Ecg leads importance
Reading File
Finding Sources
Finding Sources
Searching Images
ECG leads placement and territory
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of ECG leads and their importance, sourced from Harrison's Principles of Internal Medicine (2025) and Miller's Anesthesia.
ECG Leads — Overview and Importance
What Are ECG Leads?
An ECG lead is a configuration that displays the instantaneous difference in electrical potential between specific sets of electrodes. Each lead is analogous to a different "camera angle" looking at the same cardiac electrical events — atrial and ventricular depolarization and repolarization — from different spatial orientations. — Harrison's Principles of Internal Medicine 22E, p. 247
The ECG's utility derives from it being:
- Immediately available
- Noninvasive and inexpensive
- Highly versatile (detects arrhythmias, conduction disturbances, ischemia/infarction, metabolic disturbances, drug toxicities, and susceptibility to sudden cardiac arrest)
The 12 Standard Leads
The 12 conventional ECG leads are divided into two groups:
| Group | Leads | Plane Recorded |
|---|---|---|
| Limb (extremity) leads | I, II, III, aVR, aVL, aVF | Frontal plane |
| Chest (precordial) leads | V1 – V6 | Horizontal plane |
Together, these provide a 3-dimensional representation of cardiac electrical activity.
Frontal Plane Leads (Limb Leads)
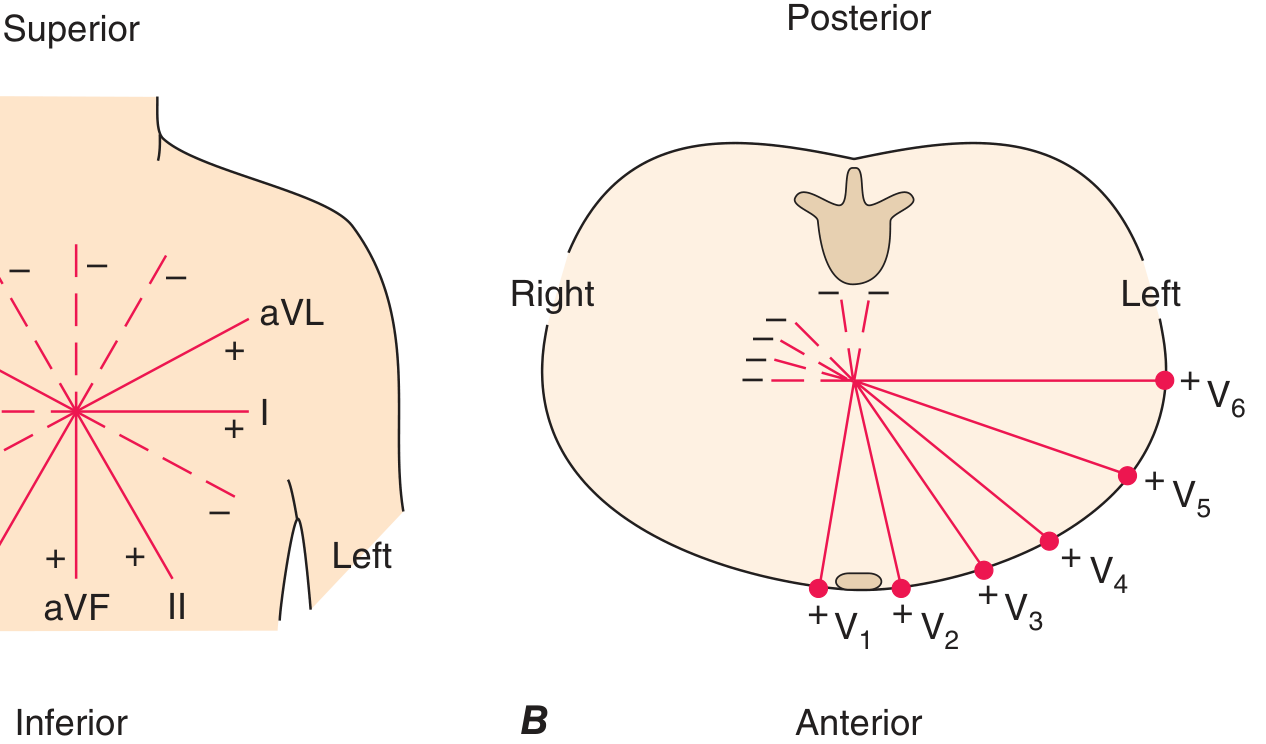
The six frontal leads are organized on a hexaxial diagram (shown below), each with a specific spatial orientation and polarity:
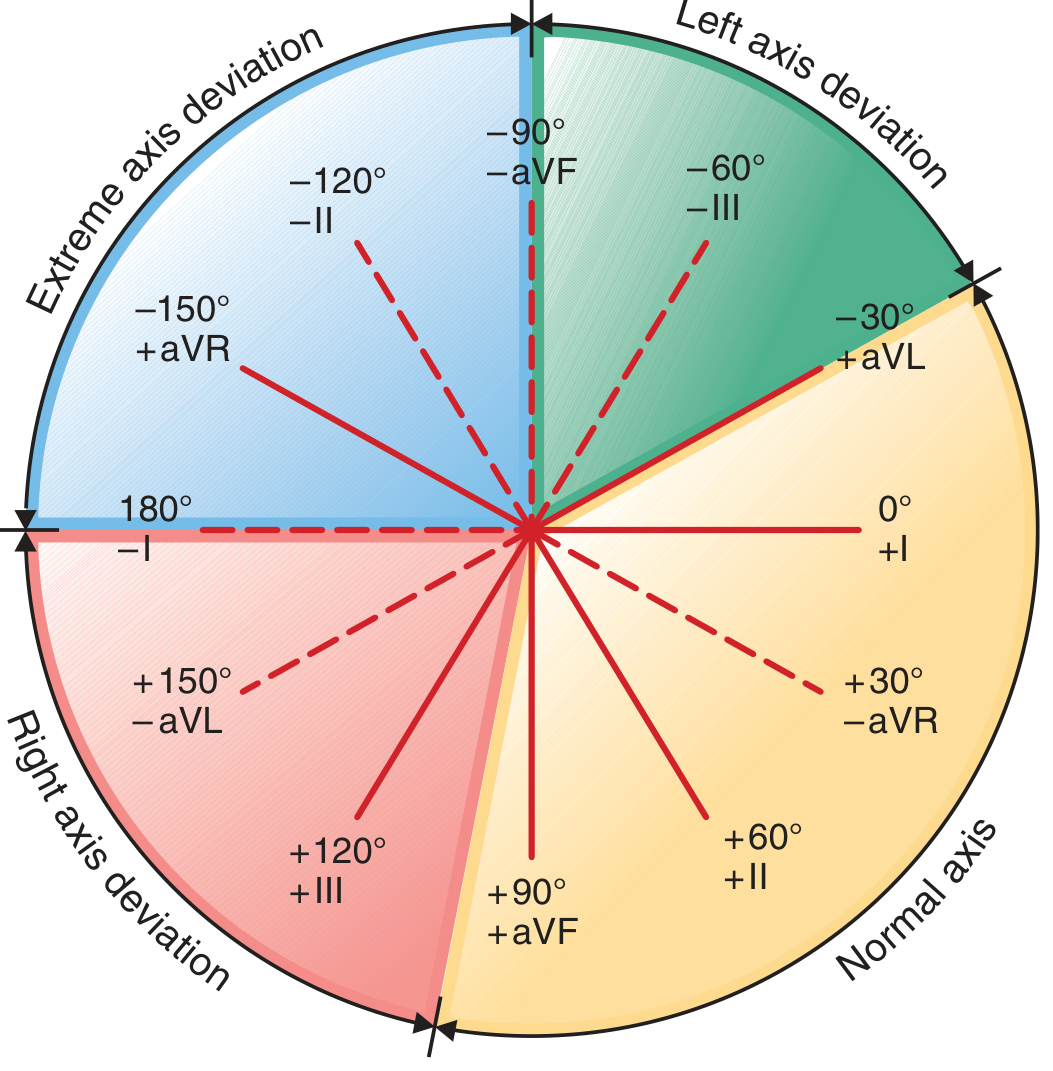
| Lead | Angle | Clinical Importance |
|---|---|---|
| Lead I | 0° | Left lateral view; detects lateral ischemia |
| Lead II | +60° | Best for rhythm monitoring; inferior wall view |
| Lead III | +120° | Inferior wall |
| aVR | −150° | Right upper view; often used in left main/proximal LAD ischemia detection |
| aVL | −30° | High lateral wall |
| aVF | +90° | Inferior wall |
Einthoven's Triangle (Leads I, II, III) forms the basis of the bipolar limb lead system. The augmented leads (aVR, aVL, aVF) are unipolar.
