Ptosis
Reading File
Finding Sources
Searching PubMed
ptosis eyelid classification management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a full, textbook-grounded overview of ptosis (blepharoptosis):
Ptosis (Blepharoptosis)

Ptosis is an abnormally low position of the upper eyelid. The upper lid normally covers the superior 2 mm of the cornea (margin reflex distance = 3-4 mm). Ptosis is present when the lid descends below this level.
Classification
| Type | Mechanism | Examples |
|---|---|---|
| Neurogenic | Innervational defect | CN III palsy, Horner syndrome |
| Myogenic | Levator myopathy or NMJ failure | Myasthenia gravis, mitochondrial myopathy, oculopharyngeal dystrophy |
| Aponeurotic (Involutional) | Dehiscence/stretching of levator aponeurosis | Age-related, post-surgical, contact lens use |
| Mechanical | Mass effect or scarring | Lid tumor, chalazion, dermatochalasis |
| Congenital | Levator dysgenesis | Isolated, blepharophimosis syndrome, Marcus Gunn |
Neurogenic Ptosis
Examination of the pupil is the key differentiator:
- Horner syndrome: ptosis + miosis + anhidrosis. The affected eye has a smaller pupil. Caused by interruption of the oculosympathetic pathway (affects Müller's muscle). Full eye movements are preserved.
- CN III palsy: ptosis + larger or normal pupil + limitation of adduction, elevation, and depression. A pupil-sparing oculomotor palsy (normal pupil, limited adduction/elevation/depression) is also possible. Rarely, a lesion in the central CN III subnucleus causes bilateral ptosis with normal pupils and eye movements.
Myogenic Ptosis
- Myasthenia gravis: fluctuating ptosis that typically worsens late in the day or with sustained upgaze (fatigability). May be unilateral or bilateral, and can mimic virtually any ocular motility disorder.
- Chronic progressive external ophthalmoplegia (CPEO): symmetric, slowly progressive ptosis + limitation of eye movements from mitochondrial DNA mutations. Diplopia is a late feature because all eye movements are equally reduced. The Kearns-Sayre variant adds retinal pigmentary changes and cardiac conduction abnormalities.
- Oculopharyngeal dystrophy: autosomal dominant, onset in middle age; ptosis + limited eye movements + dysphagia.
- Myotonic dystrophy: autosomal dominant; ptosis, ophthalmoparesis, cataract, pigmentary retinopathy, muscle wasting, myotonia, frontal balding, and cardiac abnormalities.
Aponeurotic / Involutional Ptosis
Acquired dehiscence or stretching of the aponeurotic tendon connecting the levator muscle to the tarsal plate. Most common in older adults from loss of connective tissue elasticity. Also caused by:
- Eyelid swelling (infection, blunt trauma)
- Cataract surgery (mild post-op ptosis is common and usually resolves within a year without intervention)
- Long-term contact lens use
The characteristic feature is a high or absent upper eyelid skin crease with good levator function.
Mechanical Ptosis
Occurs when excess eyelid tissue (dermatochalasis - redundant skin/fat in elderly), tumors, infections, or inflammation physically weigh down the lid.
Congenital Ptosis
Usually from dysgenesis of the levator palpebrae superioris (fibrofatty replacement of muscle). Key features:
- Absent or poorly defined upper eyelid skin crease
- Lid does not descend fully in downgaze (lid lag)
- Variable degree - mild to severe
- May be associated with superior rectus weakness (shared embryological origin)
- Risk of amblyopia (from visual axis obstruction or induced astigmatism)
- Refractive errors are actually more commonly responsible for amblyopia than the ptosis itself
Marcus Gunn jaw-winking syndrome (~5% of congenital ptosis): misdirection of a branch of CN V (mandibular division) to the levator, causing the ptotic lid to retract with pterygoid muscle stimulation (chewing, jaw movement). Usually unilateral.
Blepharophimosis-ptosis-epicanthus inversus syndrome (BPES): bilateral severe ptosis + telecanthus + epicanthus inversus + blepharophimosis. Autosomal dominant (FOXL2 gene).
Pseudoptosis
Conditions mimicking true ptosis:
- Lack of globe support (enophthalmos, phthisis, artificial eye, microphthalmos)
- Contralateral lid retraction (makes one side appear relatively low)
- Ipsilateral hypotropia (lid follows the eye downward; resolves when the hypotropic eye fixates)
- Brow ptosis (confirmed by manually elevating the eyebrow)
Clinical Evaluation
Measurements to obtain in primary gaze:
- Palpebral fissure width (normal ~10-11 mm)
- Margin reflex distance (MRD1): distance from upper lid margin to corneal light reflex (normal = 4 mm; reduced in ptosis)
- Levator function (LF): excursion from maximal downgaze to maximal upgaze, with frontalis muscle neutralized by thumb pressure over the brow
- Good: ≥8 mm
- Fair: 5-7 mm
- Poor: 4 mm or less
- Absent: ~2 mm or less
Note: Ptosis is underestimated if the patient compensates with frontalis muscle overaction (elevated brow). Unilateral ptosis may cause contralateral lid retraction (Hering's law of equal innervation) - cover the normal eye to unmask the true degree.
