Secondary arterial hypertension
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from Harrison's, the NKF Primer on Kidney Diseases, and Robbins Pathology. I can synthesize a thorough response.
Secondary Arterial Hypertension
Secondary hypertension is defined as hypertension with an identifiable, often correctable underlying cause. It accounts for approximately 10% of all hypertension in adults, but this figure likely underestimates the true prevalence given historical underdiagnosis of primary aldosteronism and sleep apnea. In children, secondary causes are the rule rather than the exception — up to 90% of young children with hypertension have an identifiable secondary cause, most commonly structural kidney disease.
When to Suspect Secondary Hypertension
Secondary hypertension should be considered in:
- Treatment-resistant hypertension (BP uncontrolled on ≥3 agents including a diuretic)
- Abrupt worsening of previously controlled hypertension
- Disproportionate target organ damage for the level of BP
- Abnormal laboratory findings: unprovoked hypokalemia, proteinuria, left ventricular hypertrophy
- Onset in young patients (<30 years), especially with no family history
- Hypertension in children (always warrants secondary cause workup)
— Harrison's Principles of Internal Medicine, 22e | NKF Primer on Kidney Diseases, 8e
Major Causes and Pathophysiology
1. Obstructive Sleep Apnea (OSA)
Most common secondary cause. Present in >30% of hypertensive adults in the US.
- Mechanism: Intermittent hypoxia → sympathetic nervous system activation → increased vascular tone, volume retention, RAAS dysregulation
- Direct association between OSA severity and BP level/treatment resistance
- Nearly 75% of OSA patients are overweight or obese
- Screening: Epworth sleepiness scale, polysomnography (sleep study)
- Treatment: Lifestyle modification, weight loss; CPAP (modest BP-lowering effect, ~2–3 mmHg)
— Harrison's Principles of Internal Medicine, 22e
2. Renovascular Hypertension / Renal Artery Stenosis
