Thyroid gland anatomy with embryology and blood supply and nerve supply?
Reading File
Finding Sources
Finding Sources
Searching Images
thyroid gland anatomy blood supply nerve supply
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Thyroid Gland — Anatomy, Embryology, Blood Supply & Nerve Supply
Embryology
The thyroid is the first endocrine gland to develop. It arises as a midline outpouching of the primitive foregut at around the 3rd week of gestation, originating from the foramen cecum at the base of the tongue.
- The medial thyroid anlage (endodermal thickening of the pharyngeal floor) descends in the midline, anterior to the hyoid bone and larynx.
- During descent it remains connected to the foramen cecum via the thyroglossal duct (an epithelial-lined tube), which normally obliterates by the 8th week of gestation.
- The paired lateral anlages originate from the 4th branchial pouch (ultimobranchial bodies), which are neuroectodermal in origin. These fuse with the median anlage at approximately the 5th week and contribute the parafollicular C cells (calcitonin-secreting), which come to lie in the superoposterior region of each lobe.
- Thyroid follicles are apparent by 8 weeks; colloid formation begins by 11 weeks.
Developmental Anomalies
| Anomaly | Cause |
|---|---|
| Thyroglossal duct cyst | Failure of duct to obliterate; 80% near hyoid bone; moves up with tongue protrusion |
| Lingual thyroid | Failure of median anlage to descend; may be only thyroid tissue present |
| Ectopic thyroid | Found anywhere from tongue base to mediastinum, pericardium, even interventricular septum |
Treatment of thyroglossal duct cysts is the Sistrunk operation — en bloc cystectomy + central hyoid bone resection.
Gross Anatomy
- Weight: ~20 g (varies with body weight and iodine intake)
- Consists of two lobes connected by an isthmus just inferior to the cricoid cartilage
- A pyramidal lobe is present in ~50% of individuals, projecting superiorly from the isthmus (remnant of the thyroglossal duct)
