Types of stoma and selection of stoma during procedure and difference between them
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
types of intestinal stoma colostomy ileostomy loop end double barrel diagram
I now have comprehensive content from Sabiston's surgical textbook and clinical images. Let me compile a thorough, well-structured answer.
Types of Stoma: Classification, Selection, and Differences
A stoma is a surgically created opening of the bowel (or urinary tract) onto the abdominal wall. Stomas can be classified across several dimensions.
I. Classification by Content Drained
1. Fecal Stomas
a. Ileostomy
- Created from the ileum (small bowel)
- Output is liquid to semi-liquid, high-volume, and contains active digestive enzymes — corrosive to peristomal skin
- Requires a spouted/everted maturation (Brooke ileostomy) to protect skin from liquid effluent
- Located in the right iliac fossa
- More common as a temporary diverting stoma
b. Colostomy
- Created from the colon
- Output varies by location:
- Ascending colostomy: liquid effluent (rarely used; poorly tolerated)
- Transverse colostomy: semi-formed; prone to prolapse — generally avoided
- Descending / Sigmoid colostomy: formed stool; preferred when permanent colostomy is needed
- Located in the left iliac fossa (for sigmoid/descending)
- Typically flush with skin (does not need to be spouted)
"Ascending colostomies tend to have a higher amount of liquid effluent, whereas descending and left-sided colostomies are usually preferable because most of the colon is in circuit, allowing for more colonic water absorption, with a more formed effluent." — Sabiston Textbook of Surgery, p. 2073
2. Urinary Stomas
- Ileal conduit (urostomy): segment of ileum used to divert urine; output is continuous and watery
- Described in urologic surgery for bladder removal (e.g., cystectomy)
II. Classification by Configuration
1. End Stoma
- The proximal cut end of bowel is brought through the abdominal wall; distal end is either removed or closed (Hartmann's pouch)
- Single lumen visible
- Used for permanent stomas (e.g., after APR for rectal cancer) or when distal bowel is resected
- Simpler appliance management; easier pouch adherence
Clinical photograph — End ileostomy:

2. Loop Stoma
- A loop of bowel is brought through the abdominal wall and opened; both lumens (proximal/afferent and distal/efferent) are visible on the surface, connected by an intact posterior wall
- A stoma rod/bridge is placed under the loop temporarily to prevent retraction
- Predominantly temporary — used for fecal diversion
- Easier to close than an end stoma
- Loop ileostomy is preferred for temporary diversion: odorless, easy to manage, easy to reverse
- Loop transverse colostomy should be avoided — large, prone to prolapse, difficult pouching (often at belt line)
Clinical photograph — Loop ileostomy with stoma rod:

3. Double-Barrel Stoma
- The bowel is completely divided; both ends are brought out as two separate stomas on the abdominal wall (proximal functioning limb + distal mucous fistula)
- Two discrete lumens — no intact posterior wall (distinguishes it from a loop stoma)
- Chosen in emergency cases, significant inflammation, complex procedures, or when there is concern about anastomotic integrity
- Provides complete fecal diversion
Clinical photograph — Double-barrel ileostomy:

