Carcinoid tumor in GIT PATHOLOGY according to definition pathogensis cf and morpholoy
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive data from Robbins Pathology and Quick Compendium. Let me compile the full answer.
Carcinoid Tumor (Neuroendocrine Tumor) of the GIT - Pathology
Definition
Carcinoid tumors (now officially termed Neuroendocrine Tumors, NETs) are neoplasms arising from neuroendocrine cells scattered throughout the GIT (and other organs such as the lung, pancreas, and ovary). The term "carcinoid" was historically used because these tumors grow more slowly than carcinomas. The current WHO classification designates them as low- or intermediate-grade neuroendocrine tumors. High-grade neuroendocrine tumors are termed neuroendocrine carcinomas and resemble small-cell carcinoma of the lung.
- Carcinoid tumors are specifically composed of neoplastic enterochromaffin (EC) cells, capable of producing hormonal substances including serotonin (5-HT), histamine, dopamine, and tachykinins.
"Neuroendocrine tumors, also referred to as carcinoid tumors, are neoplasms that arise from the neuroendocrine cells that are located in many organs, including the endocrine pancreas and the gut."
- Robbins & Kumar Basic Pathology, p. 559
Pathogenesis
Cell of Origin
- Arise from enterochromaffin (Kulchitsky) cells - APUD (Amine Precursor Uptake and Decarboxylation) cells scattered in the intestinal mucosa.
Hormone-Driven Hyperplasia (a key mechanism)
- In some cases, hormones drive hyperplasia of neuroendocrine cells before neoplastic transformation. Classic example: Gastric carcinoids arising in autoimmune gastritis - the associated achlorhydria leads to compensatory hypergastrinemia, which stimulates enterochromaffin-like (ECL) cell hyperplasia and eventual tumor formation.
Hormone Products
- Midgut carcinoids (distal duodenum, jejunum, ileum, appendix, right colon): primarily produce serotonin (5-HT) in large quantities.
- Foregut carcinoids (stomach, proximal duodenum, lung): may produce histamine, catecholamines, and 5-hydroxytryptophan (5-HTP) - not serotonin directly.
- Hindgut carcinoids (appendix, colorectum): most often nonsecretory.
Serotonin Metabolism Pathway
- Tumor secretes serotonin → released into portal circulation
- Liver metabolizes it (first-pass effect) → normally inactivated
- If liver metastases occur → serotonin escapes into systemic circulation → Carcinoid syndrome
- Serotonin → taken up by platelets (stored in dense granules)
- In renal tubules → converted to 5-HIAA (5-hydroxyindoleacetic acid) by MAO and aldehyde dehydrogenase
- 5-HIAA in urine = diagnostic marker (may be false-negative in 20-30%, especially foregut and hindgut tumors)
Other markers: Chromogranin A (CGA) - used for tumor burden and treatment response; Synaptophysin; Neuropeptide K; Pancreatic polypeptide (PP).
Clinicopathological Features (CF)
Epidemiology
- Peak incidence: 6th decade (but may occur at any age)
- Most common GIT site: Small intestine (>40%)