- The lobes extend superiorly to the mid-thyroid cartilage and lie adjacent to the carotid sheaths and sternocleidomastoid muscles laterally
- Strap muscles (sternohyoid, sternothyroid, omohyoid) overlie the gland anteriorly
- Posterolaterally, the gland is in contact with the tracheoesophageal groove where the recurrent laryngeal nerve runs
- Each lobe has a posterior projection called the tubercle of Zuckerkandl at the level of the cricoid cartilage — a key surgical landmark for identifying the RLN
The gland is invested in a fibrous capsule with septa extending into the parenchyma, dividing it into lobules containing follicles.
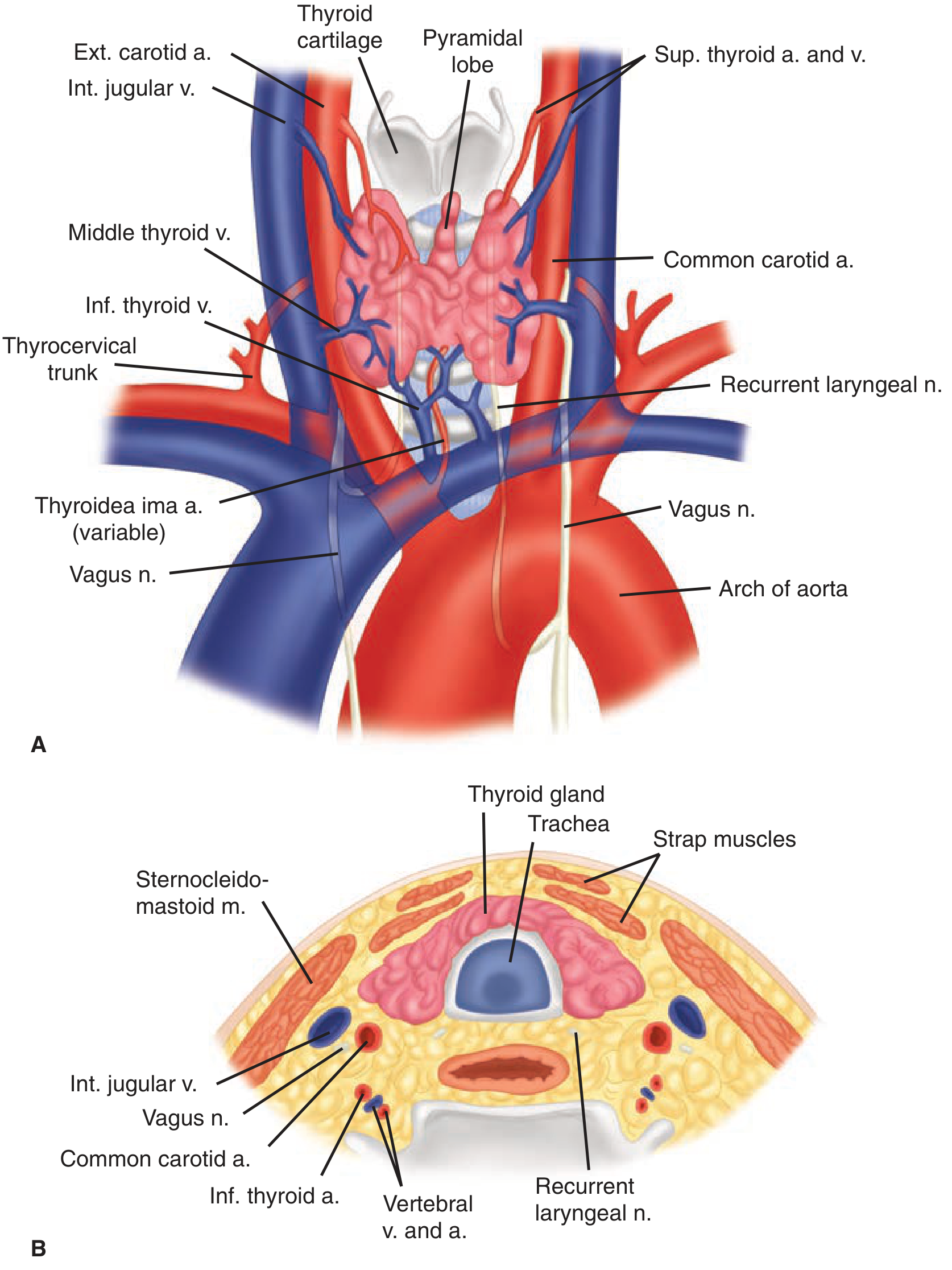
Blood Supply
Arterial Supply
| Artery | Origin | Entry |
|---|---|---|
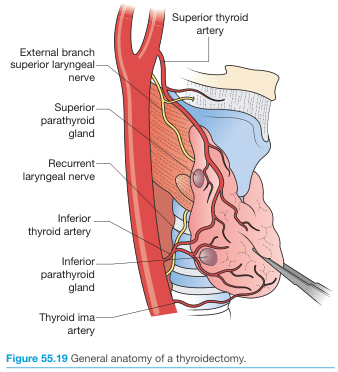
| Superior thyroid artery | External carotid artery (ipsilateral) | Divides into anterior & posterior branches at apex of each lobe |
| Inferior thyroid artery | Thyrocervical trunk (from subclavian artery) | Ascends posterior to carotid sheath; enters lobe at its midpoint |
| Thyroidea ima artery (variant) | Directly from aorta or innominate artery | Enters isthmus; present in 1–4% of individuals; may replace a missing inferior thyroid artery |
The inferior thyroid artery crosses the recurrent laryngeal nerve — the RLN must be identified before any arterial branches are ligated during surgery.
Venous Drainage
Three sets of veins drain the gland:
- Superior thyroid veins — run with the superior thyroid arteries → drain into internal jugular veins
- Middle thyroid veins — least consistent; drain into internal jugular veins
- Inferior thyroid veins — often form a plexus → drain into brachiocephalic veins
Lymphatic Drainage
Extensive intraglandular lymphatic network connecting both lobes through the isthmus. Regional nodes include:
- Pretracheal, paratracheal, perithyroidal
- RLN chain nodes
- Superior mediastinal nodes
- Retropharyngeal and lateral cervical (deep jugular) nodes
Lymph nodes are organized into levels I–VII (upper mediastinal = level VII).
