Carcinoma Brest
Reading File
Finding Sources
Searching PubMed
"breast cancer"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from multiple textbooks. Let me compile the full answer.
Carcinoma of the Breast
Epidemiology
Breast cancer is the most common malignancy in females globally. In 2020, it surpassed lung cancer as the most common cancer worldwide, with an estimated 2.3 million new cases accounting for ~12% of all new cancer diagnoses. In the United States, the lifetime risk is 1 in 8 females. The majority (75%) are diagnosed after age 50. Incidence is highest in North America, Northern/Western Europe, and Australia/New Zealand. Globally, incidence and mortality are rising in low-resource countries due to social changes in reproductive patterns and limited healthcare access. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Risk Factors
Modifiable Risk Factors
| Risk Factor | Relative Risk (RR) |
|---|---|
| Radiation exposure | RR = 6 |
| Obesity (BMI >30, postmenopausal) | RR = 1.29 |
| HRT use >10 years | RR = 1.2 |
| Heavy alcohol (>4 drinks/day) | RR = 1.46 |
| Moderate alcohol (3-4 drinks/day) | RR = 1.32 |
| Smoking ≥25 cigarettes/day | RR = 1.14 |
| Late first pregnancy (>35 yrs) | Increased risk |
| Nulliparity | Increased risk |
| Absence of breastfeeding | Increased risk |
Non-Modifiable Risk Factors (Relative Risk >4.0)
- Female sex (99% of cases are female)
- Increasing age
- Germline mutations (BRCA1/BRCA2, high penetrance)
- Strong family history (>1 first-degree relative, early onset, multiple cancers)
- Personal history of breast cancer
- High breast density
Protective Factors
-
Early first pregnancy (<20 years)
-
Prolonged breastfeeding (>12 months)
-
Bilateral prophylactic mastectomy (reduces risk ~90%)
-
ER antagonists/chemoprevention (reduces ER-positive cancer incidence)
-
Bailey and Love's Short Practice of Surgery, 28th Ed
Classification
Histological Classification
In Situ Carcinomas:
- DCIS (Ductal Carcinoma In Situ): Precursor to invasive ductal carcinoma; found as microcalcifications on mammography. If untreated, the subsequent invasive cancer is typically in the same breast.
- LCIS (Lobular Carcinoma In Situ): Marker of increased risk; two-thirds of subsequent cancers occur in the same breast, one-third in the contralateral breast.
Invasive Carcinomas (Foote and Stewart Classification):
| Type | Frequency |
|---|---|
| Invasive Ductal Carcinoma - No Special Type (NST/IDC) | ~80% |
| Invasive Lobular Carcinoma | ~10% |
| Medullary Carcinoma | ~4% |
| Mucinous (Colloid) Carcinoma | ~2% |
| Papillary Carcinoma | ~2% |
| Tubular Carcinoma | ~2% |
| Rare (adenoid cystic, squamous cell, apocrine) | <1% |
| Paget's Disease of the Nipple | - |
Special-type notes:
-
Medullary carcinoma: Soft, hemorrhagic; dense lymphoreticular infiltrate; often BRCA1 phenotype; <10% ER-positive; better prognosis than NST.
-
Mucinous carcinoma: Bulky, gelatinous; >90% ER-positive; 5-year survival ~73%.
-
Papillary carcinoma: Presents in 7th decade; ~87% ER-positive; rare LN metastases; favorable prognosis.
-
Tubular carcinoma: Up to 20% of screen-detected cancers; ~94% ER-positive; excellent prognosis.
-
Paget's disease: Eczematous eruption of nipple; Paget cells (large pale vacuolated cells) in epithelial rete pegs; CEA-positive (vs. S-100-positive in melanoma).
