TB urogenital
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Urogenital Tuberculosis (UG-TB)
Epidemiology
UG-TB is diagnosed in 1.1–1.5% of all TB cases and 5–6% of extrapulmonary TB cases. Men are infected twice as often as women. Most patients are 20–40 years of age. The average latent period from initial pulmonary infection to clinical UG-TB is 22 years (range 1–46 years). — Brenner and Rector's The Kidney
Organs affected:
- Kidneys: 60–100%
- Ureters: 19–41%
- Bladder: 15–20%
- Prostate/epididymis: 20–50% of men
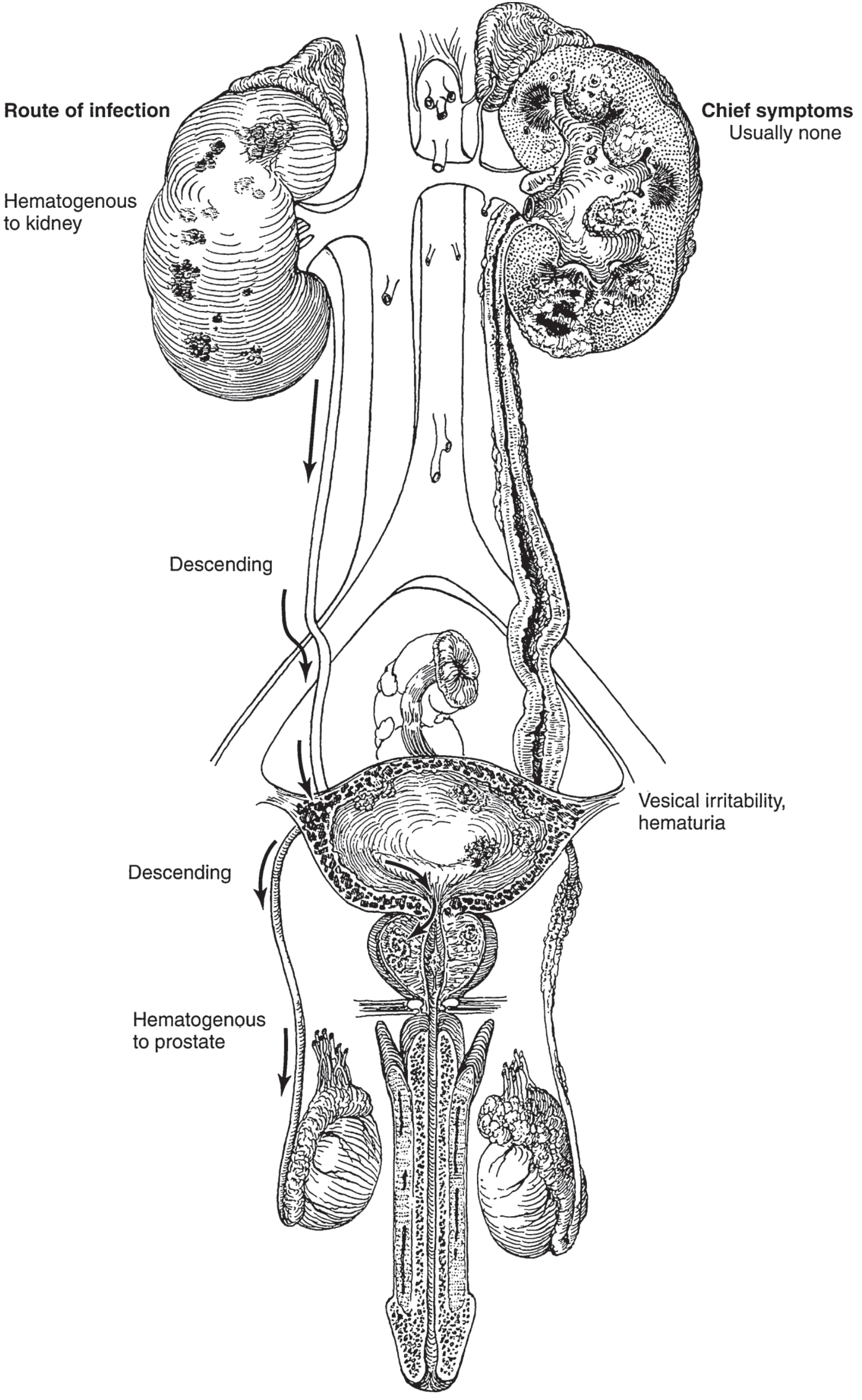
Pathogenesis
Primary TB (usually pulmonary) → haematogenous dissemination → seeding of the renal cortex (favoured by high oxygen tension) → latent foci → reactivation years later (characteristically unilateral).
From the kidney, infection descends contiguously through urine to the collecting system → ureter → bladder → prostatic urethra → prostate/seminal vesicles → epididymis. The prostate can also be seeded directly haematogenously.
Pathology by Site
Kidney & Ureter
The initial cortical granulomas caseate and liquefy → cavitation. Pus discharges into the calyx → calyceal erosion → papillary necrosis → progressive destruction. The kidney surface may appear grossly normal early, but on section shows cheesy caseation. The ureter becomes fibrosed and shortened, producing a "golf-hole" (gaping) ureteral orifice — a sign of an incompetent vesicoureteric junction.
