Epidemiology
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of core epidemiology concepts, drawn from Park's Textbook of Preventive and Social Medicine and Sabiston Textbook of Surgery.
Epidemiology - Core Concepts & Definitions
1. What is Epidemiology?
Epidemiology is the study of the distribution and determinants of health-related states or events in specified populations, and the application of this study to the control of health problems. The epidemiologist studies disease occurrence in people who, during their lives, are exposed to numerous factors - some of which may have a role in disease causation.
2. Measures of Disease Frequency
Incidence
Incidence rate = the number of new cases occurring in a defined population during a specified time period.
$$\text{Incidence Rate} = \frac{\text{Number of new cases of a disease in a given time period}}{\text{Population at risk during that period}} \times 1000$$
Example: 500 new cases in a population of 30,000 in one year:
- Incidence = 500/30,000 × 1000 = 16.7 per 1,000 per year
Key points:
- Refers only to new cases
- Must always include the unit of time (e.g., per year)
- Not influenced by duration of disease
- Best used for studying aetiology and causal hypotheses
- Mainly used for acute conditions
Special incidence rates:
| Rate | Definition |
|---|---|
| Attack rate | Incidence rate expressed as %, used during epidemics for a limited exposure period |
| Secondary attack rate | Number of exposed persons developing disease within the incubation period after exposure to a primary case |
| Hospital admission rate | New hospital admissions per defined population per time |
Prevalence
Prevalence = all current cases (old and new) existing at a given point in time or over a period of time, in a given population. Note: although called a "rate," prevalence is technically a ratio.
(a) Point Prevalence
Cases at one specific point in time.
$$\text{Point Prevalence} = \frac{\text{All current cases at a given point in time}}{\text{Estimated population at the same point}} \times 100$$
(b) Period Prevalence
All cases (old and new) existing during a defined time period (e.g., one calendar year).
$$\text{Period Prevalence} = \frac{\text{Existing cases during a given time interval}}{\text{Estimated mid-interval population at risk}} \times 100$$
The Incidence-Prevalence Diagram
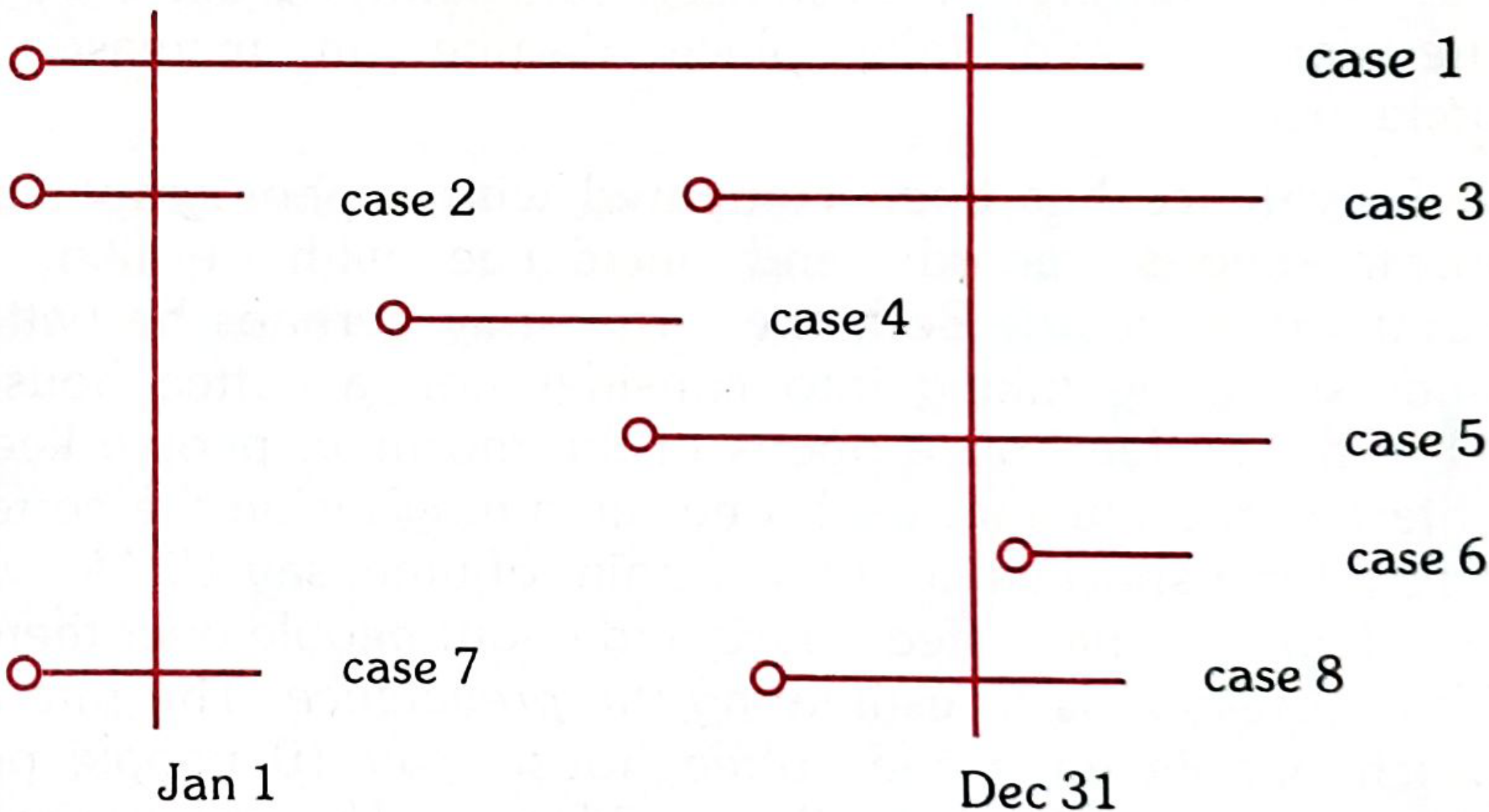
From the diagram above:
- Incidence (new cases Jan-Dec) = Cases 3, 4, 5, 8
- Point prevalence Jan 1 = Cases 1, 2, 7
- Point prevalence Dec 31 = Cases 1, 3, 5, 8
- Period prevalence (Jan-Dec) = Cases 1, 2, 3, 4, 5, 7, 8
The P = I × D Relationship
For a stable population (stable incidence and duration):
P = I × D (Prevalence = Incidence × Mean Duration)
Example: If incidence = 10 per 1,000/year and mean duration = 5 years, then prevalence = 50 per 1,000.
