choreoathetosis, dystonia)
-
Papilledema, increased intracranial pressure
-
Poor dentition, enamel hypoplasia
-
Dry skin, coarse hair, alopecia, pruritus, nail changes
-
Candidiasis (APS-1)
-
Goldman-Cecil Medicine, Table 227-7; Rosen's Emergency Medicine, p. 2697-2699; Henry's Clinical Diagnosis, p. 254
Treatment (Brief Summary)
Acute Symptomatic (Seizures, Tetany, QT Prolongation)
- IV Calcium gluconate 10%: 10 mL (93 mg elemental Ca) over >5 minutes, repeat as needed
- Follow with infusion: 10 ampules calcium gluconate in 1L D5W or NS, start at 50 mL/hr, titrate; 1.2-1.6 mg/kg elemental Ca over 4-6 hours raises Ca by 2-3 mg/dL
- Always correct hypomagnesemia first - hypocalcemia will not resolve until Mg is repleted
Chronic Hypocalcemia
-
Calcitriol (0.25-2 mcg/day) - drug of choice for hypoparathyroidism and CKD (active metabolite, no renal 1α-hydroxylation required)
-
Oral calcium supplementation (10-20 mmol Ca every 6-12 hours)
-
Vitamin D3/D2 (10,000-50,000 IU/day) - for pure vitamin D deficiency (less expensive, longer duration)
-
Alfacalcidol - requires hepatic but not renal hydroxylation
-
Recombinant PTH - for hypoparathyroidism refractory to calcitriol + Ca
-
Thiazide diuretics can help reduce urinary Ca loss in hypoparathyroidism
-
Monitor serum and urine Ca every 1-2 weeks initially; every 3-6 months once stable
-
Goldman-Cecil Medicine, p. 2646; Brenner & Rector's The Kidney, Table 73.12
Key Pitfalls
- Missing hypomagnesemia - the most commonly overlooked reversible cause; always check Mg and replete before treating hypocalcemia
- Treating pseudohypocalcemia - always correct for albumin or measure ionized Ca; don't treat low total Ca in hypoalbuminemia if ionized Ca is normal
- Missing PHP - PTH is markedly elevated (not low) despite hypocalcemia; clinically confused with hypoparathyroidism but requires different interpretation
- Post-thyroidectomy hungry bone syndrome - Ca drops rapidly and requires aggressive IV calcium; phosphate is low (unlike typical hypoparathyroidism)
- Vitamin D deficiency masking PTH response - secondary hyperparathyroidism with low 25-OH-D; 25-OH-D must be measured to confirm
Hypocalcemia workup
The previous response on this exact topic is already in our conversation above. Here is a clean, complete version for reference:
Hypocalcemia Workup
Definition
| Measure | Threshold |
|---|---|
| Total serum calcium | <8.5 mg/dL (<2.12 mmol/L) |
| Ionized (free) calcium | <4.65 mg/dL (<1.16 mmol/L) |
| Mild | Total Ca 8.0-8.5 mg/dL |
| Severe | Total Ca <7.6 mg/dL |
| Neonates | <8 mg/dL |
| Preterm infants | <7 mg/dL |
Step 1 - Confirm True Hypocalcemia (Rule Out Pseudohypocalcemia)
Hypoalbuminemia is the most common artifactual cause. Calcium is ~50% protein-bound (mainly albumin), ~10% anion-complexed, and ~40% ionized (active).
Correction formula:
Corrected Ca = Measured Ca + 0.8 × (4.0 - serum albumin in g/dL)
Every 1 g/dL fall in albumin lowers measured total Ca by ~0.8 mg/dL, but ionized Ca is unaffected. When albumin is low, always measure ionized calcium directly to confirm true hypocalcemia.
Other points:
- Alkalosis shifts Ca to the bound form → lowers ionized Ca without affecting total Ca (important in hyperventilating patients)
- False low readings: specimen freezing/thawing, hemodialysis plasma samples
Step 2 - First-Line Labs
| Test | Purpose |
|---|---|
| Intact PTH | Central branch point of entire workup |
| Serum phosphate (PO4) | Distinguishes causes once PTH known |
| Serum magnesium (Mg) | Hypomagnesemia blocks PTH secretion AND action |
| Creatinine / eGFR | CKD is the most common overall cause |
| Serum albumin | Confirm/exclude pseudohypocalcemia |
| Spot urine Ca:Cr ratio | Distinguish hypocalciuria from hypercalciuria |
| ECG | QT prolongation, arrhythmia risk |
Step 3 - Second-Line Labs (Directed by First Results)
| Test | When to Order |
|---|---|
| 25-OH-D | High PTH + low PO4 → suspect vitamin D deficiency |
| 1,25-(OH)₂D | CKD confirmed (will be low); or VDR/1α-OHase defect suspected |
| Amylase / lipase | Acute pancreatitis suspected |
| CK | Rhabdomyolysis suspected |
| 24-hr urine calcium | Quantify degree of hypocalciuria or hypercalciuria |
| PTHrP | Malignancy with osteoblastic metastases |
| SPEP / UPEP | Paraproteinemia |
| Genetic testing | Suspected CaSR mutation, DiGeorge, PHP subtype |
Diagnostic Algorithms
Goldman-Cecil Medicine - Adult Workup:
Brenner & Rector's The Kidney - Albumin → Urine Ca → PTH → PO4:
Step 4 - Interpret the PTH + Phosphate Pattern
Low/Absent PTH + High PO4 = Hypoparathyroidism
The parathyroid glands are failing - not compensating appropriately.