In advanced disease the entire kidney is replaced by caseous material. Calcium deposition during repair causes autonephrectomy (a fibrosed, functionless kidney with or without calcification). This occurs in 23–33% of cases; 27% of patients worldwide present with a non-functioning unilateral kidney. — Brenner and Rector's The Kidney
Microscopy: the classic triad — caseating necrosis + epithelioid histiocytes + Langhans giant cells.
Bladder
Infected urine bathes the mucosa → tubercles form (especially near the involved ureteral orifice) → coalescence → ulceration (may bleed) → fibrosis → "thimble bladder" (small-capacity contracted bladder) → marked urinary frequency. Ureteral reflux or stenosis may cause hydronephrosis. — Smith and Tanagho's General Urology
Prostate & Seminal Vesicles
Infected urine traversing the prostatic urethra seeds the prostate. Tuberculous granulomatous prostatitis can elevate PSA and mimic prostate carcinoma clinically.
Epididymis & Testis
Extension along the vas or perivasal lymphatics from the prostate. Usually painless (chronic indolent course). Extensive abscess may rupture through the scrotal skin creating a permanent sinus.
Clinical Features
Up to 50% of patients have no localising genitourinary symptoms. Presentations include:
| Category | Features |
|---|---|
| Asymptomatic | Incidental finding; "sterile pyuria" |
| Urinary | Dysuria, frequency, haematuria, flank pain |
| Systemic | Fever, weight loss, night sweats (25–33%) |
| Male genital | Hard non-tender epididymis, beaded vas deferens, nodular prostate, nontender testicular mass |
| Female genital | Infertility, pelvic pain |
The classic clue: "sterile (acid) pyuria" — pyuria with negative routine bacterial cultures, acidic pH urine. UG-TB should be suspected when conventional antibiotics fail for apparent UTI. — Comprehensive Clinical Nephrology
Diagnosis
Urine Examination
- Urinalysis: abnormal in >90%; most common finding is sterile pyuria + haematuria
- At least 3 (preferably 5) consecutive early-morning urine cultures for M. tuberculosis — sensitivity 65%, specificity 100%; takes 6–12 weeks (conventional) or ~2 weeks (MGIT liquid culture — WHO gold standard)
Molecular Tests
- GeneXpert MTB/RIF (PCR): sensitivity ~95%, specificity ~90%; simultaneously detects rifampicin resistance; can be used on urine. Note: may give false positives post-treatment due to residual DNA.
- Xpert XDR: also detects resistance to isoniazid, injectable agents, fluoroquinolones
Immunological
- IGRA (QuantiFERON TB Gold / T-SPOT): sensitivity and specificity >90%; not affected by prior BCG vaccination; identifies latent or active disease — preferred over TST
- TST/Mantoux: positive in 60–90% of cases; affected by BCG vaccination; now rarely used
Histopathology
- Pathologic triad: caseating necrosis + epithelioid histiocytes + Langhans giant cells
- Ultrasound-guided FNA/biopsy of renal lesion useful
- Endoscopy (cystourethroscopy, ureteroscopy, hysteroscopy, laparoscopy) for anatomic assessment and biopsy
Imaging
CT is now preferred over IVP. Characteristic findings (roughly in progression):
- Calyceal erosions (earliest)
- Papillary necrosis
- Renal parenchymal cavitation, dilated calyces, hydronephrosis
- Ureteral wall thickening + strictures (most common in distal third)
- Bladder wall thickening, reduced volume, filling defects
- Calcification patterns (curvilinear, amorphous/speckled, ureteric)
- Autonephrectomy (densely calcified, non-functioning kidney)
Management
Medical (First-Line Anti-TB Therapy)
The standard regimen follows general TB treatment principles:
- 2 months HRZE (isoniazid + rifampicin + pyrazinamide + ethambutol) induction
- 4 months HR (isoniazid + rifampicin) continuation = 6 months total for drug-sensitive disease
Corticosteroids are used adjunctively for ureteric strictures and bladder involvement to reduce fibrosis.
Surgical
Indications include: obstructive complications (ureteral stricture, hydronephrosis), non-functioning kidney, contracted bladder, or diagnostic uncertainty. Procedures include:
- Nephrectomy/nephroureterectomy for autonephrectomy or severely damaged kidney
- Ureteral reconstruction / reimplantation for strictures
- Augmentation cystoplasty for contracted (thimble) bladder
- JJ stenting or nephrostomy for acute obstruction
Surgery is almost always performed after or alongside anti-TB chemotherapy, not instead of it. — Comprehensive Clinical Nephrology
Key Complications
- Autonephrectomy (23–33%)
- Renal failure (1–10%)
- Ureteral stricture → hydronephrosis
- Thimble bladder (severe frequency/urgency)
- Male infertility (epididymal/vasal damage)
- Female infertility (fallopian tube involvement)
Sources: Comprehensive Clinical Nephrology, 7th Edition | Brenner and Rector's The Kidney | Smith and Tanagho's General Urology, 19th Edition
This is a shared conversation. Sign in to Orris to start your own chat.