- Tuberculosis has a high prevalence relative to incidence because of its long duration.
- Limitations of prevalence: It is NOT ideal for aetiological studies because it is affected by both causal factors (incidence) and prognostic factors (duration). Use incidence for causal hypotheses.
Uses of prevalence: Estimate magnitude of health problems, identify high-risk groups, plan healthcare resources (beds, manpower, rehabilitation facilities).
3. Bias, Confounding, and Chance
These are the three threats to the internal validity of a study (the degree to which observed outcomes are truly caused by the exposure under study).
Chance
Unpredictable randomness of events that can mislead researchers. Addressed by adequate sample size and statistical testing.
Bias
A systematic error in how subjects were selected or assessed, leading to inaccurate estimates of effect. Two main types:
| Type | Description | Example |
|---|---|---|
| Selection bias | Errors in choosing study subjects - subjects are not typical of the target population, or are more likely to have the outcome for reasons unrelated to the intervention | Paid volunteers may comply more with treatment |
| Measurement (information) bias | Errors in how data on exposures or outcomes are collected | Recall bias in case-control studies |
Confounding
Confounding occurs when a third variable (the confounder) is associated with both the exposure and the outcome, creating a spurious association. Confounding variables distribute risk unevenly between comparison groups.
Methods to control confounding:
- Randomization (gold standard - balances both measured and unmeasured confounders)
- Restriction
- Matching
- Multivariate analysis / statistical adjustment
- Stratification
4. Epidemiological Study Designs
Studies are classified as observational (nature takes its course) or experimental (investigator intervenes).
Observational Studies
| Study Type | Also Called | Unit of Study | Key Feature |
|---|---|---|---|
| Ecological | Correlational | Populations | Looks at group-level data |
| Cross-sectional | Prevalence study | Individuals | Exposure and outcome measured simultaneously |
| Case-control | Case-reference | Individuals | Starts from outcome, looks back at exposure |
| Cohort | Follow-up | Individuals | Starts from exposure, follows forward to outcome |
Experimental Studies (Intervention)
| Study Type | Unit of Study |
|---|---|
| Randomized controlled trial (RCT) | Patients |
| Field trial | Healthy people |
| Community trial | Communities |
Evidence hierarchy (highest to lowest for establishing causation):
- Systematic reviews / meta-analyses
- RCTs
- Cohort studies
- Case-control studies
- Cross-sectional studies
- Case reports / expert opinion
5. Internal vs. External Validity
| Concept | Meaning |
|---|---|
| Internal validity | The observed outcome is truly the result of the specific intervention (not bias, confounding, or chance) |
| External validity (generalizability) | Results can be applied to real-world clinical practice outside the study setting |
| Efficacy | How well an intervention works under ideal, controlled conditions |
| Effectiveness | How well it works when applied generally in an uncontrolled environment |
6. Key Additional Terms
| Term | Definition |
|---|---|
| Morbidity | Any departure from a state of physiological or psychological well-being; measured by incidence and prevalence |
| Mortality rate | Deaths per unit population per time period |
| Case fatality rate (CFR) | Deaths from a disease / total cases of that disease × 100 |
| Proportionate mortality rate | Deaths from a specific cause / total deaths × 100 |
| Population at risk | The denominator group actually susceptible to the disease being measured |
Sources: Park's Textbook of Preventive and Social Medicine; Sabiston Textbook of Surgery (Biological Basis of Modern Surgical Practice); Goldman-Cecil Medicine
Circulatory System From General Anatomy full chapter with diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is the full chapter on the Circulatory System from Color Atlas of Human Anatomy Vol. 2: Internal Organs (THIEME), which is the definitive general anatomy reference for this topic.
Chapter 2: Cardiovascular System
Color Atlas of Human Anatomy, Vol. 2 - Internal Organs (THIEME)
Chapter Contents
| Section | Topic |
|---|---|
| 2.1 | Overview - Circulatory System and Lymphatic Vessels |
| 2.2 | Heart |
| 2.3 | Arterial System - Aorta |
| 2.4 | Arteries of the Head and Neck |
| 2.5 | Arteries of the Shoulder and Upper Limb |
| 2.6 | Arteries of the Pelvis and Lower Limb |
| 2.7 | Venous System |
| 2.8 | Tributaries of the Superior Vena Cava |
| 2.9 | Tributaries of the Inferior Vena Cava |
| 2.10 | Lymphatic System |
| 2.11 | Structure and Function of Blood and Lymphatic Vessels |
2.1 Overview - Circulatory System and Lymphatic Vessels
Circulation of blood occurs in a closed system of tubes (blood vessels) with the heart serving as the central pump. The heart is divided into a right half and a left half, each consisting of an atrium and a ventricle. Vessels carrying blood away from the heart are arteries; vessels carrying blood toward the heart are veins - regardless of oxygen content.
Two Circulations
Human postnatal circulation can be illustrated as a figure-of-eight, with the heart at its intersection acting as both a suction and pressure pump.
Arterial blood pressure = Cardiac output × Peripheral resistance
Pulmonary Circulation (Right Heart)
Deoxygenated blood flows:
- Right atrium → Right ventricle → Pulmonary trunk → Right and left pulmonary arteries → Lung capillaries (gas exchange: O₂ in, CO₂ out) → Pulmonary veins → Left atrium
Systemic Circulation (Left Heart)
Oxygenated blood flows:
- Left atrium → Left ventricle → Aorta → Organ-specific arterial circuits → Arterioles → Capillaries (gas + metabolite exchange) → Venules → Veins → Superior/Inferior vena cava → Right atrium
Portal Circulation (Special Circuit)
Venous blood from the unpaired abdominal organs (stomach, intestines, pancreas, spleen) does NOT flow directly into the vena cava. Nutrients absorbed from the intestine are carried via the portal vein to the liver for processing, before returning to systemic circulation via hepatic veins.