| Cause | Notes |
|---|---|
| Post-surgical (most common acquired) | After thyroidectomy (1-2%), parathyroidectomy, radical neck dissection |
| Autoimmune | Isolated or APS-1 (hypoparathyroid + Addison's + mucocutaneous candidiasis) |
| DiGeorge syndrome (22q11 deletion) | Absent parathyroids + thymic aplasia + cardiac defects |
| Familial/hereditary | PTH gene mutations, Kenny-Caffey, Sanjad-Sakati syndromes |
| Activating CaSR mutation | Receptor hypersensitive to Ca; suppresses PTH at normal/low Ca → autosomal dominant hypocalcemia with hypercalciuria |
| Infiltrative | Hemochromatosis (iron), Wilson's (copper), granulomas, metastases |
| Toxic | High-dose radiation, asparaginase |
| Hypomagnesemia | Reversible - profound hypoMg impairs both PTH secretion and end-organ response; must correct Mg first |
| Neonatal | Maternal hypercalcemia (suppresses fetal PTH), prematurity, maternal DM, asphyxia, citrated transfusions |
High PTH + Low PO4 = Secondary Hyperparathyroidism (Vitamin D-Related)
PTH is compensating appropriately but Ca remains low - inadequate vitamin D-mediated intestinal Ca absorption.
| Cause | Key Lab Finding |
|---|---|
| Vitamin D deficiency | 25-OH-D ↓↓ |
| Malabsorption (celiac, Crohn's, bariatric, pancreatic insufficiency) | 25-OH-D ↓, may have other fat-soluble vitamin deficiencies |
| Liver disease (impaired 25-hydroxylation) | 25-OH-D ↓ |
| 1α-hydroxylase deficiency (Vit D-dependent rickets type 1) | 25-OH-D normal; 1,25-(OH)₂D ↓↓ |
| VDR mutation (Vit D-dependent rickets type 2) | 25-OH-D normal; 1,25-(OH)₂D ↑↑↑ (compensatory) |
| Anticonvulsants (phenytoin, phenobarbital) | Accelerate vitamin D catabolism; 25-OH-D ↓ |
| Acute pancreatitis | Calcium saponification in retroperitoneum |
| Hungry bone syndrome post-parathyroidectomy | Bone avidly takes up Ca/P; PO4 also low |
| Malnutrition / malabsorption | Combined Ca and vitamin D deficiency |
High PTH + High PO4 = CKD or Pseudohypoparathyroidism
| Cause | Key Distinguishing Feature |
|---|---|
| Chronic kidney disease (most common overall cause) | Cr ↑↑, 1,25-(OH)₂D ↓↓ (lost 1α-hydroxylase); phosphate retention |
| Pseudohypoparathyroidism (PHP) | Cr normal; PTH markedly ↑; infused PTH → subnormal urine cAMP + phosphaturia response; Albright's phenotype (round face, short stature, brachydactyly, subcutaneous ossifications) |
| Massive tumor lysis syndrome | Context: post-chemotherapy; massive phosphate release |
| Rhabdomyolysis (early) | CK ↑↑↑; phosphate released from muscle |
High PTH + High Urinary Calcium
| Cause | Mechanism |
|---|---|
| Activating CaSR mutation (ADHH) | CaSR inappropriately active → low PTH set point + renal Ca wasting |
| FHHNC (familial hypomagnesemia, hypercalciuria, nephrocalcinosis) | Claudin-16/19 mutations; renal Mg AND Ca wasting |
Lab Pattern Summary
| Cause | PTH | PO4 | Mg | 25-OH-D | 1,25-(OH)₂D | Cr |
|---|---|---|---|---|---|---|
| Surgical hypoparathyroidism | ↓/undetectable | ↑ | N | N | Low | N |
| Hypomagnesemia | ↓ (functional) | N | ↓↓ | N | N | N |
| CKD | ↑ | ↑ | N/↓ | N | ↓↓ | ↑↑ |
| Vitamin D deficiency | ↑ | ↓ | N | ↓↓ | ↓ | N |
| Vit D-dep rickets type 1 | ↑ | ↓ | N | N | ↓↓ | N |
| Vit D-dep rickets type 2 | ↑ | ↓ | N | N | ↑↑↑ | N |
| Pseudohypoparathyroidism | ↑↑ | ↑ | N | N | Low-N | N |
| Acute pancreatitis | ↑ | N/↑ | N | N | N | N/↑ |
| Hypoalbuminemia (pseudo) | N | N | N | N | N | N |
Clinical Features That Guide Workup
Symptoms of neuromuscular irritability (correlate with ionized Ca level and rate of fall):
- Perioral, fingertip, and toe paresthesias (earliest symptom)
- Muscle cramps, carpopedal spasm, tetany
- Chvostek sign: tap facial nerve just anterior to ear → circumoral/facial twitching (present in ~10% of normals - low specificity)