-
Schwartz's Principles of Surgery, 11th Ed
Molecular/Clinical Subtypes
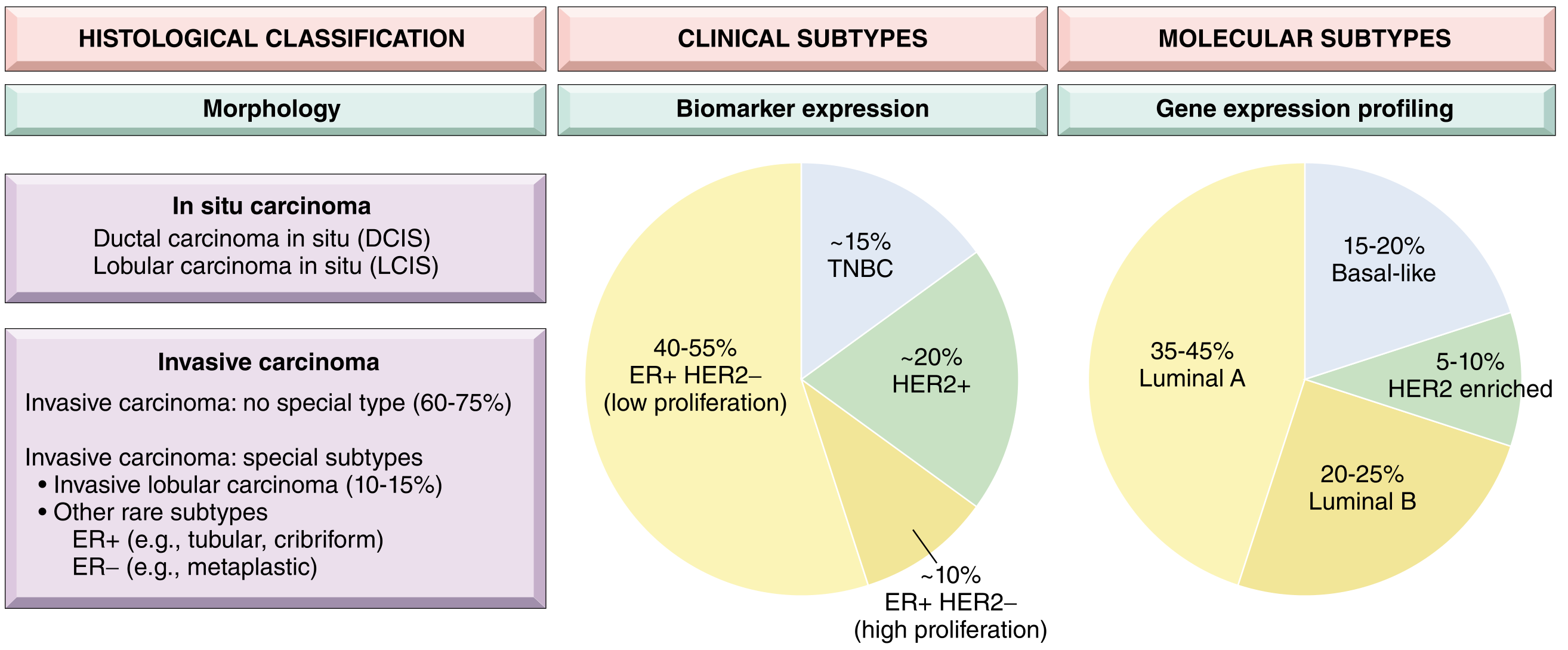
| Molecular Subtype | Hormone Receptor | HER2 | Ki-67 | Frequency |
|---|---|---|---|---|
| Luminal A | ER/PR positive | Negative | Low | 35-45% |
| Luminal B | ER/PR positive | Negative | High | 20-25% |
| HER2 enriched | Negative | Positive | High | 5-10% |
| Basal-like (TNBC) | Negative | Negative | High | 15-20% |
| Claudin-low | Negative | Negative | Variable | Rare |
- ER-positive/HER2-negative tumors = "Luminal" cancers (largest group, ~40-55% of all)
- Triple-negative breast cancer (TNBC) = ER/PR/HER2-negative = worst prognosis, most chemosensitive acutely
- HER2 cancers and TNBC constitute a higher proportion in younger patients and women of African descent
- Bailey and Love's Short Practice of Surgery, 28th Ed; Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis
Breast carcinomas arise via stepwise acquisition of driver mutations. Two main molecular pathways:
Low-grade pathway: Initiated by mutations in genes such as CDH1 (lobular cancers), PIK3CA; precursor lesion is low-grade DCIS/ADH. These cancers are typically ER-positive, luminal A subtype.