Fetal Circulation
Before birth, several special shunts operate:
- Foramen ovale - opening between right and left atrium (bypasses lungs)
- Ductus arteriosus - connects pulmonary trunk to aortic arch (bypasses lungs)
- Ductus venosus - bypasses hepatic circulation
- Umbilical arteries/veins carry blood to/from the placenta
All shunts close at or soon after birth as pulmonary respiration begins.
2.2 Heart
Position and External Features
The heart lies in the mediastinum within the pericardial cavity. It has four surfaces:
- Sternocostal (anterior) surface - formed mainly by the right ventricle
- Diaphragmatic (inferior) surface - formed mainly by the left ventricle
- Base (posterior) - formed by the left atrium receiving the pulmonary veins
- Apex - formed by the left ventricle, pointing left, downward, and forward
Posterior view of the heart with great vessels:
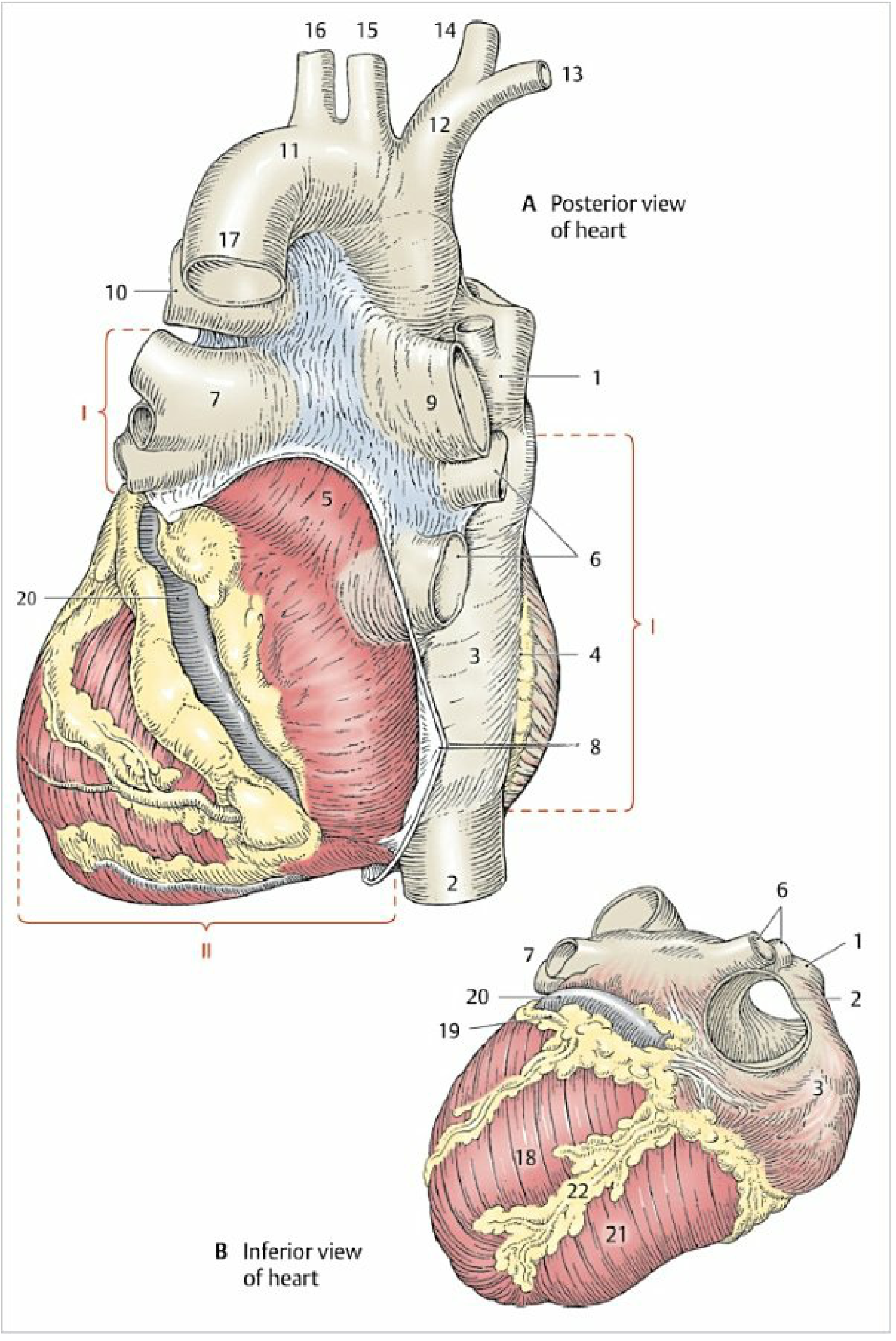
Fig. 2.4 - Posterior (A) and inferior (B) views of the heart. Key structures: (1) Superior vena cava, (2) Inferior vena cava, (3) Right atrium, (6) Right/left pulmonary veins, (11) Aortic arch, (12) Brachiocephalic trunk, (17) Descending aorta, (20) Coronary sinus, (22) Posterior interventricular sulcus.
Heart Chambers
| Chamber | Key Features |
|---|---|
| Right atrium | Receives SVC + IVC; contains fossa ovalis (remnant of foramen ovale); right auricle |
| Right ventricle | Trabeculated; papillary muscles; conus arteriosus leads to pulmonary trunk |
| Left atrium | Smooth walls; receives 4 pulmonary veins; left auricle |
| Left ventricle | Thick muscular wall (~3× right ventricle); 2 papillary muscles; outflow to aorta |
Cardiac Conduction System
The impulse originates in the sinoatrial (SA) node (right atrial wall near SVC opening) and spreads:
SA node → Atrial myocardium → Atrioventricular (AV) node (floor of right atrium) → Bundle of His → Right and left bundle branches → Purkinje fibers → Ventricular myocardium
Heart Valves
Atrioventricular Valves (close during systole)
- Tricuspid valve (right) - 3 cusps: anterior, posterior, septal. Chordae tendineae attach to 3 papillary muscles.
