Autoimmune hepatitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of autoimmune hepatitis (AIH), synthesized from multiple textbooks.
Autoimmune Hepatitis
Definition
Autoimmune hepatitis is a chronic, progressive inflammatory liver disorder characterized by autoimmune reactions against normal hepatocytes, the presence of circulating autoantibodies, elevated serum immunoglobulins, and responsiveness to immunosuppression. It frequently co-exists with other autoimmune diseases.
— Goldman-Cecil Medicine, p. 1583 | Robbins & Kumar Basic Pathology, p. 607
Epidemiology
- Incidence: ~1.7 per 100,000/year
- Strong female predominance (78%)
- Bimodal age distribution: 15–25 years and 45–60 years
- One of three major autoimmune liver diseases, alongside primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC)
Pathogenesis
Believed to result from autoimmune reactions against hepatocyte antigens in genetically predisposed individuals, possibly triggered by environmental factors. HLA associations:
- HLA B8, DR3, DR52a (Western populations)
- HLA DR4 (Asian populations)
Classification: Two Types
| Feature | Type 1 (~90%) | Type 2 |
|---|---|---|
| Typical age | Adults | Children/teenagers |
| Key autoantibodies | ANA, ASMA (65%), anti-actin, anti-SLA/LP (25–35%) | Anti-LKM-1, Anti-LC1, Anti-SLA/LP |
| ANA/ASMA titer | ≥1:80 (>1:20 in children) | Absent |
Note: Autoantibodies are not detected in 20–35% of all cases, so their absence does not exclude the diagnosis.
Clinical Presentation
Presentations span a wide spectrum:
- Asymptomatic — incidentally found elevated transaminases
- Acute hepatitis — fatigue and jaundice (most common symptomatic presentation)
- Acute liver failure (rare)
- Chronic hepatitis progressing to cirrhosis
AIH tends to be more severe at onset than chronic hepatitis B or C. Elevated bilirubin or alkaline phosphatase indicates more severe/advanced disease. Marked elevation of serum γ-globulin (IgG) is characteristic.
Up to 30% of adults have cirrhosis at the time of diagnosis.
Diagnosis
Diagnosis requires a combination of four features:
- Autoantibodies (ANA, ASMA, anti-LKM-1, anti-SLA/LP)
