
What is possible diagnosis of this nail discoloration..
toenail discoloration subungual dark greenish brown discoloration onychomycosis
Hugging Face pmc clinical VQA raw
Page 0
toenail discoloration differential diagnosis onychomycosis subungual hematoma melanonychia green nail
Diagnosis and Management of Melanoma
Page 334
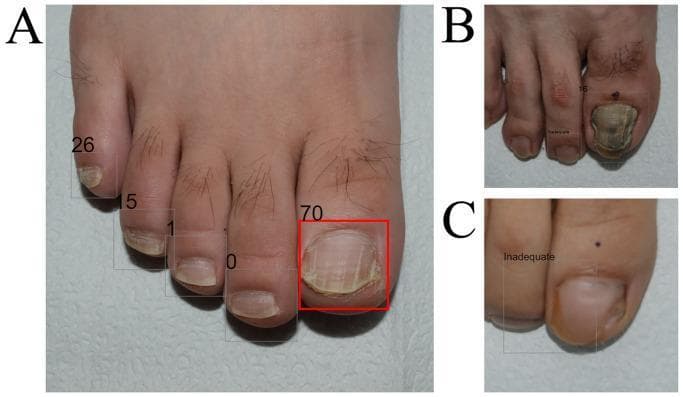
Nail Discoloration — Differential Diagnosis
- Large toenail (hallux) with greenish-brown to dark discoloration, predominantly at the medial/proximal aspect
- Nail plate dystrophy with cracking and surface irregularity
- Partial onycholysis (nail plate separation from the nail bed)
- Surrounding soft tissue appears mildly inflamed/swollen
Most Likely Diagnoses
| Diagnosis | Features Supporting It | Features Against |
|---|---|---|
| Onychomycosis (Tinea unguium) | Dystrophy, thickening, yellowish-white areas, nail plate crumbling, common in toenails | Green tinge less typical without secondary infection |
| Pseudomonas aeruginosa nail infection (Chloronychia / "Green Nail Syndrome") | Greenish-brown/black discoloration under nail, onycholysis, can co-occur with fungal infection | Usually green is more vivid; typically in fingernails but can occur in toes |
| Subungual hematoma | Dark discoloration (blood pooling under nail), trauma history, seen in great toe | Blood usually reddish-purple, not greenish |
| Subungual melanoma | Dark pigmentation under nail, nail dystrophy | No visible longitudinal melanonychia band; Hutchinson's sign not visible |
Most Probable Diagnosis
- The greenish-brown hue — the green color is pathognomonic of Pseudomonas aeruginosa pigment (pyocyanin/pyoverdine) accumulating in the subungual space
- The associated nail dystrophy, crumbling, and onycholysis — classic for fungal nail disease, which predisposes to secondary bacterial colonization
- Location on the hallux — the most commonly affected toe in onychomycosis
Other Conditions to Consider
- Traumatic onycholysis — repeated microtrauma (tight footwear) can cause separation and secondary discoloration
- Contact with topical agents (e.g., potassium permanganate, certain dyes)
- Yellow nail syndrome — rare; associated with lymphedema and respiratory conditions
Recommended Workup
- KOH preparation / fungal culture — from nail clippings and subungual debris to confirm onychomycosis
- Bacterial culture / swab — to confirm Pseudomonas and guide antibiotic choice
- Dermoscopy — to exclude subungual melanoma if dark pigmentation persists after treatment
- Nail plate biopsy with PAS stain — if initial cultures are negative and diagnosis remains uncertain
⚠️ This is for educational purposes only. A formal diagnosis requires in-person clinical examination, history, and laboratory confirmation by a qualified clinician.
Probable treatment
onychomycosis treatment antifungal terbinafine itraconazole topical systemic
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 6315
green nail syndrome Pseudomonas chloronychia treatment antibiotics topical
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 4840
onychomycosis terbinafine itraconazole pulse therapy duration cure rate toenail
Pseudomonas nail infection topical ciprofloxacin acetic acid treatment management
Treatment Plan
Step 1 — Address the Pseudomonas Infection First
| Approach | Details |
|---|---|
| Trim/debride the nail | Remove as much of the separated, dystrophic nail plate as possible to eliminate the moist subungual environment |
| Topical acetic acid soaks | 1–2% acetic acid (dilute white vinegar) soaks for 10–15 min twice daily — directly bactericidal against Pseudomonas |
| Topical ciprofloxacin/gentamicin ear/eye drops | Applied under the lifted nail edge twice daily; highly effective for localized Pseudomonas nail infections |
| Oral ciprofloxacin | 500–750 mg twice daily × 2–3 weeks if infection is extensive or non-responsive to topical treatment |
| Keep nail dry | Moisture perpetuates Pseudomonas colonization — avoid prolonged wet exposure |
Per Harrison's Principles of Internal Medicine (p. 4840): the green discoloration in green nail syndrome results from pyocyanin diffusion into the nail bed from P. aeruginosa.
Step 2 — Treat the Underlying Onychomycosis (Fungal Component)
Systemic Antifungals (First-line for toenail)
| Drug | Regimen | Duration | Notes |
|---|---|---|---|
| Terbinafine (preferred) | 250 mg/day orally | 12 weeks for toenail | Highest mycological cure rates (~70–80%); fungicidal |
| Itraconazole | 200 mg/day continuously × 12 weeks OR pulse: 400 mg/day × 1 week/month × 3–4 months | 12 weeks or 3–4 pulse cycles | Fungistatic; check drug interactions |
Per Harrison's (p. 6315): "Itraconazole and terbinafine both accumulate in the nail plate" — this is why shorter courses can have prolonged effects.
Topical Antifungals (Adjunct or mild cases)
| Drug | Regimen | Notes |
|---|---|---|
| Efinaconazole 10% solution | Apply to affected nail daily × 48 weeks | Evidence-based per Harrison's; best penetration of topicals |
| Ciclopirox 8% nail lacquer | Apply daily, remove weekly × 48 weeks | Less effective for toenail alone; useful as adjunct |
| Tavaborole 5% solution | Apply daily × 48 weeks | Newer agent with good nail penetration |
Step 3 — Supportive Measures
- Nail trimming and debridement at regular intervals (by podiatrist if needed) to remove infected nail material
- Footwear hygiene: wear moisture-wicking socks, avoid tight shoes, use antifungal foot powder
- Treat tinea pedis if present concurrently (topical clotrimazole/terbinafine cream) — untreated athlete's foot is a major source of reinfection
- Avoid walking barefoot in communal areas (gyms, pools)
Monitoring & Follow-up
| Timepoint | Action |
|---|---|
| Baseline | LFTs before starting oral terbinafine/itraconazole (hepatotoxicity risk) |
| 6 weeks | Clinical response check; repeat LFTs if symptomatic |
| 3 months | Assess mycological cure (repeat KOH/culture) |
| 12–18 months | Full nail regrowth expected — final cosmetic assessment |
When to Refer
- No response after 3 months of systemic therapy → consider nail biopsy with PAS stain
- Suspicion of subungual melanoma → urgent dermatology/oncology referral
- Significant paronychia or cellulitis → podiatry or dermatology
⚠️ This information is for educational purposes. Treatment should be individualized by a qualified clinician after culture confirmation and assessment of contraindications (e.g., hepatic disease, drug interactions).