Mechanism: Stenosis of one or both renal arteries → decreased glomerular perfusion → reduced pressure at afferent arteriole → renin secretion → Angiotensin I → Angiotensin II (via ACE in lung endothelium) → vasoconstriction + aldosterone release → Na⁺/H₂O retention → ↑ blood pressure (see RAAS diagram below).
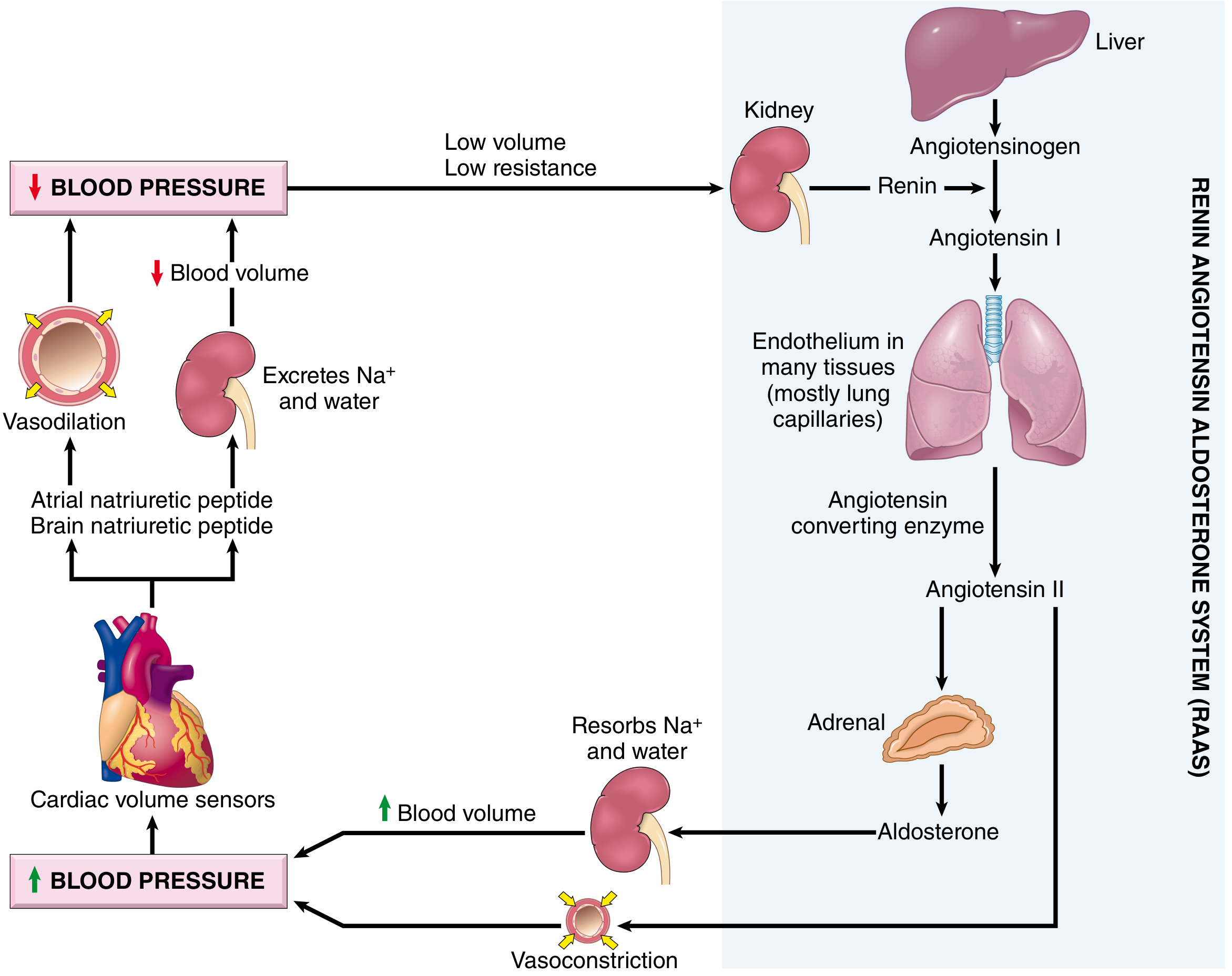
- Causes: Atherosclerotic plaques (elderly), fibromuscular dysplasia (young women)
- Clues: Abdominal bruit, flash pulmonary edema, worsening renal function on ACE inhibitor/ARB, hypokalemia
- Screening: Renal Doppler ultrasound, CT angiography, MR angiography
- Treatment: Percutaneous transluminal angioplasty ± stenting; ACE inhibitors/ARBs (caution in bilateral stenosis)
3. Primary Aldosteronism (Hyperaldosteronism)
One of the most frequent secondary causes (~20% of resistant hypertension cases).
- Mechanism: Autonomous aldosterone overproduction (idiopathic bilateral hyperplasia ~60–70%; adrenal adenoma [Conn syndrome] ~30–40%; rarely adrenocortical carcinoma) → Na⁺/H₂O retention + K⁺ excretion → volume expansion + suppressed plasma renin
- Clues: Unprovoked hypokalemia, muscle weakness, polyuria, metabolic alkalosis; BP may be severe
- Screening: Aldosterone-to-renin ratio (ARR) — elevated in primary aldosteronism; confirm with salt-loading or fludrocortisone suppression test
- Imaging: CT adrenal; adrenal vein sampling for lateralization
- Treatment: Unilateral adenoma → adrenalectomy (potentially curative); bilateral hyperplasia → mineralocorticoid receptor antagonists (spironolactone, eplerenone)
4. Chronic Kidney Disease (CKD) / Renoparenchymal Hypertension
Most common secondary cause when considering all comorbidities.
- Mechanism: ↓ GFR → Na⁺/H₂O retention → volume overload + RAAS activation + sympathetic overactivity
- Clues: Proteinuria, elevated creatinine/BUN, anemia, history of kidney disease
- Treatment: Salt restriction, diuretics, ACE inhibitors/ARBs (preferred, also reduce proteinuria)
5. Pheochromocytoma / Paraganglioma
Rare (0.1–0.6% of hypertensive patients) but potentially lethal if missed.