- Trousseau sign: inflate BP cuff 20 mmHg above systolic × 3 min → carpal spasm (more specific)
- Seizures (focal, grand mal, or absence)
- Prolonged QT, ventricular arrhythmias, cardiac failure
- Laryngospasm, bronchospasm
Chronic hypocalcemia features (suggest long-standing hypoparathyroidism):
- Subcapsular cataracts
- Basal ganglia calcifications - extrapyramidal signs (choreoathetosis, dystonia)
- Papilledema / increased intracranial pressure
- Poor dentition, enamel hypoplasia
- Dry skin, coarse hair, alopecia, nail changes
- Candidiasis (points to APS-1)
Key Pitfalls
- Missing hypomagnesemia - most commonly overlooked reversible cause; correct Mg first or Ca will not respond to treatment
- Treating pseudohypocalcemia - always correct for albumin or measure ionized Ca; don't treat total Ca in hypoalbuminemia if ionized Ca is normal
- Confusing PHP with hypoparathyroidism - PTH is markedly elevated in PHP (not low); clinical phenotype (Albright's) and PTH infusion test help confirm
- Hungry bone syndrome post-parathyroidectomy - Ca and PO4 both drop rapidly; requires aggressive IV calcium
- Alkalosis - shifts ionized Ca down without changing total Ca; seen in hyperventilating or vomiting patients
- Anticonvulsant-induced - accelerated 25-OH-D catabolism; check 25-OH-D in all epilepsy patients with hypocalcemia
Treatment Summary
Acute Symptomatic (Tetany, Seizures, QT Prolongation, Laryngospasm)
- IV Calcium gluconate 10%: 10 mL (93 mg elemental Ca) slow IV push over >5 min, repeat as needed
- Follow with continuous infusion: 10 ampules (1 g each) in 1L D5W or NS at 50 mL/hr, titrated - 1.2-1.6 mg/kg elemental Ca over 4-6 hours raises Ca by 2-3 mg/dL
- Correct hypomagnesemia concurrently (IV MgSO4)
- Continuous cardiac monitoring during IV infusion
Chronic Hypocalcemia
-
Calcitriol (0.25-2 mcg/day) - drug of choice for hypoparathyroidism and CKD; active metabolite, no renal hydroxylation required
-
Oral calcium (1-3 g elemental Ca/day divided) - calcium carbonate (with food) or calcium citrate (without food)
-
Cholecalciferol/ergocalciferol - for pure vitamin D deficiency (10,000-50,000 IU/day); cheapest, longest-acting
-
Alfacalcidol - requires hepatic (not renal) hydroxylation; useful in CKD
-
Recombinant PTH (teriparatide/PTH 1-84) - for refractory hypoparathyroidism
-
Thiazide diuretics - reduce urinary Ca loss; adjunct in hypoparathyroidism
-
Monitor serum and urine Ca every 1-2 weeks initially, then every 3-6 months once stable; watch for hypercalciuria → nephrolithiasis
-
Goldman-Cecil Medicine, p. 2645-2646; Brenner & Rector's The Kidney, Table 73.11-73.12; Henry's Clinical Diagnosis, p. 253-254; Rosen's Emergency Medicine, p. 2697-2703; Textbook of Family Medicine 9e
Hypercalcemia workup
Finding Sources
Searching PubMed
"hypercalcemia"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive data. Let me compile the full response.
Hypercalcemia Workup
Definition and Severity
| Category | Total Serum Ca |
|---|---|
| Normal | 9.0-10.5 mg/dL (2.25-2.62 mmol/L) |
| Mild | 10.5-12.0 mg/dL |
| Moderate | 12.0-14.0 mg/dL |
| Severe / life-threatening | >14 mg/dL |
- Rosen's Emergency Medicine, p. 2602; Brenner & Rector's The Kidney
Step 1 - Confirm True Hypercalcemia
As with hypocalcemia, always correct for albumin first:
Corrected Ca = Measured Ca + 0.8 × (4.0 - serum albumin in g/dL)
- In hyperalbuminemia (e.g., dehydration, tourniquet effect), total Ca may appear elevated while ionized Ca is normal
- When in doubt, measure ionized calcium directly - this is the active form and not affected by protein binding
Step 2 - First-Line Labs (Simultaneous)
| Test | Reason |
|---|---|
| Intact PTH | Single most important test - central branch point |
| Serum phosphate | Low in PHPT; high in malignancy with bone mets / vitamin D toxicity |