A positive deflection is recorded if the depolarization wave spreads toward the positive pole of a lead; a negative deflection if it spreads away. — Harrison's 22E
Horizontal Plane Leads (Precordial Leads)
| Lead | Position | Clinical Importance |
|---|---|---|
| V1 | 4th ICS, right sternal border | Right ventricular activity; bundle branch blocks; P-wave morphology |
| V2 | 4th ICS, left sternal border | Septal activity; anterior ischemia |
| V3 | Between V2 and V4 | Anterior wall; sensitive for postoperative ischemia |
| V4 | 5th ICS, mid-clavicular line | Anterior wall; highly sensitive for ischemia |
| V5 | Anterior axillary line (same level as V4) | Most sensitive single lead for intraoperative ischemia detection |
| V6 | Mid-axillary line (same level as V4–V5) | Lateral wall |
Lead V5 has historically been shown to be the most sensitive single lead for detecting ischemia during exercise stress testing and during anesthesia. — Miller's Anesthesia 10e
For high-risk vascular procedures, leads V3 or V4 may be even more sensitive for prolonged postoperative myocardial ischemia. — Miller's Anesthesia 10e
Localization of Myocardial Infarction by Lead Group
| Territory | Leads Showing Changes | Coronary Artery |
|---|---|---|
| Inferior | II, III, aVF | RCA (or LCx) |
| Anterior | V1–V4 | LAD |
| Lateral | I, aVL, V5, V6 | LCx |
| Septal | V1, V2 | Septal branches of LAD |
| Right ventricle | V3R–V6R (right-sided leads) | RCA |
| Posterior | Reciprocal changes in V1–V2; direct in V7–V9 | LCx or RCA |
Additional / Special Leads
- Right precordial leads (V3R–V6R): Used to detect right ventricular ischemia/infarction
- Posterior leads (V7–V9): Detect posterior MI (often missed on standard 12-lead)
- 15-lead ECG: Adds V4R, V8, V9 for broader coverage
- Holter monitors / wearable patches: Typically use 1–2 modified leads for continuous monitoring
Key Clinical Summary
| Purpose | Most Relevant Leads |
|---|---|
| Rhythm analysis | II (and V1 for P waves) |
| Axis determination | I, II, aVF |
| Intraoperative ischemia monitoring | V5 (± II) |
| Inferior MI | II, III, aVF |
| Anterior MI | V1–V4 |
| Lateral MI | I, aVL, V5, V6 |
| Right ventricular MI | V3R–V6R |
| Drug toxicity / QT monitoring | II or V5 |
The standard 12-lead ECG remains the cornerstone of cardiac diagnosis because its combination of frontal and horizontal plane perspectives allows both precise localization of pathology and comprehensive rhythm assessment simultaneously.
This is a shared conversation. Sign in to Orris to start your own chat.