- Mechanism: Catecholamine excess (epinephrine, norepinephrine) → α- and β-adrenergic receptor activation → severe vasoconstriction + ↑ cardiac output
- Clues: Paroxysmal hypertension, headache, diaphoresis, palpitations ("the 5 Ps"): also pallor, pressure rises with palpation; possible familial (MEN2, VHL, SDH mutations)
- Screening: 24-hour urine or plasma fractionated metanephrines (most sensitive)
- Imaging: CT/MRI adrenal; MIBG scintigraphy or PET for extraadrenal disease
- Treatment: Surgical resection after α-blockade (phenoxybenzamine or doxazosin) + β-blockade
6. Cushing Syndrome (Hypercortisolism)
- Mechanism: Glucocorticoid excess → Na⁺ retention + mineralocorticoid receptor activation + increased angiotensinogen synthesis + sympathetic potentiation
- Clues: Central obesity, striae, proximal myopathy, moon face, buffalo hump, hyperglycemia, osteoporosis
- Screening: 24-hour urine free cortisol; late-night salivary cortisol; 1 mg overnight dexamethasone suppression test
- Treatment: Remove source (pituitary adenoma, adrenal adenoma, ectopic ACTH tumor); metyrapone/ketoconazole as bridge
7. Thyroid and Parathyroid Disorders
- Hypothyroidism: ↑ diastolic BP (peripheral vasoconstriction, decreased cardiac output) — TSH screening
- Hyperthyroidism: ↑ systolic BP (↑ heart rate + cardiac output) — isolated systolic hypertension pattern; treat underlying thyroid disease
- Primary hyperparathyroidism: ↑ Ca²⁺ → vasoconstriction; screen with serum calcium
8. Coarctation of the Aorta
- Congenital narrowing of the aorta (classically at the level of the ductus arteriosus)
- Clues: Upper-limb hypertension with weak/delayed femoral pulses, BP differential between arms and legs, rib notching on CXR, systolic murmur
- Treatment: Percutaneous balloon dilation/stenting or surgical repair — potentially curative if corrected early
9. Drug-Induced and Exogenous Causes
Common drugs elevating BP:
| Category | Examples |
|---|---|
| NSAIDs | Ibuprofen, naproxen (Na⁺ retention, blunt antihypertensive drugs) |
| Sympathomimetics | Decongestants (pseudoephedrine), cocaine, amphetamines |
| Hormonal | Oral contraceptives, androgens, erythropoietin |
| Immunosuppressants | Cyclosporine, tacrolimus |
| Stimulants | Caffeine (acute), methylphenidate |
| Herbal | Licorice (glycyrrhizin → mineralocorticoid effect) |
— Fuster and Hurst's The Heart, 15th Edition | Harrison's 22e
10. Monogenic (Single-Gene) Disorders
Rare but mechanistically important:
- Liddle syndrome: ENaC-γ gain-of-function mutation → excessive distal Na⁺ reabsorption, low renin/aldosterone, hypokalemia
- Glucocorticoid-remediable aldosteronism (GRA/FH-I): Chimeric gene → ACTH-regulated aldosterone synthesis
- 11β-hydroxylase / 17α-hydroxylase deficiency: Congenital adrenal hyperplasia variants with mineralocorticoid excess
- Gordon syndrome (pseudohypoaldosteronism type II): WNK kinase mutations → ↑ NaCl reabsorption, hyperkalemia, hypertension
Diagnostic Approach
| Setting | Initial Workup |
|---|---|
| All hypertensive patients | Urinalysis, serum creatinine/eGFR, electrolytes, fasting glucose, lipids, ECG |
| Resistant or young-onset HTN | Aldosterone-to-renin ratio, renal Doppler |
| Hypokalemia | ARR, confirm primary aldosteronism |
| Paroxysmal HTN/symptoms | Plasma/urine metanephrines |
| Central obesity + striae | 24h urine cortisol, dexamethasone suppression |
| Upper/lower limb BP differential | Echo/CXR for coarctation |
| Snoring + daytime sleepiness | Polysomnography (OSA) |
The second critical opportunity to diagnose secondary hypertension is in patients with resistant hypertension — those whose BP remains above target despite ≥3 antihypertensives at optimal doses. In this setting, primary aldosteronism accounts for ~20%, renovascular disease ~25%, and OSA >50%.
— NKF Primer on Kidney Diseases, 8e
Key Takeaways
- Secondary hypertension is potentially curable — early identification matters
- "Classic" curable causes: primary aldosteronism, renal artery stenosis, pheochromocytoma, Cushing syndrome, coarctation, acute GN
- Associated causes (correction may not fully resolve BP): CKD, OSA, obesity
- The RAAS is the central shared mechanistic pathway for most renal and adrenal causes
- Always revisit secondary causes in resistant hypertension and hypertension in the young
This is a shared conversation. Sign in to Orris to start your own chat.