Old photographs are invaluable for dating the onset and distinguishing congenital from acquired cases.
Treatment
Surgical (definitive)
| Levator Function | Preferred Procedure |
|---|---|
| Good (≥8 mm) | Levator aponeurosis repair/resection (most common for involutional) |
| Fair (5-7 mm) | Levator resection |
| Poor (<4 mm) | Frontalis sling (connects lid to frontalis muscle) |
- Congenital ptosis: surgery during preschool years; earlier in severe cases to prevent amblyopia
- A weak Bell phenomenon (failure of the eye to rotate upward on lid closure) increases the risk of post-operative exposure keratopathy - check before surgery
Medical
- Myasthenia gravis: acetylcholinesterase inhibitors (pyridostigmine), immunosuppression, thymectomy
- Horner syndrome: identify and treat the underlying cause; phenylephrine eye drops can temporarily elevate the lid (pharmacological test and temporary treatment)
- Ptosis props / crutch spectacles: for patients unfit for surgery
Key Distinguishing Features at a Glance
| Feature | CN III Palsy | Horner Syndrome | Myasthenia Gravis |
|---|---|---|---|
| Pupil | Dilated (or spared) | Miotic | Normal |
| Eye movements | Limited (EOM palsy) | Full | Variable/fatigable |
| Variability | Constant | Constant | Fluctuating (worse with fatigue) |
| Laterality | Unilateral | Unilateral | Uni- or bilateral |
| Associated | Diplopia, headache | Anhidrosis, enophthalmos | Anti-AChR antibodies, thymoma |
Sources: Kanski's Clinical Ophthalmology 10e; Harrison's Principles of Internal Medicine 22e (2025); Localization in Clinical Neurology 8e
Horner syndrome
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a thorough answer. Here is the complete guide:
Horner Syndrome (Oculosympathetic Palsy)
Horner syndrome (also called Bernard-Horner syndrome or oculosympathetic palsy) results from interruption of the sympathetic innervation to the eye and face at any point along the three-neuron pathway.
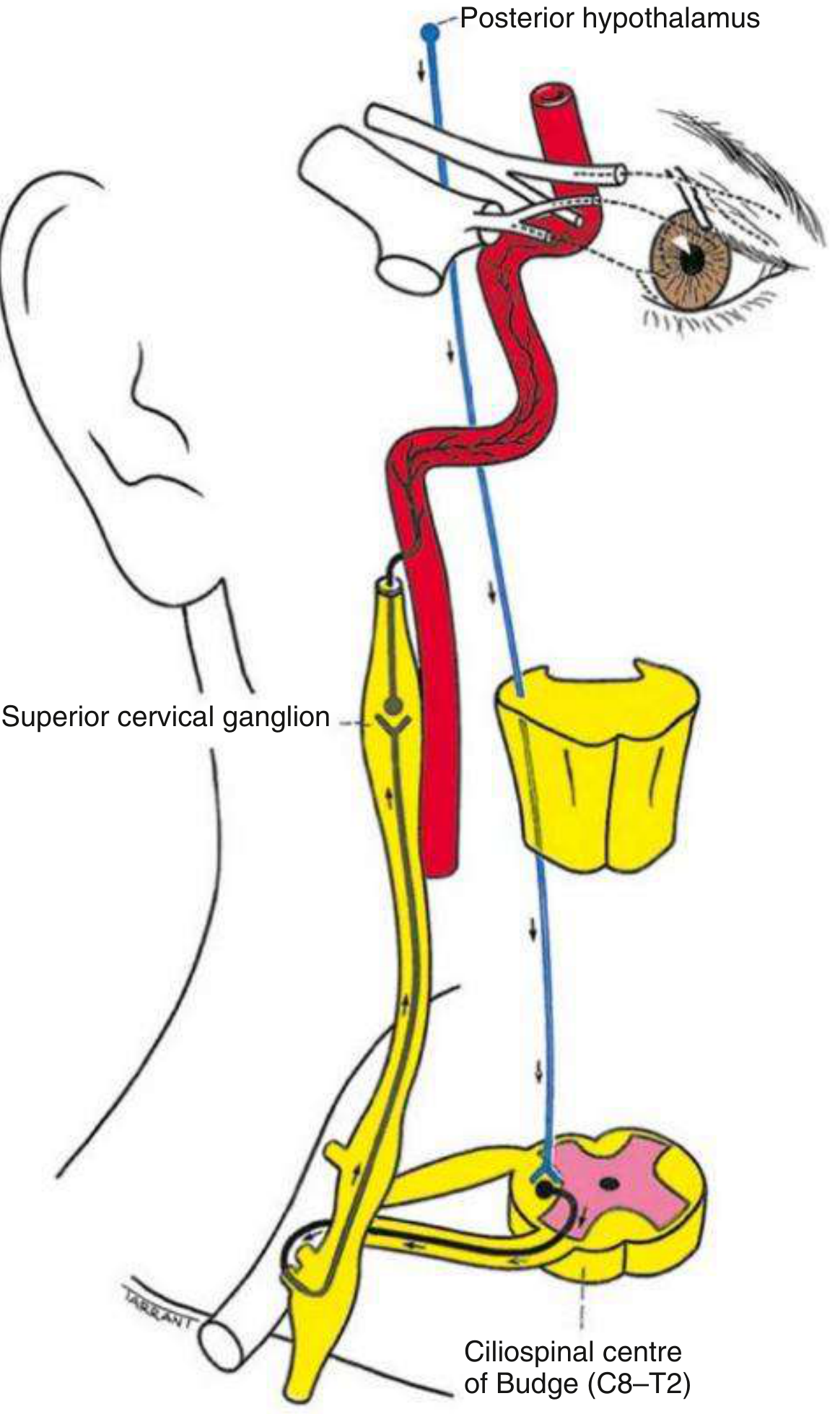
Anatomy of the Three-Neuron Pathway
| Neuron | Course | Key Relations |
|---|---|---|
| 1st order (central) | Posterior hypothalamus → descends uncrossed through brainstem → ciliospinal centre of Budge (C8-T2 intermediolateral horn) | Brainstem, cervical cord |
| 2nd order (preganglionic) | Ciliospinal centre → superior cervical ganglion (neck) | Closely related to apical pleura; vulnerable to Pancoast tumour and neck surgery |
| 3rd order (postganglionic) | Superior cervical ganglion → ascends along internal carotid artery → cavernous sinus → joins CN V1 → via nasociliary and long ciliary nerves to dilator pupillae and Müller's muscle | Internal carotid artery, cavernous sinus |
Classic Signs (the Triad + more)
| Sign | Mechanism |
|---|---|
| Miosis (small pupil) | Loss of sympathetic drive to dilator pupillae; sphincter acts unopposed |