- Bicuspid/Mitral valve (left) - 2 cusps: anterior (anteromedial) and posterior (posterolateral). The anterior cusp is continuous with the aortic wall at its septal origin.
Semilunar Valves (close during diastole)
- Pulmonary valve - 3 semilunar cusps guarding the pulmonary trunk orifice
- Aortic valve - 3 semilunar cusps; behind the anterior and left cusps are the openings of the left and right coronary arteries
Coronary Arteries
| Artery | Origin | Supply |
|---|---|---|
| Right coronary artery (RCA) | Right aortic sinus | Right atrium, right ventricle, SA node (60%), AV node (80%), posterior left ventricle |
| Left coronary artery (LCA) | Left aortic sinus | Divides into: |
| - Left anterior descending (LAD) | LCA | Anterior LV wall, anterior IVS, apex |
| - Circumflex artery | LCA | Lateral and posterior LV wall, left atrium |
Myocardium and Wall Layers
| Layer | Description |
|---|---|
| Epicardium | Visceral layer of serous pericardium; contains coronary vessels and subepicardial fat |
| Myocardium | Cardiac muscle; interconnected by intercalated discs; cannot regenerate after ischemia |
| Endocardium | Inner lining; continuous with vessel endothelium |
Pericardium
The pericardium encloses the heart and roots of the great vessels. It consists of:
- Fibrous pericardium (outer) - collagenous; attached to diaphragm, sternum, and vertebral column; anchors the heart
- Serous pericardium (inner, two layers):
- Parietal layer - lines fibrous pericardium
- Visceral layer (epicardium) - covers heart surface
- Between them: pericardial cavity with ~20-50 mL serous fluid
- Transverse pericardial sinus - passage between aorta/pulmonary trunk (anteriorly) and great veins (posteriorly); surgically important for clamping the aorta
- Oblique pericardial sinus - behind left atrium between pulmonary veins and IVC
2.3 Arterial System - The Aorta
The aorta is the main trunk of the systemic circulation, divided into four parts:
| Segment | Location |
|---|---|
| Ascending aorta (I) | From aortic valve to aortic arch; gives off right and left coronary arteries |
| Aortic arch (II) | Three branches: brachiocephalic trunk, left common carotid artery, left subclavian artery |
| Thoracic aorta (IIIa) | From aortic isthmus to aortic hiatus of diaphragm; gives off posterior intercostal arteries (spaces 3-11), bronchial, esophageal, and pericardial branches |
| Abdominal aorta (IIIb) | From aortic hiatus to L4 (bifurcation) |
Diagram - Aorta with all branches:
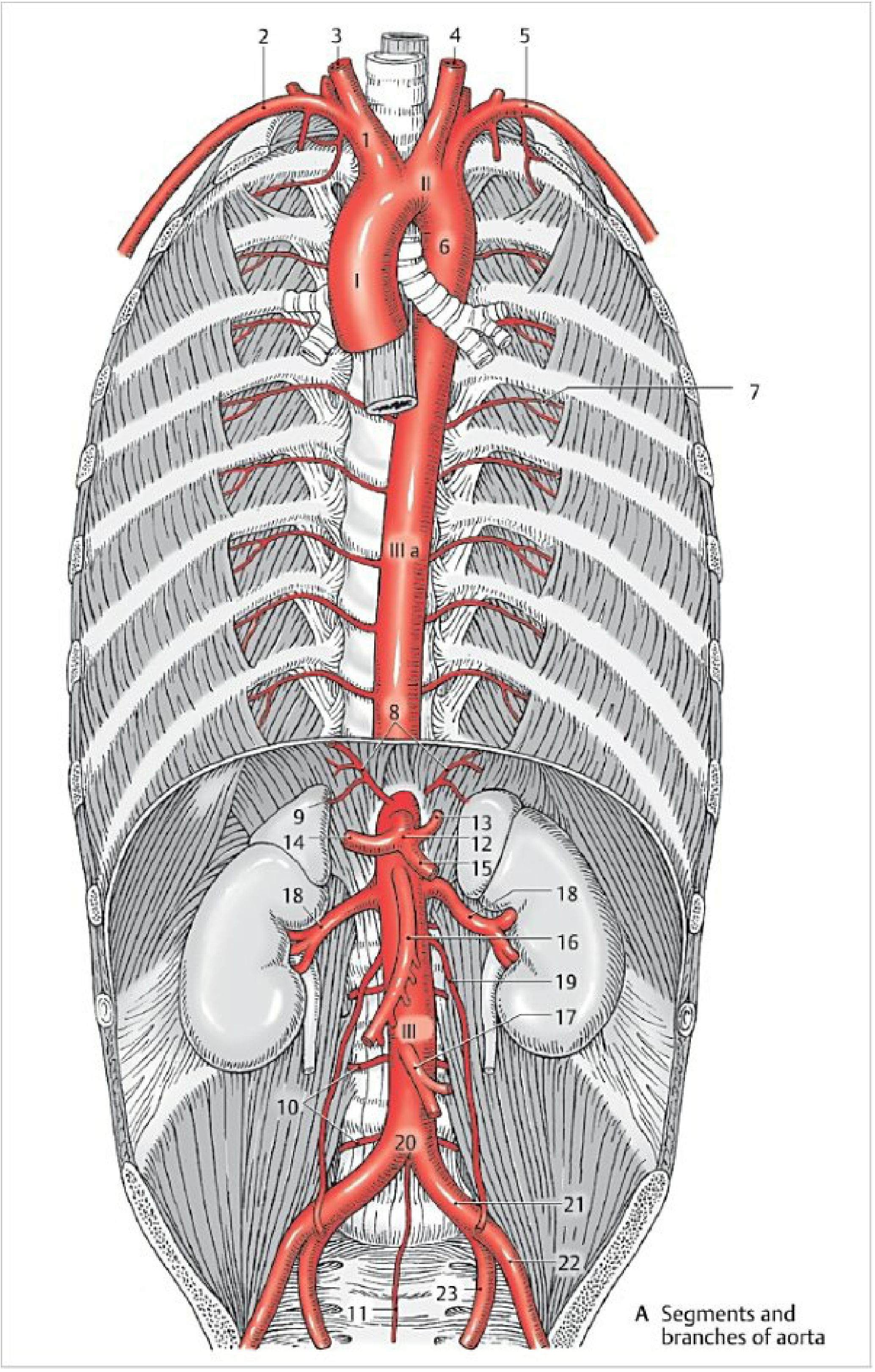
Fig. 2.20 - The aorta and its branches. (I) Ascending aorta, (II) Aortic arch, (IIIa) Thoracic aorta, (IIIb) Abdominal aorta. Key branches: (7) Posterior intercostal arteries, (8) Inferior phrenic artery, (12) Celiac trunk, (13) Left gastric artery, (14) Common hepatic artery, (15) Splenic artery, (16) Superior mesenteric artery, (17) Inferior mesenteric artery, (18) Renal arteries, (20) Aortic bifurcation at L4, (21) Common iliac arteries.