- Next: Tracheobronchial tree / lungs
Location-Based Prognosis (The Most Important Prognostic Factor)
| Location | Behavior |
|---|---|
| Foregut (stomach, proximal duodenum, esophagus) | Rarely metastasize; generally cured by resection |
| Midgut (small bowel, appendix, right colon) | May metastasize; appendiceal tumors almost uniformly benign |
| Hindgut (appendix, colorectum) | Usually incidental; appendiceal = benign course; rectal = rare metastasis |
Carcinoid Syndrome
Caused by vasoactive substances (primarily serotonin) secreted by tumors with hepatic metastases:
- Cutaneous flushing and sweating
- Bronchospasm
- Colicky abdominal pain and diarrhea
- Right-sided cardiac valvular fibrosis (endocardial fibrosis of tricuspid and pulmonary valves)
- Occurs in <10% of patients - almost always indicates hepatic metastatic disease
- Carcinoid crisis = life-threatening; sudden flushing, hypotension/hypertension, even cardiac arrest - treated with Octreotide (Sandostatin)
Gastrinoma (Zollinger-Ellison Syndrome)
- Rare gastrin-producing foregut NETs
- Features: refractory peptic ulcers, GERD, diarrhea due to excessive gastric acid inactivating pancreatic enzymes
Morphology
Gross
- Intramural or submucosal masses forming small polypoid lesions
- Yellow or tan in color on cut section
- Elicit an intense desmoplastic reaction → may cause kinking of the bowel and obstruction
Microscopy
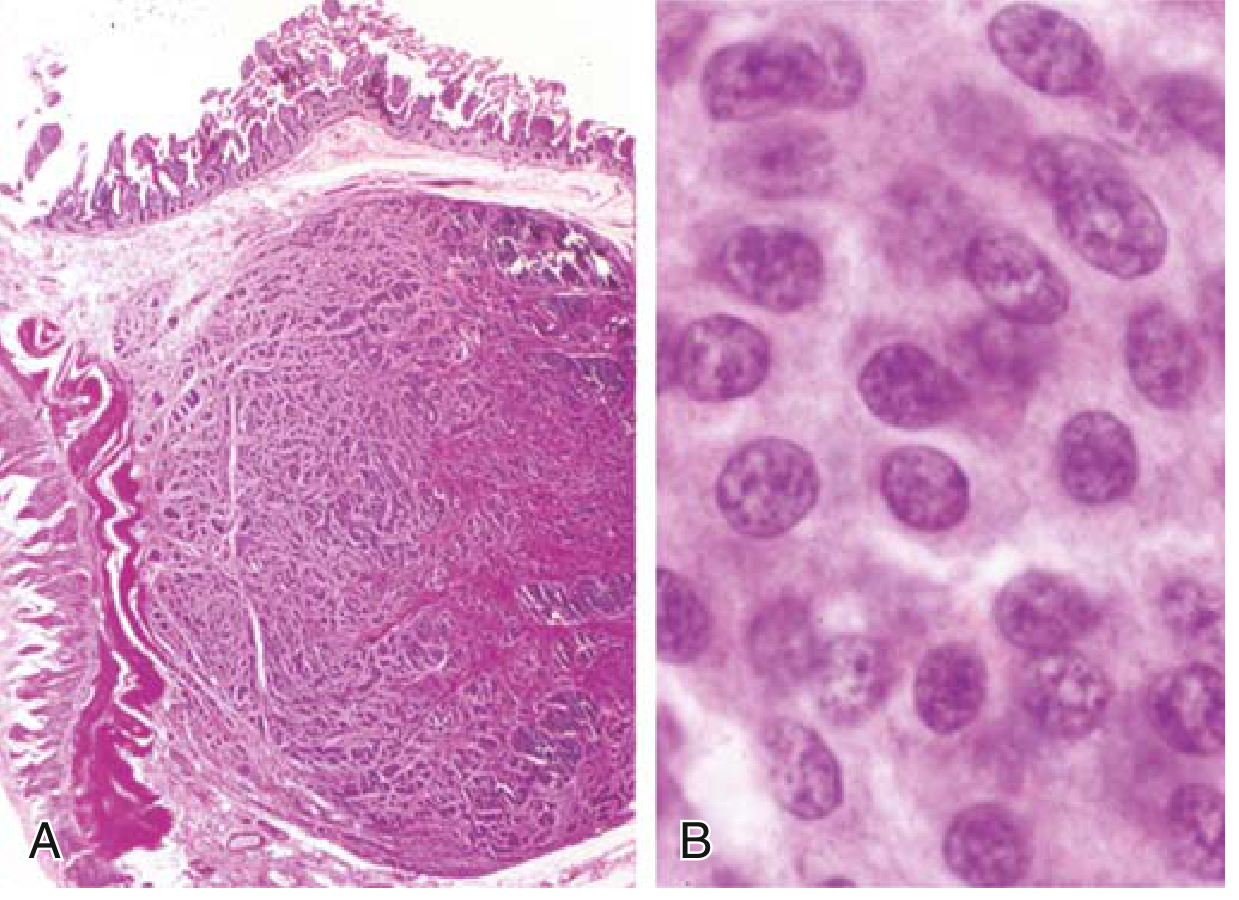
FIG. 13.17 - Robbins Pathology: (A) Carcinoid tumors often form a submucosal nodule composed of tumor cells embedded in dense fibrous tissue. (B) High magnification shows bland cytology typical of neuroendocrine tumors.
Histological features:
- Cells arranged in islands, trabeculae, strands, glands, or sheets
- Uniform cells with:
- Scant pink granular cytoplasm (neurosecretory granules)
- Round-to-oval stippled nucleus ("salt-and-pepper" chromatin pattern)
- Bland cytology - no significant pleomorphism (distinguishes low/intermediate grade from neuroendocrine carcinoma)
Summary Table
| Feature | Detail |
|---|---|
| Cell of origin | Enterochromaffin (Kulchitsky/APUD) cells |
| WHO term | Neuroendocrine tumor (NET) - low/intermediate grade |
| Most common GIT site | Small intestine (>40%) |
| Main hormone | Serotonin (5-HT) - midgut; histamine - foregut |
| Gross appearance | Yellow/tan submucosal polyp; desmoplastic |
| Histology | Islands/trabeculae; uniform cells; "salt-and-pepper" nuclei |
| Carcinoid syndrome | Only with liver metastases; <10% of patients |
| Best urine marker | 5-HIAA (urinary) |
| Best serum marker | Platelet serotonin (most accurate); Chromogranin A |
| Worst prognosis site | Midgut (ileum) - highest rate of metastasis |
| Best prognosis | Appendiceal carcinoids - almost uniformly benign |
Sources: Robbins & Kumar Basic Pathology, p. 559-560; Quick Compendium of Clinical Pathology, 5th ed., p. 37; Yamada's Textbook of Gastroenterology, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.