| Creatinine / eGFR | CKD alters Ca metabolism; renal Ca handling impaired |
| Serum albumin | Confirm true hypercalcemia; rule out dehydration artifact |
| Alkaline phosphatase (ALP) | Elevated in bone involvement (PHPT, metastases) |
| Serum magnesium | Often low in PHPT |
| ECG | Shortened QT interval; bradyarrhythmias; AV block at severe levels |
| 24-hr urine calcium + creatinine | Calculate calcium-to-creatinine clearance ratio (CCR) to distinguish PHPT from FHH |
Step 3 - Second-Line Labs (Directed by PTH Result)
| Test | When to Order |
|---|---|
| PTHrP | PTH suppressed → suspect malignancy (humoral hypercalcemia) |
| 25-OH-D | PTH suppressed + vitamin D supplementation/granulomatous disease suspected |
| 1,25-(OH)₂D | Granulomatous disease (sarcoid, TB) - will be markedly elevated; lymphoma |
| SPEP / UPEP + serum free light chains | Multiple myeloma suspected |
| Serum ACE level | Sarcoidosis suspected |
| TSH / free T4 | Hyperthyroidism causing high-bone-turnover hypercalcemia |
| Morning cortisol / ACTH stimulation test | Adrenal insufficiency (rarely causes hypercalcemia) |
| Bone scan / skeletal survey | Metastatic disease or myeloma |
| CXR + CT chest/abdomen/pelvis | Occult malignancy, sarcoidosis, lymphoma |
| Genetic testing (CaSR, GNA11, AP2S1) | FHH suspected |
| Vitamin A level | Supplement/medication history suggests excess |
Diagnostic Algorithm (Harrison's Principles of Internal Medicine)
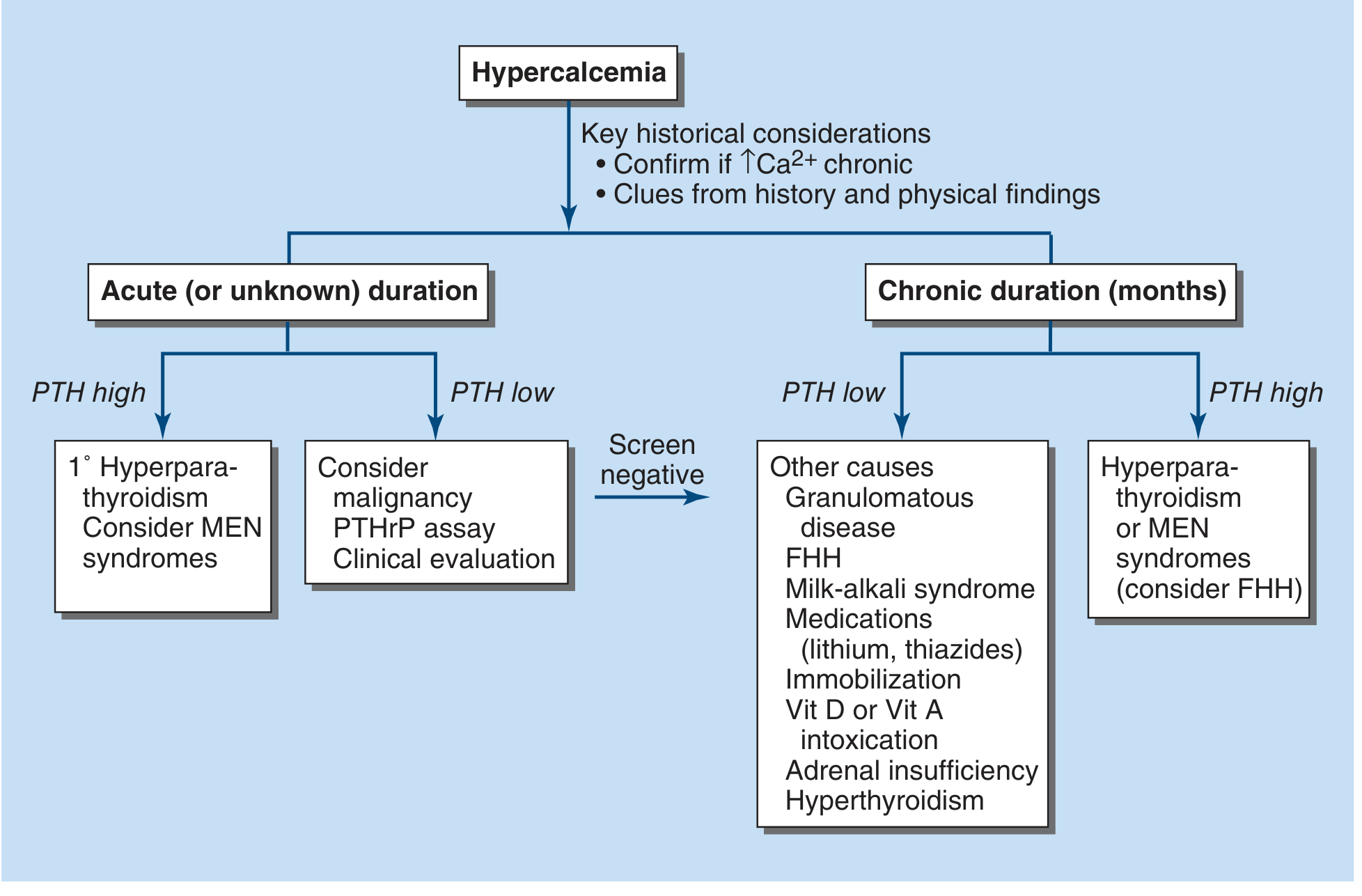
Harrison's Principles of Internal Medicine 22e - Fig. 422-6
Step 4 - Interpret the PTH Result
High/Detectable PTH + Hypercalcemia = PTH-Mediated (Parathyroid Causes)
PTH is inappropriately elevated despite high calcium - the parathyroid glands are not suppressing as expected.
| Cause | Key Features |
|---|---|
| Primary hyperparathyroidism (PHPT) - most common outpatient cause | Solitary adenoma (80%), multigland hyperplasia (15-20%), carcinoma (<1%); PTH elevated; PO4 low-normal; urine Ca elevated; 24-hr urine CCR >0.01 |
| Parathyroid carcinoma | Ca often >14 mg/dL; very high PTH; palpable neck mass; markedly elevated ALP |
| Multiple endocrine neoplasia type 1 (MEN-1) | Parathyroid hyperplasia + pituitary adenoma + pancreatic islet tumors; multigland disease |
| MEN-2A | Parathyroid hyperplasia + medullary thyroid carcinoma + pheochromocytoma |
| Tertiary hyperparathyroidism | Autonomous parathyroid hyperfunction after prolonged secondary HPT (CKD, post-transplant) |
| Lithium therapy | Raises the Ca set point of CaSR; shifts PTH secretion curve upward; urine CCR may be low |
| Familial Hypocalciuric Hypercalcemia (FHH) | Critical to distinguish from PHPT - see below |
Distinguishing PHPT from FHH
FHH (Familial Hypocalciuric Hypercalcemia) is an autosomal dominant condition caused by loss-of-function mutations in CaSR (FHH1), GNA11 (FHH2), or AP2S1 (FHH3) - the parathyroid and kidney sense Ca as lower than it is.
| Feature | PHPT | FHH |
|---|---|---|
| Urine Ca | Elevated | Inappropriately low |
| Ca:Cr Clearance Ratio (CCR) | >0.01 | <0.01 |
| PTH | Elevated | Normal or mildly elevated (80%) |
| Serum Mg | Normal/low | Often mildly elevated (hypermagnesemia) |
| Family history | Usually absent | Present - lifelong asymptomatic hypercalcemia in family |
| Age of onset | Adults | Since birth / childhood |
| Symptoms | Possible | Usually asymptomatic |
| Parathyroidectomy | Curative | Does NOT correct hypercalcemia |
| Treatment | Surgery | Usually none; cinacalcet 30-60 mg/day if symptomatic |
CCR formula:
CCR = (Urine Ca × Serum Cr) / (Serum Ca × Urine Cr)
- <0.01 strongly suggests FHH
- 0.01-0.02 - overlap zone; genetic testing required
Low/Suppressed PTH + Hypercalcemia = Non-PTH-Mediated
The parathyroid glands are appropriately suppressed - the calcium elevation comes from another source.