Abdominal Aorta Branches
Parietal branches:
- Inferior phrenic arteries (with superior suprarenal arteries)
- Lumbar arteries ×4 pairs (segmental)
- Median sacral artery (caudal continuation)
Unpaired visceral branches:
- Celiac trunk (T12) → left gastric, common hepatic, splenic arteries
- Superior mesenteric artery (~1 cm below celiac) → small intestine, ascending and transverse colon
- Inferior mesenteric artery (L3-4) → descending colon, sigmoid, rectum
Paired visceral branches:
- Middle suprarenal arteries
- Renal arteries
- Gonadal (ovarian/testicular) arteries
Terminal bifurcation at L4 → Right and left common iliac arteries → split at sacroiliac joint into:
- External iliac artery (becomes femoral artery below inguinal ligament)
- Internal iliac artery (supplies pelvic organs and walls)
Clinical note: The intercostal arteries run along the lower border of the ribs - pleural aspiration/chest drain insertion should always be sited at the upper border of the rib below to avoid neurovascular injury.
2.4 Arteries of the Head and Neck
Common Carotid Artery
Bifurcates at C3-C4 into:
- Internal carotid artery - enters carotid canal; supplies the brain and eye via the circle of Willis
- External carotid artery - supplies the face, scalp, and neck
Circle of Willis (Arterial Circle of the Brain)
Formed by anastomoses at the base of the brain:
- Anterior communicating artery - connects left and right anterior cerebral arteries
- Anterior cerebral arteries (×2)
- Internal carotid arteries (×2)
- Posterior communicating arteries (×2)
- Posterior cerebral arteries (×2, from basilar artery)
The basilar artery is formed by union of the two vertebral arteries and gives off: anterior inferior cerebellar arteries, labyrinthine arteries, superior cerebellar arteries, and terminates as the posterior cerebral arteries.
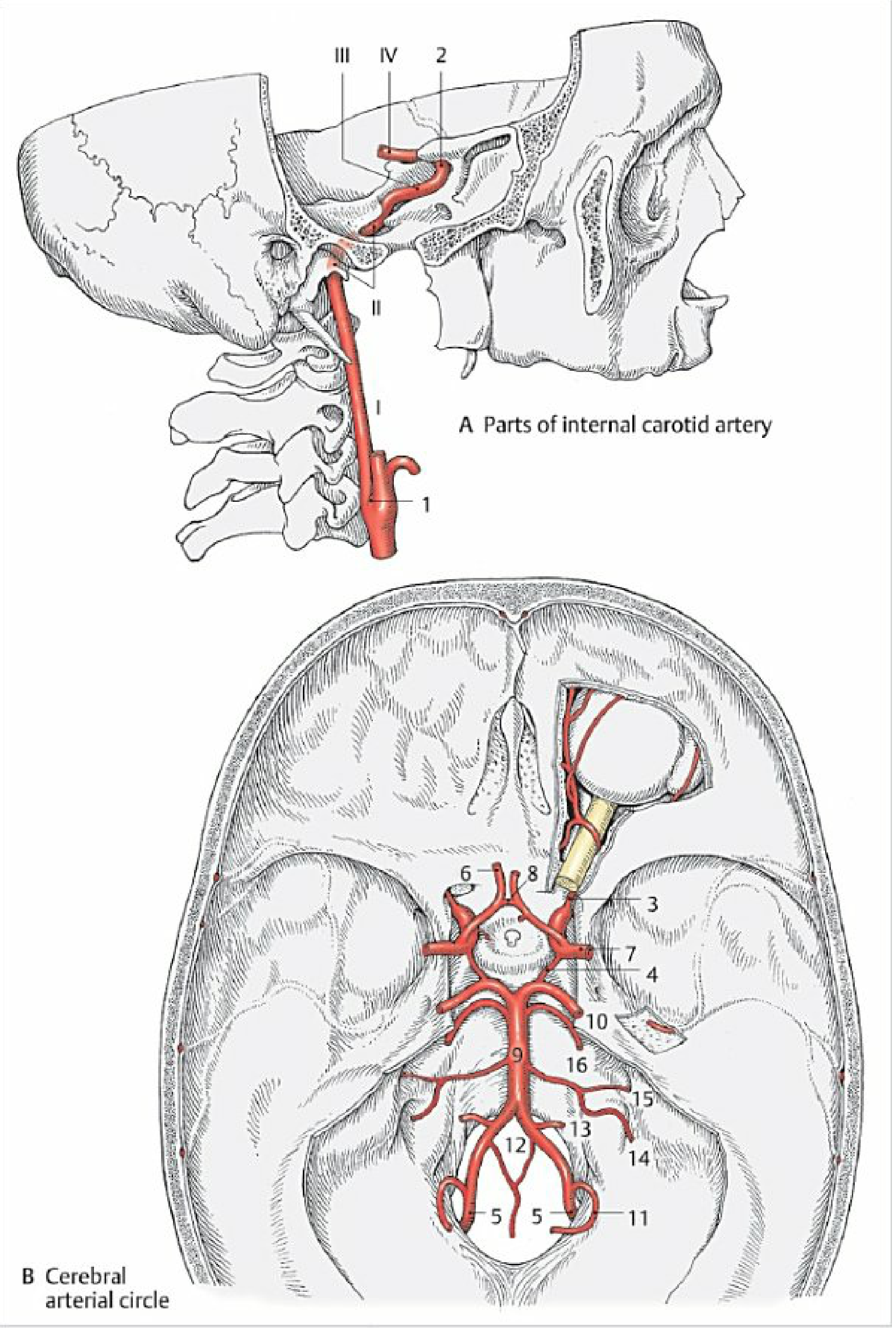
Fig. 2.23 - Arterial circle (Circle of Willis) and branches of the internal carotid and basilar arteries.