- Elevated serum IgG
- Characteristic pathologic findings on liver biopsy
- Exclusion of viral hepatitis and drug-induced liver injury
Liver biopsy is the key diagnostic tool. Noninvasive fibrosis markers (transient elastography, MR elastography) correlate with histologic stage but may be impaired by active inflammation at diagnosis.
Histopathology
AIH shares injury patterns with viral hepatitis but has characteristic features:
- Interface hepatitis (periportal necrosis/inflammation) — often extensive
- Confluent necrosis — perivenular or bridging
- Plasma cell predominance in the mononuclear infiltrate (hallmark)
- Hepatocyte "rosettes" — circular arrangements of regenerating hepatocytes around a dilated canaliculus
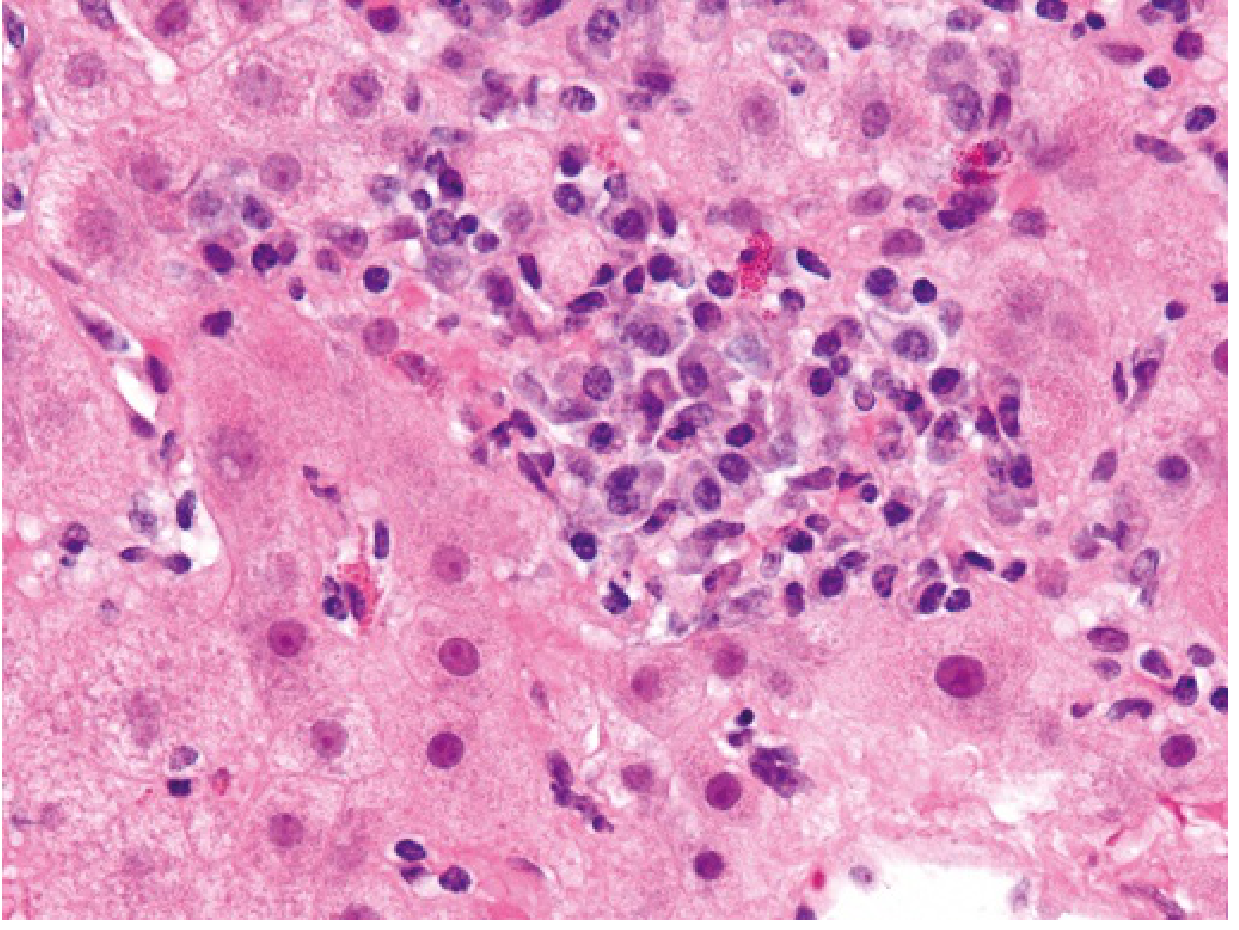
Lobular hepatitis with prominent plasma cells, typical of autoimmune hepatitis. — Robbins & Kumar Basic Pathology, p. 607
Treatment
First-line
- Prednisone/prednisolone 0.5–1.0 mg/kg/day (induction)
- Add azathioprine 1.0–2.0 mg/kg/day gradually (~2 weeks after steroid initiation), while tapering steroids
- Budesonide (3 mg TID, reduced to BID on remission) can replace prednisone in patients without cirrhosis and without acute severe AIH, combined with azathioprine
- Target: normalize ALT and IgG levels
Second-line (failure, incomplete response, or intolerance)
- Mycophenolate mofetil (up to 3 g/day)
- Tacrolimus (1–8 mg/day)
Third-line
- Infliximab or rituximab after first- and second-line failure
Remission and withdrawal
- After ≥3 years of remission, therapy may be carefully withdrawn
- Caution: severe and even fatal flares can occur weeks to months after withdrawal
Prognosis
- Immunosuppressive therapy achieves remission in ~90% of patients, including those with cirrhosis at diagnosis
- A small subset has overlap syndrome with features of PBC or PSC
- End-stage disease → liver transplantation
- 10-year post-transplant survival: 75%
- Recurrence in the transplanted liver: ~20%
Sources: Robbins & Kumar Basic Pathology (p. 607); Goldman-Cecil Medicine (p. 1583); Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.