A. Malignancy (most common cause in hospitalized patients)
Accounts for up to 40% of hypercalcemia in advanced cancer. PTH is suppressed.
| Mechanism | Cancers | Labs |
|---|---|---|
| Humoral hypercalcemia of malignancy (HHM) - PTHrP secretion | Squamous cell (lung, esophagus, cervix, head/neck), kidney, bladder, ovary, breast | PTHrP ↑, PTH ↓, PO4 low-normal, 1,25-OH-D ↓ |
| Osteolytic bone metastases - local cytokines recruit osteoclasts | Breast cancer, lymphoma, multiple myeloma | PTHrP often normal, PTH ↓, PO4 ↑ (bone release), ALP ↑ |
| Ectopic 1,25-(OH)₂D production | Lymphoma (Hodgkin's and NHL) | PTH ↓, 1,25-(OH)₂D ↑, similar to granulomatous disease |
| Ectopic PTH secretion | Rare - ovarian, lung, thymoma | PTH elevated (by intact PTH assay) |
Malignancy Ca levels are typically >14 mg/dL - higher than typical PHPT (<13 mg/dL). Exception: multiple myeloma may present with chronic low-grade hypercalcemia.
B. Granulomatous Disease
Mechanism: Activated macrophages within granulomas express 1α-hydroxylase, converting 25-OH-D → 1,25-(OH)₂D independent of PTH or renal regulation.
| Disease | Key Tests |
|---|---|
| Sarcoidosis (most common) | 1,25-(OH)₂D ↑↑, PTH ↓, serum ACE elevated, CXR (hilar adenopathy), BAL |
| Tuberculosis | 1,25-(OH)₂D ↑↑, PTH ↓; chest imaging; sputum AFB |
| Histoplasmosis, Coccidioidomycosis, Berylliosis | 1,25-(OH)₂D ↑↑, PTH ↓; fungal serology/cultures |
| Crohn's disease, Wegener's, leprosy | 1,25-(OH)₂D ↑↑ |
C. Vitamin D Toxicity
- Requires chronic ingestion >10,000 IU/day (often from supplements or fat-soluble preparations)
- 25-OH-D markedly elevated (>100 ng/mL) - diagnostic
- 1,25-(OH)₂D may not be elevated (25-OH-D itself has direct biologic activity)
- PTH suppressed; urine Ca elevated; phosphate normal or elevated
- 25-OH-D stores persist for weeks after stopping supplementation
D. Vitamin A Toxicity
- Direct bone resorption effect
- History of excess retinoid use (supplements, acne medications in high doses)
- Measure serum vitamin A / retinol
E. High Bone Turnover States
| Cause | Mechanism | Key Feature |
|---|---|---|
| Hyperthyroidism | Thyroid hormones accelerate bone turnover → net Ca release | TSH ↓, free T4 ↑ |
| Immobilization | Loss of mechanical loading → uncoupled osteoclast activity exceeds formation | Context: Paget's disease, spinal cord injury, prolonged bed rest |
| Paget's disease | Focal high turnover; Ca elevated during immobilization | ALP markedly ↑; bone scan |
| Adrenal insufficiency | Reduced renal Ca excretion; increased intestinal Ca absorption | Morning cortisol low; ACTH ↑ |
| Pheochromocytoma | Catecholamines increase PTH secretion AND/OR coexistent MEN-2A | 24-hr urine metanephrines ↑ |
F. Drug-Induced
| Drug | Mechanism |
|---|---|
| Thiazide diuretics | Reduce renal Ca excretion; mild hypercalcemia; common in dehydration |
| Lithium | Raises CaSR set point; shifts PTH secretion threshold upward |
| Calcium carbonate (antacids) + alkali = Milk-alkali syndrome | Ca load + alkalosis → impaired renal Ca excretion; triad of hypercalcemia + metabolic alkalosis + renal failure |
| Vitamin D analogues (topical or systemic) | |
| Estrogens / antiestrogens (tamoxifen) | In patients with breast cancer bone mets - "flare" hypercalcemia |
| All-trans retinoic acid (ATRA) | |
| Aminophylline / theophylline |
Lab Pattern Summary
| Cause | PTH | PTHrP | PO4 | 1,25-(OH)₂D | 25-OH-D | Urine Ca | CCR |
|---|---|---|---|---|---|---|---|
| PHPT | ↑ | N | ↓ | N or ↑ | N | ↑ | >0.01 |
| FHH | N or mildly ↑ | N | N | N | N | ↓ | <0.01 |
| HHM (PTHrP) | ↓ | ↑ | ↓ | ↓ | N | ↑ | - |
| Osteolytic mets | ↓ | N | ↑ | N | N | ↑ | - |
| Lymphoma (1,25-D) | ↓ | N | N | ↑↑ | N | ↑ | - |
| Sarcoidosis | ↓ | N | N | ↑↑ | N | ↑ | - |
| Vitamin D toxicity | ↓ | N | N/↑ | N/↑ | ↑↑ | ↑ | - |
| Hyperthyroidism | ↓ | N | N | N | N | ↑ | - |
| Milk-alkali | ↓ | N | N | N | N | Variable | - |
| Tertiary HPT (CKD) | ↑↑ | N | ↑ | ↓ | N | Variable | - |
Clinical Features
Classic mnemonic: "Bones, Stones, Moans, and Abdominal Groans"
| System | Symptoms |
|---|---|
| Bones | Bone pain, pathologic fractures, subperiosteal resorption (PHPT), osteoporosis |
| Stones | Nephrolithiasis (calcium oxalate/phosphate), nephrocalcinosis, polyuria, polydipsia |
| Moans | Fatigue, weakness, depression, anxiety, confusion, lethargy, coma |
| Abdominal Groans | Nausea, vomiting, constipation, anorexia, acute pancreatitis, peptic ulcer disease |
| Cardiac | Shortened QT interval, bradyarrhythmias, sinus arrest, AV block, AF, VT at >14 mg/dL |
| Renal | Nephrogenic DI (Ca inhibits AVP action in collecting tubule), dehydration, renal failure |
| Chronic | Ectopic calcification (blood vessels, cornea - band keratopathy, soft tissue), chondrocalcinosis |
Severity of symptoms depends on the degree of hypercalcemia AND the rate of onset. Chronic mild hypercalcemia (e.g., PHPT, FHH) is often asymptomatic and discovered incidentally on routine labs.