Subclavian Artery
Conveys blood to the neck, anterior chest wall, shoulder girdle, and arm. Three parts relative to anterior scalene muscle.
Major branches:
- Vertebral artery - ascends through transverse foramina C6-C1 → foramen magnum → forms basilar artery
- Internal thoracic artery - runs parallel to sternum; gives anterior intercostal branches; terminal branch = superior epigastric artery
- Thyrocervical trunk - branches to thyroid, scapular region
- Costocervical trunk - superior intercostal and deep cervical arteries
2.5 Arteries of the Upper Limb
The subclavian artery continues as:
Subclavian → Axillary (at lateral border of 1st rib) → Brachial (at lower border of teres major) → Radial + Ulnar (at elbow)
Key Branches
| Artery | Branch | Supply |
|---|---|---|
| Axillary | Thoracoacromial, lateral thoracic, subscapular, circumflex humeral | Shoulder region |
| Brachial | Deep brachial (profunda brachii), superior/inferior ulnar collaterals | Arm |
| Radial | Radial recurrent, posterior carpal, deep palmar branch | Lateral forearm, thumb |
| Ulnar | Anterior/posterior ulnar recurrent, common interosseous | Medial forearm |
Vascular Arches of the Hand
- Deep palmar arch - mainly radial artery + deep palmar branch of ulnar → gives palmar metacarpal arteries
- Superficial palmar arch - mainly ulnar artery + superficial palmar branch of radial → gives common palmar digital arteries → proper palmar digital arteries to fingers
- Posterior carpal arch - dorsal supply via posterior metacarpal arteries → posterior digital arteries
2.6 Arteries of the Pelvis and Lower Limb
The external iliac artery becomes the femoral artery below the inguinal ligament and continues as:
Femoral → Popliteal (at adductor canal) → Anterior tibial + Posterior tibial (at tibial head)
Lower Limb Arterial Chain
| Segment | Key Branches |
|---|---|
| Femoral | Superficial/deep femoral (profunda femoris), circumflex femoral arteries |
| Popliteal | Genicular arteries (anastomosis around knee) |
| Anterior tibial | Continues as dorsalis pedis on dorsum of foot |
| Posterior tibial | Fibular (peroneal) artery; terminates as medial and lateral plantar arteries |
Vascular Arches of the Foot
- Deep plantar arch (corresponds to deep palmar arch) → plantar metatarsal arteries → plantar digital arteries
- The superficial plantar arch is usually absent
2.7 Venous System
The venous system consists of three circuits:
- Pulmonary veins (4 veins → left atrium)
- Systemic veins draining to superior and inferior vena cava
- Portal venous system
Veins have thinner walls and larger lumens than arteries. They contain valves (especially in the lower limbs) that prevent backflow. Venous blood is driven by respiratory pump, muscle pump, and residual cardiac pressure.
Superior Vena Cava (SVC) System
Formed by the union of the two brachiocephalic veins behind the sternal angle. Drains head, neck, upper limbs, and thoracic wall.
Key tributaries:
- Internal jugular vein (drains the brain and deep face) + Subclavian vein → Brachiocephalic vein
- External jugular vein - drains superficial face and scalp into subclavian vein
- Azygos system - drains posterior thoracic wall; the azygos vein (right side) arches over root of right lung to drain into SVC
Dural Venous Sinuses (Intracranial Veins)
Blood from the brain drains via dural venous sinuses into the internal jugular vein:
| Sinus | Drainage pathway |
|---|---|
| Superior sagittal sinus | → Confluence of sinuses → Transverse sinuses |
| Inferior sagittal sinus | → Straight sinus → Confluence of sinuses |
| Straight sinus | Receives great cerebral vein (of Galen) |
| Transverse sinuses | → Sigmoid sinuses → Internal jugular veins |
| Cavernous sinuses | Receive ophthalmic veins; → inferior petrosal sinuses → internal jugular |
Emissary veins connect intracranial sinuses to extracranial veins through skull foramina.