High-grade pathway: Major precursor is high-grade DCIS. Genomic changes include loss of 13q, gain of 11q13, amplification of 17q12 (HER2 locus). Expression signature is enriched for proliferating cell genes.
The tumor microenvironment plays an important role: cancer-associated fibroblasts, immune evasion via PD-L1 upregulation, and myoepithelial cell loss all contribute to progression from in situ to invasive disease. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Familial/Genetic Causes
- BRCA1 (17q21): 50-85% lifetime risk of breast cancer; up to 40% risk of ovarian cancer; associated mostly with TNBC.
- BRCA2 (13q12.3): 50-60% lifetime risk; 20% ovarian cancer risk; also associated with prostate, pancreatic, and biliary cancer.
- BRCA1/2 account for 80-90% of single-gene familial breast cancers; ~3-6% of all breast cancers.
- Other high-penetrance genes: TP53 (Li-Fraumeni), PTEN (Cowden), STK11 (Peutz-Jeghers), CDH1.
Clinical Presentation
- Most common: Discrete, painless breast lump - most often in the upper outer quadrant (where 50% of terminal duct-lobular units lie)
- Nipple retraction or discharge (blood/serous)
- Skin changes: peau d'orange (obstruction of cutaneous lymphatic drainage), dimpling/tethering (shortening of Cooper's ligaments), ulceration
- Peau d'orange: sign of locally advanced disease
- Cancer en cuirasse: extensive dermal infiltration of chest wall
- Inflammatory carcinoma: diffuse redness/erythema + skin edema involving >1/3 of the breast; no discrete lump; mimics mastitis but does not respond to antibiotics
Spread and Metastasis
Lymphatic: Mainly to axillary lymph nodes; inner half tumors also drain to internal mammary nodes. The pattern of axillary involvement is used for staging.
Haematogenous: At tumor size of 1-2 mm, neoangiogenesis occurs. Distant metastases occur (in order of frequency) to:
-
Bone: lumbar vertebrae > neck of femur > thoracic vertebrae > ribs > skull (generally osteolytic; rarely osteosclerotic). Bone marrow replacement → leukoerythroblastic anaemia.
-
Liver, lungs, brain; occasionally adrenals and ovaries.
-
Limb deposits occur above the elbow and above the knee (haematopoietic marrow distribution).
-
Bailey and Love's Short Practice of Surgery, 28th Ed
Investigations (Triple Assessment)
- Clinical examination
- Imaging:
- Mammography (calcifications, mass, architectural distortion)
- Ultrasound (solid vs. cystic, LN assessment)
- MRI (extent of disease, multifocal disease, response to NACT)
- Bone scan, CT chest/abdomen/pelvis for staging
- Pathology:
- Core needle biopsy (histology + receptor status: ER, PR, HER2, Ki-67)
- Fine needle aspiration cytology (FNAC) - less common now
- Sentinel lymph node biopsy (SLNB) for axillary staging
TNM Staging (AJCC 8th Edition - Summary)
| Stage | Description |
|---|---|
| 0 | DCIS/LCIS only |
| I | T ≤2 cm, N0 |
| IIA | T ≤5 cm, N1 or T 2-5 cm, N0 |
| IIB | T >5 cm, N0 or T 2-5 cm, N1 |
| IIIA | Any T, N2; or T >5 cm, N1-2 |
| IIIB | T4 (skin/chest wall involvement) any N; Inflammatory carcinoma |
| IIIC | Any T, N3 |
| IV | Distant metastases (M1) |
Management
Neoadjuvant Chemotherapy (NACT)
Given for locally advanced disease (stage III) to downstage tumor before surgery. After 2 cycles, if stable/progressive disease → proceed to surgery + second-line chemo. Pathological Complete Response (pCR) is a favorable prognostic marker.
Surgery
Early Breast Cancer (Stages 0, I, II):
- Breast-Conserving Surgery (BCS/lumpectomy/wide local excision): Preferred when feasible; requires negative margins (no tumor on inked margins for invasive cancer; ≥2 mm for DCIS). Followed by radiotherapy.
