Unilateral and bilateral superior laryngeal nerve palsy causes , clinical features and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"superior laryngeal nerve" AND palsy
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed from authoritative sources. Let me compile a comprehensive, well-structured answer.
Superior Laryngeal Nerve (SLN) Palsy
Anatomy - Quick Overview
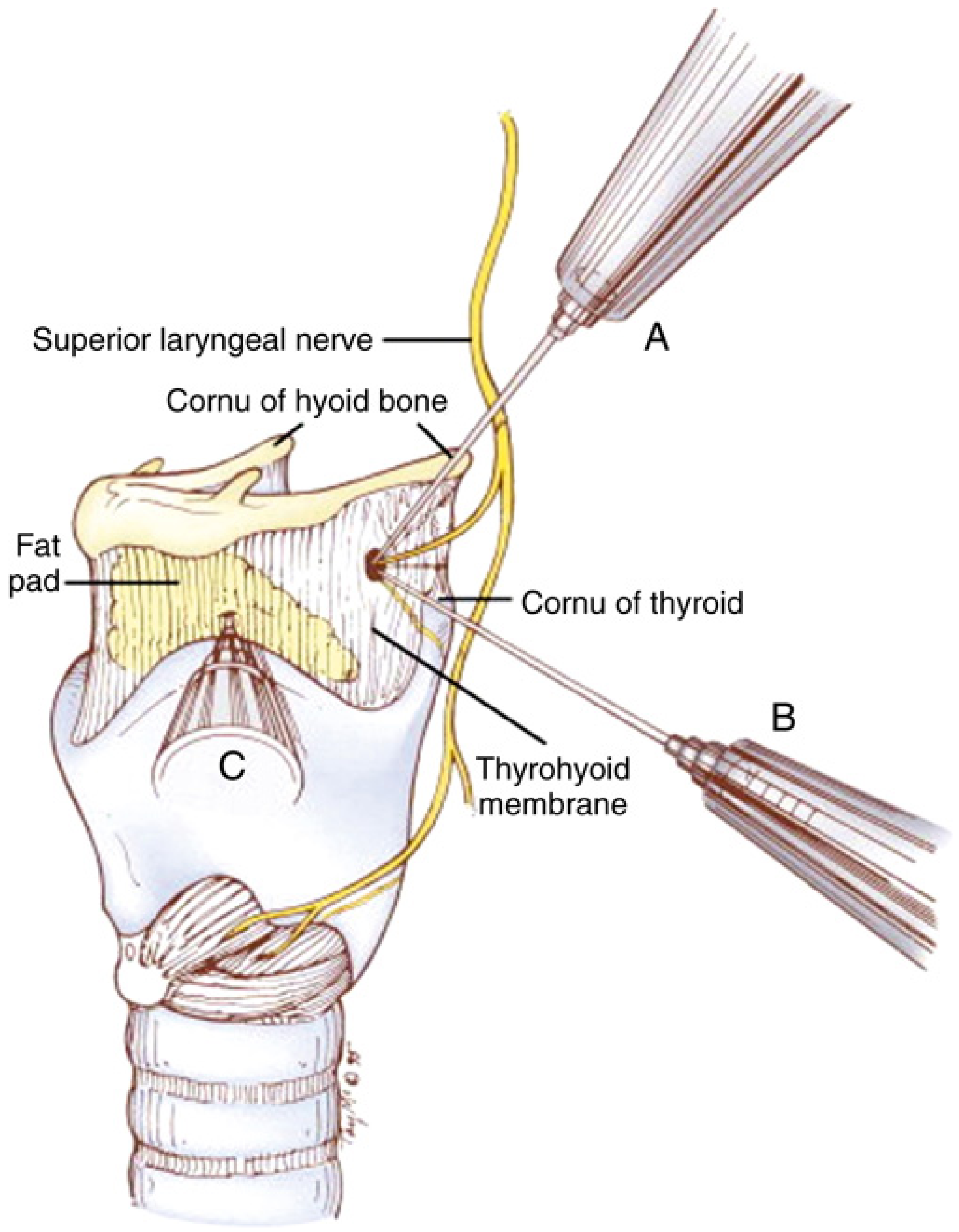
The SLN arises from the inferior (nodose) ganglion of the vagus nerve (CN X) and descends lateral to the pharynx, behind the internal carotid artery. At the level of the greater cornu of the hyoid bone, it divides into two branches:
- Internal branch (IBSLN): Larger, sensory. Pierces the thyrohyoid membrane with the superior laryngeal artery. Supplies sensation to the supraglottic mucosa - base of tongue, epiglottis, vallecula, aryepiglottic folds, piriform fossae, and laryngeal vestibule down to the vocal folds. Also carries afferents from laryngeal stretch receptors.