Biochemical Profile: Primary Hyperparathyroidism (Classic)
| Parameter | PHPT Finding | Reference Range |
|---|---|---|
| Serum calcium | 10.7 mg/dL (mean) | 8.2-10.2 mg/dL |
| Serum phosphorus | 2.8 mg/dL (low-normal) | 2.5-4.5 mg/dL |
| Alkaline phosphatase | 114 IU/L (mildly elevated) | <100 IU/L |
| Intact PTH | 119 pg/mL (elevated) | 10-65 pg/mL |
| 25-OH-D | Often low-normal | |
| 1,25-(OH)₂D | Normal to mildly elevated | |
| Urine Ca | Elevated |
- Textbook of Family Medicine 9e, Table 35-23
Indications for Surgery in Asymptomatic PHPT
Parathyroidectomy is recommended for asymptomatic PHPT if ANY of:
- Serum Ca >1 mg/dL above the upper limit of normal
- eGFR <60 mL/min/1.73 m²
- Nephrolithiasis or nephrocalcinosis on imaging
- 24-hr urine Ca >400 mg/day with elevated stone risk
- Bone mineral density T-score ≤-2.5 at any site, or vertebral fracture
- Age <50 years
Treatment Summary
Acute Symptomatic Hypercalcemia (Ca >12-14 mg/dL or symptomatic)
- IV normal saline (0.9% NaCl) 200-300 mL/hr - restore volume, increase renal Ca excretion (first and most important step)
- Furosemide (loop diuretic) - only after full hydration; promotes calciuresis; use in volume-replete patients or those with CHF/renal failure
- IV bisphosphonates - zoledronate 4 mg IV over 15-30 min (effect in 2-4 days, peaks at 4-7 days); pamidronate 60-90 mg IV over 2-4 hrs
- Calcitonin (4-8 units/kg IM/SC q12h) - fastest onset (hours), transient effect (tachyphylaxis in 48-72h); use for acute bridging with bisphosphonates
- Denosumab (120 mg SC) - for bisphosphonate-refractory malignant hypercalcemia
- Glucocorticoids (prednisone 40-60 mg/day) - highly effective for granulomatous disease and vitamin D toxicity; not effective for PHPT or malignancy
- Dialysis - for severe hypercalcemia with renal failure refractory to above
Cause-Specific
-
PHPT: parathyroidectomy (curative); cinacalcet for surgical candidates
-
Malignancy: treat underlying cancer; zoledronate + denosumab for bone mets; saline diuresis
-
Sarcoidosis/granulomas: glucocorticoids (reduce 1,25-(OH)₂D synthesis); avoid sun/vitamin D
-
FHH: no treatment needed (benign); cinacalcet if symptomatic; never parathyroidectomy
-
Drug-induced: discontinue offending drug; monitor Ca
-
Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine, p. 2644-2646; Rosen's Emergency Medicine, p. 2602-2650; Textbook of Family Medicine 9e, Tables 35-22 to 35-25; Henry's Clinical Diagnosis, p. 253-254
Hypercalcemia workup
The full workup is already in the previous response. Here it is presented cleanly:
Hypercalcemia Workup
Definition and Severity
| Category | Total Serum Ca |
|---|---|
| Normal | 9.0-10.5 mg/dL |
| Mild | 10.5-12.0 mg/dL |
| Moderate | 12.0-14.0 mg/dL |
| Severe / life-threatening | >14 mg/dL |
Step 1 - Confirm True Hypercalcemia
Correct for albumin first:
Corrected Ca = Measured Ca + 0.8 × (4.0 - serum albumin in g/dL)
- Dehydration and hemoconcentration can falsely raise total Ca while ionized Ca is normal
- When in doubt, measure ionized calcium directly - this is the physiologically active fraction
Step 2 - First-Line Labs
| Test | Purpose |
|---|---|
| Intact PTH | Single most important test - the central branch point |
| Serum phosphate | Low in PHPT; elevated in osteolytic mets, vitamin D toxicity |
| Creatinine / eGFR | CKD alters Ca metabolism; renal function affects treatment |
| Serum albumin | Confirm true vs. artifactual hypercalcemia |
| Alkaline phosphatase (ALP) | Elevated with bone involvement (PHPT, metastases, Paget's) |
| Serum magnesium | Often low in PHPT; elevated in FHH |
| 24-hr urine calcium + creatinine | Calculate Ca:Cr clearance ratio (CCR) to separate PHPT from FHH |