4. End-Loop Stoma
- A hybrid: the loop is brought through the fascia and the mesenteric side is oversewn so that only the functioning end is opened
- Useful in obese patients where mobilizing enough colon for a true end stoma is technically difficult
- Provides the pouching advantages of an end stoma while requiring less bowel length
III. Classification by Permanence
| Feature | Temporary Stoma | Permanent Stoma |
|---|---|---|
| Purpose | Protect distal anastomosis; treat sepsis/emergency | Bowel/bladder removed or irreversible disease |
| Common types | Loop ileostomy, loop sigmoid colostomy | End sigmoid colostomy (APR), end ileostomy (panproctocolectomy) |
| Closure | Planned at 8–12 weeks post-op | Not closed |
| Preferred choice | Loop ileostomy (low odor, easy closure) | Left-sided colostomy (formed stool) |
IV. Classification by Continence
| Type | Description |
|---|---|
| Incontinent (conventional) | Passive drainage into an external pouching system; most common |
| Continent stoma (Kock pouch) | Internal reservoir with a nipple valve; patient catheterizes intermittently; no external bag needed |
| Catheterizable stoma | Used in urologic surgery (e.g., Mitrofanoff appendicovesicostomy); continent, catheterized |
V. Stoma Site Selection
The diagram below shows stoma site marking relative to the umbilicus and iliac crest:
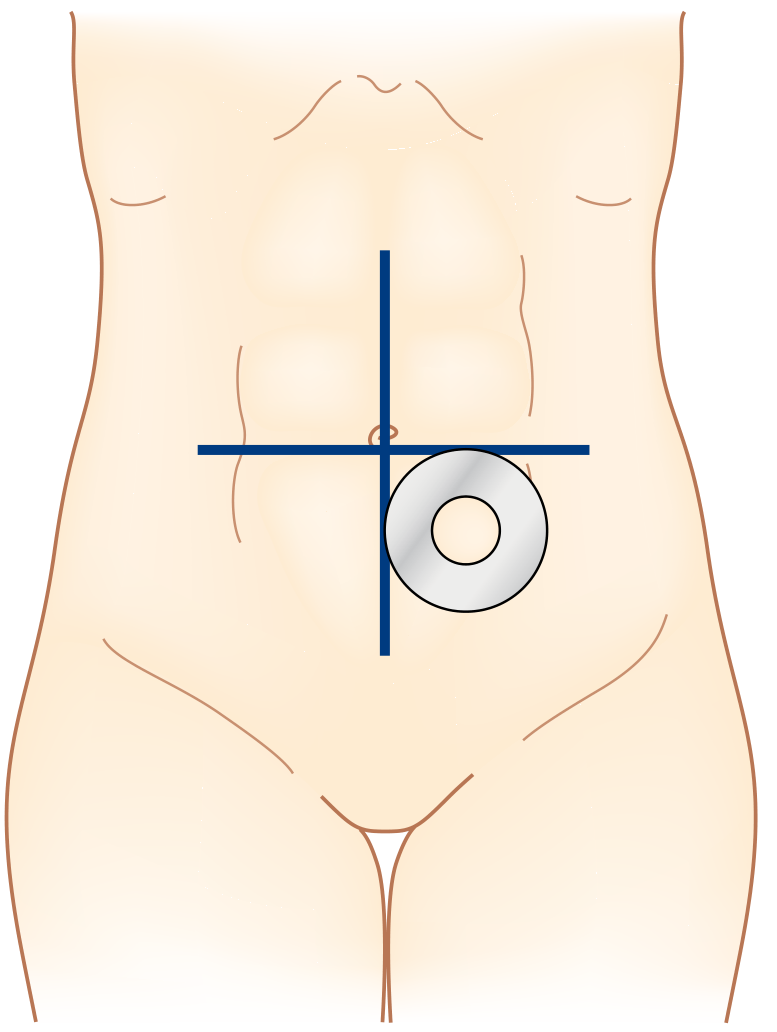
Principles of site selection:
- Mark preoperatively (ideally with stomal therapy nurse)
- Within the rectus abdominis muscle (reduces parastomal hernia risk)
- Away from bony prominences, belt line, skin creases, previous scars, and umbilicus
- Visible to the patient (infraumbilical fat mound is ideal in most patients)
- Aperture should admit two fingers comfortably
VI. Stoma Selection During Surgery — Decision Guide
| Clinical Scenario | Preferred Stoma |
|---|---|
| Temporary diversion after low anterior resection | Loop ileostomy (preferred) |
| Emergency perforation/peritonitis with resection | End colostomy + Hartmann's or double-barrel |
| Permanent colostomy after APR for rectal cancer | End sigmoid colostomy |
| Permanent ileostomy (panproctocolectomy for UC/FAP) | End ileostomy (Brooke) |
| Obese patient — limited colon mobility | End-loop colostomy |
| Anastomotic leak risk very high | Double-barrel or end stoma |
| Complex intra-abdominal sepsis | Double-barrel (complete diversion) |
| Continent diversion (selected patients) | Kock pouch or catheterizable stoma |
"Loop ileostomies are often chosen for temporary diversion because of their lack of odor, ease of care, and ease of closing. Transverse loop colostomies should seldom be used because they are large and are very prone to prolapse, and it can be difficult to maintain pouch adherence." — Sabiston Textbook of Surgery, p. 2072
VII. Key Differences at a Glance
| Feature | Ileostomy | Colostomy |
|---|---|---|
| Bowel segment | Ileum | Colon |
| Effluent | Liquid/semi-liquid | Semi-formed to formed |
| Skin risk | High (digestive enzymes) | Lower |
| Output volume | High (800–1200 mL/day) | Lower |
| Stoma maturation | Spouted (Brooke) | Flush |
| Typical side | Right iliac fossa | Left iliac fossa |
| Common use | Temporary diversion | Permanent diversion |
| Feature | End Stoma | Loop Stoma | Double-Barrel |
|---|---|---|---|
| Lumens visible | 1 | 2 (joined) | 2 (separate) |
| Posterior wall | — | Intact | Absent |
| Reversibility | Harder | Easier | Intermediate |
| Diversion | Complete (proximal) | Near-complete | Complete |
| Use case | Permanent / emergency | Temporary diversion | Emergency / complex |
| Prolapse risk | Lower | Higher (esp. transverse) | Lower |
Sources: Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice; Sleisenger and Fordtran's Gastrointestinal and Liver Disease.
This is a shared conversation. Sign in to Orris to start your own chat.