- Mastectomy: Indicated for large tumors (relative to breast size), multicentric disease, diffuse microcalcification (DCIS), BRCA-positive cancers, local recurrence after BCS, or patient preference. Skin-sparing/nipple-sparing mastectomy possible when tumor is >1 cm from skin.
- Modified Radical Mastectomy (MRM): Mastectomy + level I/II/III axillary node dissection.
- Radical Mastectomy (Halsted): Rarely indicated now - excessive morbidity, no survival benefit.
Axillary Surgery:
- SLNB first (if clinically node-negative); full axillary dissection if SLNB positive.
Breast Reconstruction: Latissimus dorsi flap, TRAM flap, DIEP flap, silicone implant.
Radiotherapy
Indicated:
- After all BCS
- After mastectomy if: tumor ≥5 cm, skin/chest wall involvement, lymphovascular invasion (grade 3), or axillary LN-positive
- Dose: 45-50.4 Gy in 25 fractions OR 40-42.5 Gy in 15-16 fractions (hypofractionation)
Adjuvant Systemic Therapy
| Subtype | Treatment |
|---|---|
| ER/PR-positive (premenopausal) | Tamoxifen ± ovarian suppression × 5-10 years |
| ER/PR-positive (postmenopausal) | Aromatase inhibitors (anastrozole, letrozole, exemestane) |
| HER2-positive | Trastuzumab (Herceptin) ± pertuzumab; chemotherapy backbone (e.g., docetaxel + carboplatin) |
| TNBC | Chemotherapy (anthracycline + taxane based); immunotherapy (pembrolizumab for PD-L1+); PARP inhibitors if BRCA-mutated (olaparib/talazoparib) |
| Any high-risk | Adjuvant chemotherapy (AC-T: doxorubicin + cyclophosphamide → paclitaxel; or FEC-D: 5-FU + epirubicin + cyclophosphamide → docetaxel) |
- EBCCTCG Oxford meta-analyses: chemotherapy improves relapse-free survival by ~30% and overall survival by ~10%.
- Bailey and Love's Short Practice of Surgery, 28th Ed
Metastatic (Stage IV) Breast Cancer
Goals are palliative - control of disease, quality of life, symptom management.
- Bone metastases: bisphosphonates (zoledronic acid) or denosumab; radiotherapy for pain
- Visceral metastases: systemic therapy guided by receptor status
- Pleural effusion: drainage + pleurodesis
- Solitary metastasis in good performance status: consider surgical resection
Hereditary Breast Cancer
| Gene | Chromosome | Breast Cancer Risk | Other Cancers |
|---|---|---|---|
| BRCA1 | 17q21 | 50-85% lifetime | Ovarian (40%), fallopian tube |
| BRCA2 | 13q12.3 | 50-60% lifetime | Ovarian (20%), prostate, pancreatic, biliary |
| TP53 | 17p13 | High (Li-Fraumeni) | Sarcoma, brain, adrenal |
| PTEN | 10q23 | Elevated (Cowden) | Thyroid, endometrium |
Management for BRCA carriers:
- Bilateral risk-reducing mastectomy (↓ risk 90%)
- Chemoprophylaxis with tamoxifen/anastrozole (↓ risk ~50%)
- Bilateral salpingo-oophorectomy after family completion (~35-40 years)
- Bailey and Love's Short Practice of Surgery, 28th Ed
Prognosis
The most important prognostic factors are:
- Axillary lymph node status (most important)
- Tumor size (T stage)
- Histological grade (Nottingham grading)
- ER/PR/HER2 receptor status (biologic subtype)
- Ki-67 proliferative index
- Lymphovascular invasion
- Overall risk of death from invasive breast cancer is approximately 20% (declining ~1-2% per year with modern therapy)
- Luminal A has the best prognosis; TNBC has the worst short-term prognosis
- Gene expression signatures (Oncotype DX, MammaPrint) help guide chemotherapy decisions in ER-positive, HER2-negative early breast cancer
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease | Robbins & Kumar - Basic Pathology | Bailey and Love's Short Practice of Surgery, 28th Ed | Schwartz's Principles of Surgery, 11th Ed
This is a shared conversation. Sign in to Orris to start your own chat.