| ECG | Shortened QT, bradyarrhythmias, AV block at severe levels |
Step 3 - Second-Line Labs (Directed by PTH)
| Test | When to Order |
|---|---|
| PTHrP | PTH suppressed → suspect humoral hypercalcemia of malignancy |
| 25-OH-D | Vitamin D toxicity suspected; elevated (>100 ng/mL) confirms it |
| 1,25-(OH)₂D | Granulomatous disease (sarcoid, TB) or lymphoma - will be markedly elevated |
| Serum ACE | Sarcoidosis suspected |
| SPEP / UPEP + serum free light chains | Multiple myeloma |
| TSH / free T4 | Hyperthyroidism |
| Morning cortisol / ACTH stim test | Adrenal insufficiency |
| Vitamin A level | Supplement/retinoid use history |
| Bone scan / skeletal survey | Metastatic disease, myeloma, Paget's |
| CXR + CT chest/abdomen/pelvis | Occult malignancy, sarcoidosis, lymphoma |
| CaSR / GNA11 / AP2S1 genetic testing | FHH suspected; family history of asymptomatic hypercalcemia |
Diagnostic Algorithm
Harrison's Principles of Internal Medicine 22e, Fig. 422-6
Step 4 - Interpret the PTH Result
PTH Elevated (Inappropriately High) = Parathyroid-Mediated
| Cause | Key Distinguishing Features |
|---|---|
| Primary hyperparathyroidism (PHPT) | Most common outpatient cause; solitary adenoma 80%, hyperplasia 15-20%, carcinoma <1%; CCR >0.01; urine Ca elevated; PO4 low-normal |
| Parathyroid carcinoma | Ca often >14 mg/dL; very high PTH; palpable neck mass; markedly elevated ALP |
| MEN-1 | Multigland parathyroid hyperplasia + pituitary adenoma + pancreatic islet tumor |
| MEN-2A | Parathyroid hyperplasia + medullary thyroid carcinoma + pheochromocytoma |
| Tertiary hyperparathyroidism | Autonomous parathyroid function after prolonged CKD; post-transplant |
| Lithium therapy | Raises CaSR set point; elevates PTH secretion threshold; can mimic FHH |
| FHH | See table below - must actively exclude before operating |
PHPT vs. FHH - Critical Distinction
FHH (Familial Hypocalciuric Hypercalcemia) is caused by loss-of-function mutations in CaSR (type 1), GNA11 (type 2), or AP2S1 (type 3) - the parathyroid glands and kidneys perceive Ca as lower than it actually is.
Ca:Cr Clearance Ratio (CCR):
CCR = (Urine Ca × Serum Cr) / (Serum Ca × Urine Cr)
| Feature | PHPT | FHH |
|---|---|---|
| CCR | >0.01 | <0.01 |
| Urine calcium | Elevated | Inappropriately low |
| PTH | Elevated | Normal or mildly elevated (80%); elevated in 20% |
| Serum Mg | Normal or low | Often mildly elevated |
| Family history | Usually absent | Present - lifelong asymptomatic hypercalcemia |
| Age of onset | Adults | From birth/childhood |
| Symptoms | Possible | Usually none |
| Parathyroidectomy | Curative | Does NOT correct - must not operate |
| Treatment if needed | Surgery | Cinacalcet 30-60 mg/day |
Note: 20% of FHH patients have CCR >0.01, overlapping with PHPT - genetic testing is definitive in ambiguous cases.
PTH Low/Suppressed = Non-PTH-Mediated
1. Malignancy (most common cause in hospitalized patients; up to 40% of advanced cancer)
| Mechanism | Typical Tumors | Key Labs |
|---|---|---|
| Humoral hypercalcemia of malignancy (HHM) - PTHrP secretion | Squamous cell (lung, esophagus, cervix, head/neck), kidney, bladder, ovary, breast | PTHrP ↑, PO4 ↓, 1,25-OH-D ↓ |
| Osteolytic bone metastases - local cytokines | Breast, lymphoma, multiple myeloma | PTHrP normal, PO4 ↑, ALP ↑ |
| Ectopic 1,25-(OH)₂D production | Hodgkin's and non-Hodgkin's lymphoma | 1,25-(OH)₂D ↑↑ |
| Ectopic PTH secretion (rare) | Ovarian, lung, thymoma | PTH elevated on intact PTH assay |
Malignancy Ca typically >14 mg/dL (higher than PHPT). Multiple myeloma may present with chronic low-grade hypercalcemia, anemia, and elevated globulins.