- External branch (EBSLN): Smaller, motor. Descends along the inferior constrictor to innervate the cricothyroid muscle (and to a lesser degree, the inferior pharyngeal constrictor). The cricothyroid muscle lengthens and tenses the vocal cords, enabling high-pitch phonation.
Causes of SLN Palsy
Both branches can be injured together or individually. Injury to the EBSLN is far more common than IBSLN injury in isolation.
Surgical / Iatrogenic (most common)
| Procedure | Mechanism |
|---|---|
| Thyroidectomy | EBSLN lies adjacent to superior thyroid pole vessels; up to 25% injury rate; in ~20% of cases the nerve travels subfascially and is visually unidentifiable |
| Carotid body tumor resection | ~5% SLN injury rate |
| Anterior cervical spine surgery | Direct stretch or retraction injury |
| Neck dissection | Disruption of nerve along carotid sheath |
| Laryngeal / pharyngeal surgery | Direct trauma |
Neoplastic
- Pharyngeal, laryngeal, thyroid, or esophageal carcinoma invading the nerve
- Skull base tumors
- Carotid body paragangliomas
- Lymph node metastases compressing the nerve
Traumatic
- Penetrating or blunt neck trauma
- Fractures of the hyoid bone or thyroid cartilage
- Difficult endotracheal intubation (stretch injury)
Inflammatory / Infectious
- Viral neuritis (e.g., post-viral neuropathy, analogous to Bell's palsy)
- Neck space infections, abscess
- Granulomatous disease (sarcoidosis, tuberculosis)
Neurological
- Stroke or other central lesions affecting the vagal nuclear complex (SLN palsy would occur as part of a broader vagal palsy)
- Damage at the skull base (jugular foramen tumors/fractures, involving CN X more broadly)
- Hereditary neuropathy with liability to pressure palsies
Idiopathic
- A number of cases have no identifiable cause (idiopathic viral neuritis is presumed)
Clinical Features
A. Unilateral SLN Palsy
Motor (EBSLN) - cricothyroid denervation:
- Reduced pitch range: Inability to produce high-pitched sounds; reduction in average fundamental frequency
- Decreased vocal power and projection
- Voice fatigue on prolonged speaking/singing
- Subtle hoarseness (mild, often overlooked)
- On laryngoscopy: the posterior commissure and glottic chink may rotate slightly toward the affected side (the contralateral cricothyroid still contracts); the paralyzed vocal cord appears bowed or slightly lax
- Clinical findings are often very subtle and may go undetected
Key point: Unilateral denervation of the cricothyroid causes "very subtle clinical findings." - Morgan & Mikhail's Clinical Anesthesiology, 7e
Sensory (IBSLN):
- Ipsilateral supraglottic hypoesthesia
- Tendency toward silent aspiration (especially thin liquids), since the protective cough reflex from the supraglottis is blunted
- Pooling of secretions in the piriform fossa on the affected side
Who is most affected clinically:
- Singers and professional voice users (opera singers, actors, teachers) notice the loss most acutely - the inability to produce sustained high notes or project the voice is career-threatening
- Pye's Surgical Handicraft notes: "This can be a serious deficit in singers or professional speakers."
B. Bilateral SLN Palsy
- Hoarseness - more prominent than with unilateral palsy
- Easy voice fatigue / easy tiring of the voice
- Loss of high-pitch phonation entirely
- Severely diminished vocal range and loudness
- Bilateral loss of supraglottic sensation - increased aspiration risk, silent penetration of the laryngeal vestibule
- Airway is NOT jeopardized (the glottis remains open via the recurrent laryngeal nerve and the posterior cricoarytenoid muscles)
"Bilateral palsy of the superior laryngeal nerve may result in hoarseness or easy tiring of the voice, but airway control is not jeopardized." - Morgan & Mikhail's Clinical Anesthesiology, 7e
Summary Table (from Morgan & Mikhail):
| Nerve Injured | Effect |
|---|---|
| SLN - Unilateral | Minimal effects |
| SLN - Bilateral | Hoarseness, easy voice fatigue |
| RLN - Unilateral | Hoarseness |
| RLN - Bilateral (acute) | Stridor, respiratory distress |
| RLN - Bilateral (chronic) | Aphonia |
C. Important Physical Examination Signs
- Videostroboscopy: Shows reduced vocal fold length and tension on the affected side; asymmetric vibration pattern; cord appears lax
- "Paralytic falsetto": Some patients with intact cricothyroid (SLN intact in co-existing RLN palsy) use the cricothyroid to increase vocal fold resistance - generating a characteristic falsetto voice. Conversely, in pure SLN palsy this falsetto capacity is lost.