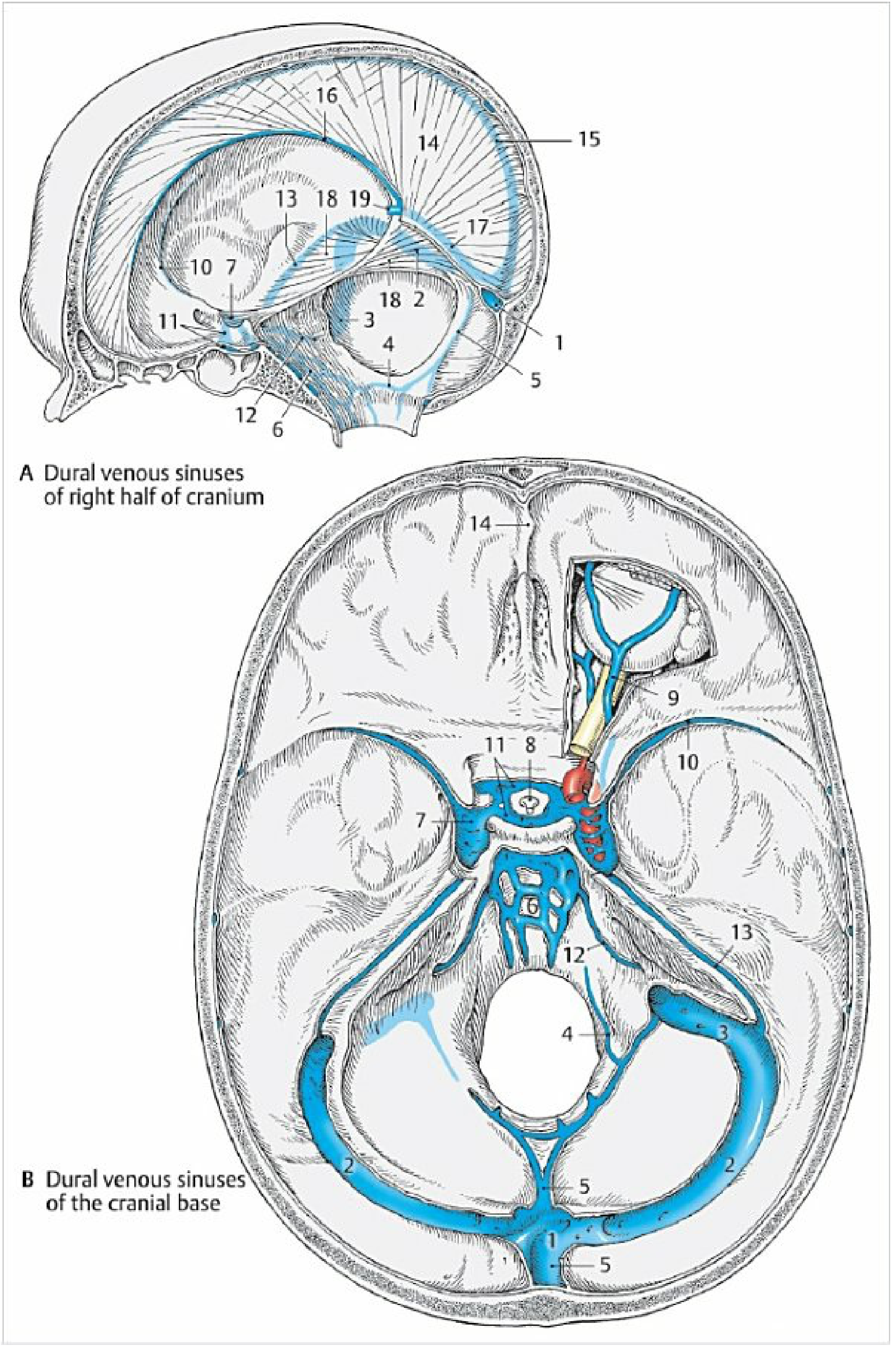
Fig. 2.33 - Dural venous sinuses viewed from the right lateral and basal aspects.
Inferior Vena Cava (IVC) System
The IVC is formed at L4-5 by the union of the two common iliac veins. Drains the lower half of the body.
Direct tributaries:
- Lumbar veins, gonadal veins, renal veins, suprarenal veins, inferior phrenic veins, hepatic veins
Portal vein system (special): Drains stomach, intestines, pancreas, spleen → portal vein → liver sinusoids → hepatic veins → IVC. The portal-systemic anastomoses (at esophagus, rectum, umbilicus) are clinically important in portal hypertension.
Veins of the Upper Limb
- Deep veins accompany arteries (venae comitantes)
- Superficial veins:
- Cephalic vein - lateral forearm/arm → axillary vein
- Basilic vein - medial forearm/arm → brachial vein
- Median cubital vein - connects cephalic and basilic at elbow; site of venipuncture
Veins of the Lower Limb

Fig. 2.36 - Veins of the lower limb, showing the great and small saphenous veins and the deep venous system.
- Great saphenous vein - longest vein in the body; medial surface, from foot to femoral vein at saphenofemoral junction (just below inguinal ligament)
- Small saphenous vein - posterior leg; drains into popliteal vein
- Deep veins - anterior/posterior tibial, popliteal, femoral veins
- Perforating (Cockett's) veins - connect superficial and deep systems; contain valves directing flow from superficial to deep
- Incompetent perforating veins → varicose veins
2.10 Lymphatic System
Lymphatic Vessels
The lymphatic system begins with lymphatic capillaries - blind-ended, valveless vessels in the interstitium. Lymph arises from filtration of blood from arterial capillaries into interstitial spaces. The pathway:
Lymphatic capillaries → Lymphatic vessels (with valves) → Lymph nodes → Lymphatic trunks → Venous angles
Lymphatic vessels are divided into superficial (above fascia) and deep (below fascia) vessels.