2. Granulomatous Disease
Activated macrophages express 1α-hydroxylase and produce 1,25-(OH)₂D independent of PTH or renal regulation.
| Disease | Additional Tests |
|---|---|
| Sarcoidosis (most common; 10% have hypercalcemia) | 1,25-(OH)₂D ↑↑, ACE elevated, CXR (bilateral hilar adenopathy) |
| Tuberculosis | AFB cultures, 1,25-(OH)₂D ↑↑ |
| Histoplasmosis, Coccidioidomycosis | Fungal serology, 1,25-(OH)₂D ↑↑ |
| Berylliosis, Wegener's, Crohn's, leprosy | 1,25-(OH)₂D ↑↑ |
3. Vitamin D Toxicity
- Chronic ingestion >10,000 IU/day required (supplements, fortified foods, topical analogues)
- Diagnostic: 25-OH-D >100 ng/mL (25-OH-D itself has direct biological activity at high levels)
- 1,25-(OH)₂D may or may not be elevated
- Stores persist for weeks after stopping supplementation - glucocorticoids may be needed
4. High Bone Turnover States
| Cause | Mechanism | Key Test |
|---|---|---|
| Hyperthyroidism | Accelerated bone resorption > formation | TSH ↓, free T4 ↑ |
| Immobilization (esp. with Paget's, spinal cord injury) | Osteoclast activity uncoupled from formation | Clinical context; ALP ↑ in Paget's |
| Adrenal insufficiency | Reduced renal Ca excretion + increased intestinal absorption | Morning cortisol ↓, ACTH ↑ |
| Pheochromocytoma | Catecholamines stimulate PTH; MEN-2A co-occurrence | 24-hr urine metanephrines ↑ |
| Vitamin A toxicity | Direct bone resorption | Serum retinol ↑; supplement history |
5. Drug-Induced
| Drug | Mechanism |
|---|---|
| Thiazide diuretics | Reduce renal Ca excretion; mild hypercalcemia, especially with dehydration |
| Lithium | Raises CaSR set point; shift in PTH secretion threshold (mimics FHH) |
| Milk-alkali syndrome (calcium carbonate + alkali) | Ca load + metabolic alkalosis → impaired renal excretion; triad: hypercalcemia + alkalosis + renal failure |
| Vitamin D analogues (topical or systemic) | |
| Estrogens / tamoxifen | "Flare" reaction in patients with breast cancer bone metastases |
Lab Pattern Summary
| Cause | PTH | PTHrP | PO4 | 1,25-OH-D | 25-OH-D | Urine Ca | CCR |
|---|---|---|---|---|---|---|---|
| PHPT | ↑ | N | ↓ | N/↑ | N | ↑ | >0.01 |
| FHH | N/↑ | N | N | N | N | ↓ | <0.01 |
| HHM (PTHrP) | ↓ | ↑ | ↓ | ↓ | N | ↑ | - |
| Osteolytic mets | ↓ | N | ↑ | N | N | ↑ | - |
| Lymphoma | ↓ | N | N | ↑↑ | N | ↑ | - |
| Sarcoidosis/granuloma | ↓ | N | N | ↑↑ | N | ↑ | - |
| Vitamin D toxicity | ↓ | N | N/↑ | N/↑ | ↑↑ | ↑ | - |
| Hyperthyroidism | ↓ | N | N | N | N | ↑ | - |
| Tertiary HPT (CKD) | ↑↑ | N | ↑ | ↓ | N | Variable | - |
| Milk-alkali | ↓ | N | N | N | N | Variable | - |
Clinical Features
Classic mnemonic: "Bones, Stones, Moans, and Abdominal Groans"
| System | Manifestations |
|---|---|
| Bones | Bone pain, subperiosteal resorption, pathologic fractures, osteoporosis, osteitis fibrosa cystica (severe PHPT) |
| Stones | Nephrolithiasis (Ca oxalate/phosphate), nephrocalcinosis, polyuria, polydipsia (nephrogenic DI - Ca inhibits AVP action) |
| Moans | Fatigue, muscle weakness (proximal), depression, anxiety, confusion, lethargy, stupor, coma |
| Abdominal Groans | Nausea, vomiting, constipation, anorexia, acute pancreatitis, peptic ulcer disease |
| Cardiac | Shortened QT interval, bradyarrhythmias, sinus arrest, AV block, atrial fibrillation, VT at Ca >14 mg/dL |
| Chronic changes | Band keratopathy (corneal Ca deposits), ectopic vascular calcification, chondrocalcinosis, calciphylaxis |
Symptoms depend on degree + rate of rise. Chronic mild hypercalcemia (PHPT, FHH) is often completely asymptomatic - found incidentally on routine labs.
Indications for Surgery in Asymptomatic PHPT
Parathyroidectomy is recommended if ANY of the following:
- Serum Ca >1 mg/dL above upper limit of normal
- eGFR <60 mL/min/1.73 m²
- Nephrolithiasis or nephrocalcinosis on imaging
- 24-hr urine Ca >400 mg/day with elevated stone risk profile
- BMD T-score ≤-2.5 at any site, or vertebral fracture
- Age <50 years
Acute Treatment of Severe Hypercalcemia (>12-14 mg/dL or symptomatic)
| Step | Intervention | Onset |
|---|---|---|
| 1 | IV 0.9% NaCl 200-300 mL/hr - volume resuscitation + renal Ca excretion | Hours |
| 2 | Calcitonin 4-8 units/kg IM/SC q12h - bridging agent; tachyphylaxis in 48-72h | 2-4 hours |
| 3 | IV zoledronate 4 mg over 15-30 min OR pamidronate 60-90 mg over 2-4h | 2-4 days (peak 4-7 days) |
| 4 | Furosemide - only after full volume repletion; promotes calciuresis | Hours |
| 5 | Denosumab 120 mg SC - for bisphosphonate-refractory malignant hypercalcemia | Days |
| 6 | Glucocorticoids (prednisone 40-60 mg/day) - granulomatous disease and vit D toxicity only | Days |
| 7 | Dialysis - refractory cases with renal failure | Immediate |
- Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine, p. 2644-2646; Rosen's Emergency Medicine, p. 2602-2650; Textbook of Family Medicine 9e, Tables 35-22 to 35-25
This is a shared conversation. Sign in to Orris to start your own chat.