Nerve Supply
1. Recurrent Laryngeal Nerves (RLN)
- Branch of the vagus nerve (CN X)
- Left RLN: arises where the vagus crosses the aortic arch, loops around the ligamentum arteriosum, ascends medially in the tracheoesophageal groove
- Right RLN: arises where the vagus crosses the right subclavian artery, loops posterior to it, then ascends more obliquely than the left
- Both RLNs may branch in the neck and can pass anterior, posterior, or interdigitate with branches of the inferior thyroid artery
Function: Innervates all intrinsic laryngeal muscles except cricothyroid
Injury consequences:
- Unilateral injury → ipsilateral vocal cord paralysis (paramedian = weak voice; abducted = hoarse voice + ineffective cough)
- Bilateral injury → airway obstruction (may need emergency tracheostomy) or loss of voice
Non-recurrent RLN occurs in 0.5–1% on the right (associated with aberrant right subclavian artery). Extremely rare on the left (seen with situs inversus + right aortic arch). Important surgical pitfall.
The ligament of Berry is a critical zone: the last segment of the RLN courses below the tubercle of Zuckerkandl and is closely applied to this ligament. Nerve branches may traverse the ligament in 25% of individuals.
2. Superior Laryngeal Nerves (SLN)
Also from the vagus nerve; divides at the level of the hyoid into:
| Branch | Type | Function |
|---|---|---|
| Internal branch | Sensory | Supraglottic larynx |
| External branch | Motor | Cricothyroid muscle |
- The external branch of the SLN (EBSLN) descends on the inferior pharyngeal constrictor alongside the superior thyroid vessels before innervating the cricothyroid
- Cernea classification describes its relationship to the superior thyroid artery:
- Type 1: nerve crosses artery ≥1 cm above superior thyroid pole (safe zone)
- Type 2a: nerve crosses artery <1 cm above the pole — occurs in ~20% of individuals (at risk)
- Type 2b: nerve crosses below the thyroid pole (highest risk)
- Injury: inability to tense ipsilateral vocal cord → loss of high-pitched voice, voice fatigue, difficulty projecting voice (particularly devastating for singers)
3. Autonomic Innervation
- Sympathetic: from superior and middle cervical sympathetic ganglia → enter gland with blood vessels → vasomotor function
- Parasympathetic: from the vagus nerve via branches of the laryngeal nerves
Summary Diagram
Sources: Schwartz's Principles of Surgery 11th Ed., pp. 1653–1658 | Bailey & Love's Short Practice of Surgery 28th Ed., p. 885 | Guyton & Hall Medical Physiology, p. 930
Normal respiratory rate
Finding Sources
Reading File
Reading File
Normal Respiratory Rate
| Age Group | Normal Range |
|---|---|
| Adults | 12–20 breaths/min |
| Neonates (0–1 month) | 30–60 breaths/min |
| Infants/Children | Higher than adults, decreasing toward adult values with age |
Key Points
Adults
- Normal tidal volume is ~500 mL; at 12 breaths/min this gives a minute ventilation of ~6 L/min — Guyton & Hall Medical Physiology
- The acceptable range is 10–20 breaths/min in adults with normal respiratory physiology — Tintinalli's Emergency Medicine
Neonates
- Normal is 30–60 breaths/min; count for a full minute with the infant resting or asleep
- Neonates increase minute ventilation almost entirely by increasing rate (not tidal volume)
- A resting rate >60 breaths/min during quiet breathing requires evaluation for tachypnea
Terminology
- Tachypnea: >20 breaths/min in adults; >60/min in neonates
- Bradypnea: <12 breaths/min in adults
- Apnea: cessation of breathing; in neonates, pauses >20 seconds (or with bradycardia/cyanosis) are abnormal
This is a shared conversation. Sign in to Orris to start your own chat.