Main Lymphatic Trunks
| Trunk | Drains |
|---|---|
| Thoracic duct (left) | Entire lower body + left upper body → left venous angle (left subclavian-jugular junction) |
| Right lymphatic duct | Right head/neck, right arm, right thorax → right venous angle |
Thoracic duct - the main trunk of the entire lymphatic system:
- Begins at cisterna chyli (spindle-shaped dilatation at L1, right of aorta)
- Receives: right and left lumbar trunks, intestinal trunks, left bronchomediastinal trunk, left subclavian trunk, left jugular trunk
- Opens into left venous angle
Regional Lymph Nodes
Head and neck:
- Occipital, mastoid, parotid, submandibular, submental, anterior/posterior cervical, supraclavicular nodes
Thorax:
- Parasternal, intercostal, tracheobronchial, mediastinal nodes
Abdomen:
- Celiac, superior/inferior mesenteric, lumbar (para-aortic) nodes; drain all abdominal organs
Pelvis:
- External/internal iliac nodes (parietal); paravesical, parauterine, pararectal nodes (visceral)
Lower limb:
- Superficial inguinal nodes - palpable in groin; receive lymph from superficial leg, anus, perineum, external genitalia
- Deep inguinal nodes - deep to fascia lata; Rosenmüller node in femoral canal
- Popliteal nodes (superficial and deep) - filter foot and leg
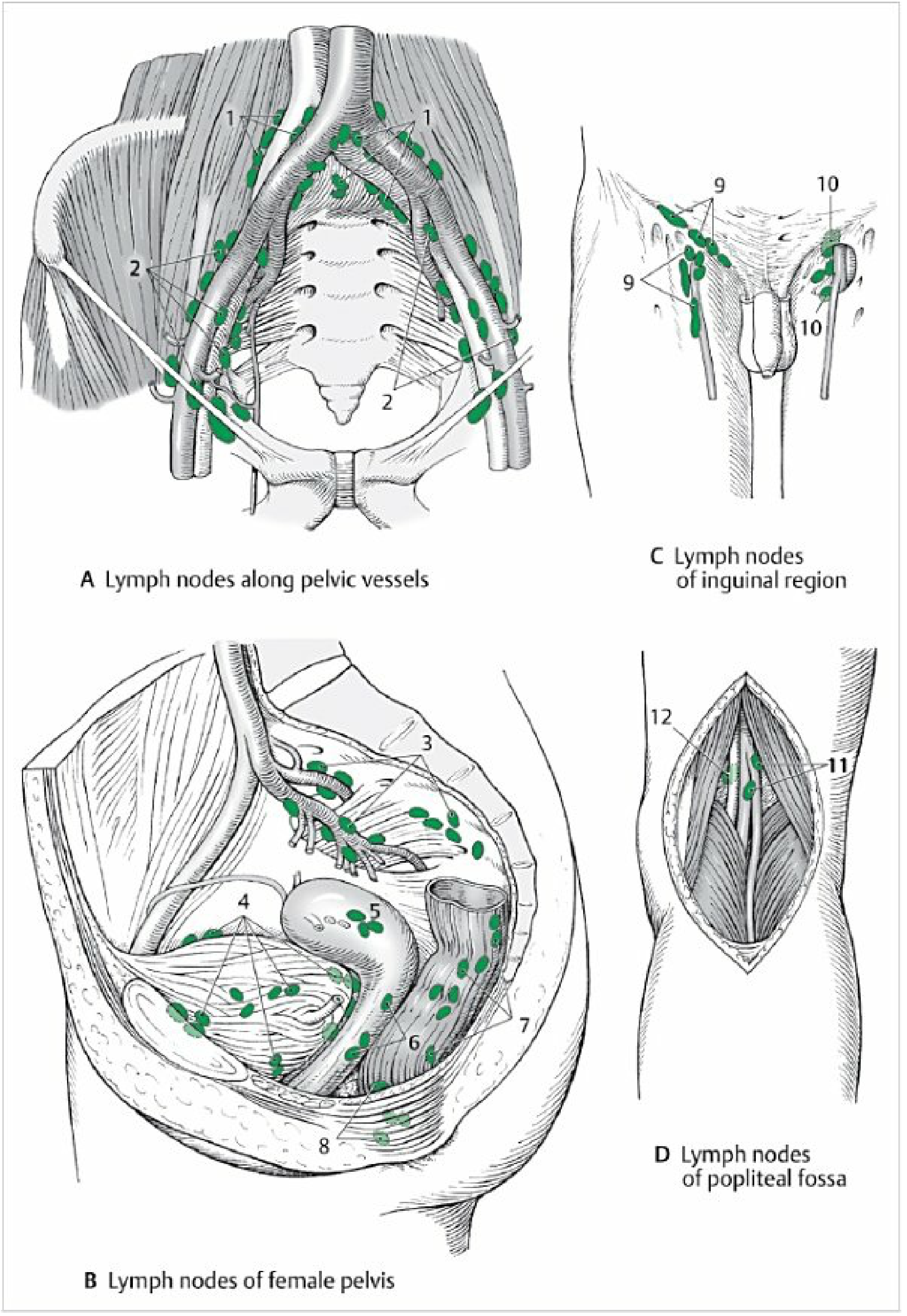
Fig. 2.40 - Regional lymph nodes of the pelvis and lower limb.
Clinical note: Precise knowledge of regional lymph nodes is essential for cancer surgery. Metastatic spread via lymphatics requires removal of both the primary organ and its regional lymph node groups.
2.11 Structure and Function of Blood and Lymphatic Vessels
The Three-Layered Vessel Wall
All blood vessels (except capillaries) share the same basic three-layer structure:
| Layer | Also Called | Composition | Function |
|---|---|---|---|
| Tunica interna | Intima | Endothelial cells on a basal lamina + subendothelial connective tissue; bounded by internal elastic lamina | Smooth blood flow; anticoagulant; endocrine functions |
| Tunica media | Media | Smooth muscle cells + elastic fibers; bounded externally by external elastic lamina | Vasomotion (vasoconstriction/dilation); determines vessel diameter and blood pressure |
| Tunica externa | Adventitia | Dense connective tissue; contains nervi vasorum and vasa vasorum | Anchors vessel; nerve supply; nutrition of vessel wall |
Vessel Type Comparison
| Type | Wall Features | Function |
|---|---|---|
| Elastic arteries (e.g., aorta) | Thick media with abundant elastic fibers | Windkessel effect: store energy during systole, maintain pressure during diastole |
| Muscular arteries (distributing) | Media predominantly smooth muscle | Regulate blood distribution to organs via vasoconstriction/dilation |
| Arterioles | Mostly smooth muscle; little elastin | Main site of peripheral resistance regulation |
| Capillaries | Single endothelial cell layer only | Gas + nutrient exchange |
| Venules | Thin walls; little smooth muscle | Collect from capillaries; site of leukocyte diapedesis |
| Veins | Thin media; large lumen; valves | Low-pressure return; blood reservoir (60-70% of blood volume) |
| Lymphatic vessels | Similar to veins; valves present; no RBCs | Return interstitial fluid to circulation; immune surveillance via lymph nodes |
Clinical note: Cardiac muscle cells cannot regenerate. Prolonged ischemia causes irreversible necrosis followed by connective tissue scarring. Even temporary ischemia causes reversible injury, but sustained ischemia (as in myocardial infarction) permanently destroys myocardium.
Source: Color Atlas of Human Anatomy, Vol. 2: Internal Organs (THIEME); General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy.
This is a shared conversation. Sign in to Orris to start your own chat.