- Electromyography (EMG): Cricothyroid EMG confirms EBSLN denervation - shows reduced or absent motor unit potentials
- "Eee-sniff" manoeuvre: Helps reveal vocal fold asymmetry during laryngoscopy
Management
Management is guided by the affected branch, severity, and whether the injury is temporary (neuropraxia) or permanent.
1. Initial Assessment
- Formal voice evaluation - acoustic analysis, vocal range, aerodynamic assessment
- Videostroboscopy - to assess vocal fold tension, symmetry, and closure pattern
- Flexible fiberoptic laryngoscopy - exclude concurrent RLN injury
- Laryngeal EMG - confirms denervation; helps distinguish neuropraxia (polyphasic potentials, positive sharp waves) from permanent axonotmesis
- Modified Barium Swallow (MBS) or FEES - if aspiration is suspected (particularly with IBSLN injury), to assess swallowing safety
2. Conservative / Watchful Waiting
- Most cases after thyroid surgery are a neuropraxia and spontaneous recovery can be anticipated over 3-6 months
- "The nerve can be damaged in some patients but this will often be a neuropraxia and recovery can be anticipated." - Pye's Surgical Handicraft, 22nd ed.
- Voice rest and hydration during recovery
3. Voice Therapy (Speech-Language Pathology)
- First-line active treatment for most patients
- Techniques include:
- Semi-occluded vocal tract exercises (e.g., lip trills, straw phonation)
- Pitch-glide exercises to retrain range
- Resonance and projection exercises
- Lee Silverman Voice Treatment (LSVT) style intensity training
- Compensatory strategies for aspiration: thickening liquids, chin-tuck posture, rotating head to the affected side during swallowing
4. Intraoperative Prevention (Surgical Management)
- Nerve monitoring (IONM): Intraoperative neuromonitoring of the EBSLN during thyroid surgery is strongly recommended; up to 20% of EBSLNs are subfascial and visually unidentifiable - EMG stimulation identifies them reliably
- Meticulous superior pole dissection: Ligation of superior thyroid pole vessels directly on the thyroid capsule (rather than en masse) reduces nerve injury risk
- Identification in Joll's triangle: The sternothyrolaryngeal (Joll's) triangle - bounded by the superior thyroid pedicle, cricothyroid muscle, and lower edge of thyroid cartilage - is the surgical landmark for EBSLN identification
5. Surgical Rehabilitation (for Permanent Injury)
- Medialization laryngoplasty / vocal cord augmentation: If concurrent RLN injury is present with SLN injury, the cord is more laterally positioned and voice/glottic competence is worse; medialization helps
- Arytenoid adduction may be considered in selected cases with significant glottic insufficiency
- Reinnervation procedures are investigational for combined SLN+RLN injuries
- Cricopharyngeal myotomy may help in cases where bilateral sensory loss leads to intractable aspiration
6. Management of Aspiration (IBSLN injury)
- Thickening of liquids (provides more time for pharyngeal response)
- Swallowing with chin tucked and head rotated to the affected side (routes bolus to the contralateral pyriform sinus)
- Referral to speech-language pathology for swallowing rehabilitation
Key Clinical Distinctions
| Feature | Unilateral SLN Palsy | Bilateral SLN Palsy |
|---|---|---|
| Voice change | Minimal / subtle pitch reduction | Hoarseness + severe pitch range loss |
| Voice fatigue | Yes | Yes (prominent) |
| Airway compromise | None | None |
| Aspiration risk | Mild (unilateral sensory loss) | Higher (bilateral sensory loss) |
| Laryngoscopy finding | Subtle cord laxity, posterior glottic rotation | Bilateral cord laxity |
| Who notices most | Singers/professional speakers | All patients |
Sources:
- Localization in Clinical Neurology, 8e, p. 871 - Lesions of the Superior Laryngeal Nerve
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 568 - Table 19-1 Laryngeal Nerve Injury Effects
- Cummings Otolaryngology Head and Neck Surgery - Superior Laryngeal Nerve Injury
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 - EBSLN Injury and IONM
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vocal Fold Paralysis, Physical Examination
- K.J. Lee's Essential Otolaryngology - Pharyngeal Sensory Loss, SLN Anatomy
- Pye's Surgical Handicraft, 22nd ed. - Superior Laryngeal Nerve
- Mulholland & Greenfield's Surgery, 7e - Nerves of the Thyroid
- Barash's Clinical Anesthesia, 9e - Airway Management
This is a shared conversation. Sign in to Orris to start your own chat.