| Ptosis (1-2 mm, upper lid) | Paralysis of Müller's smooth muscle in upper lid |
| Anhidrosis (ipsilateral face) | Loss of sudomotor fibres - only present if lesion is below the superior cervical ganglion (sudomotor fibres travel along the external carotid artery) |
| Inferior lid elevation ("upside-down ptosis" / reverse ptosis) | Weakness of the lower lid retractor (smooth muscle equivalent in lower lid) |
| Apparent enophthalmos | Optical illusion from narrowed palpebral fissure, not true globe retraction |
| Dilation lag | Horner pupil redilates slowly when light is removed - the most sensitive early sign |
| Heterochromia iridis | Affected iris is lighter - seen in congenital or longstanding cases (sympathetics needed for iris pigmentation) |
Key exam finding: anisocoria is more pronounced in the dark (the Horner pupil fails to dilate), in contrast to a CN III palsy where anisocoria is worse in light. Pupillary light and near reflexes remain normal in Horner syndrome.
Causes by Neuron Order
1st Order (Central)
- Brainstem stroke - lateral medullary (Wallenberg) syndrome is the classic cause
- Brainstem tumour or demyelination (MS)
- Syringomyelia / syringobulbia
- Cervical spinal cord lesion
- Diabetic autonomic neuropathy
2nd Order (Preganglionic)
- Pancoast tumour (apical lung carcinoma) - associated with T1 root involvement (weak hand intrinsics)
- Carotid or aortic aneurysm/dissection
- Thoracic spinal cord lesion
- Neck lesions: thyroid tumour, enlarged lymph nodes, trauma, post-surgical
3rd Order (Postganglionic)
- Internal carotid artery dissection - painful acute Horner syndrome; urgent vascular imaging required
- Cavernous sinus mass (thrombosis, aneurysm, tumour)
- Nasopharyngeal tumour
- Otitis media
- Cluster headache (migrainous neuralgia) - transient Horner during attacks
Clinical pearl: Acute onset of painful Horner syndrome - especially with neck or facial pain - should immediately raise concern for carotid artery dissection and be treated as an emergency.
Pharmacological Testing
Step 1: Confirm the Diagnosis
Apraclonidine 0.5-1.0% (preferred, widely available)
- Instill one drop in both eyes; check pupils at 30-45 min
- Result: Horner pupil dilates (and ptosis improves); normal pupil unaffected
- Mechanism: Alpha-1 receptors are upregulated (denervation supersensitivity) on the dilator pupillae in Horner syndrome, so apraclonidine (weak alpha-1 agonist) dilates it; the normal pupil has no such supersensitivity
- Sensitivity ~90%, specificity ~100%
- Caution: Do not use in infants (crosses blood-brain barrier). Has a ~7-day latent period before becoming positive in new lesions
Cocaine 4% (less commonly used now, reserved for equivocal cases)
- Result: Normal pupil dilates; Horner pupil does not
- Mechanism: Cocaine blocks noradrenaline reuptake at postganglionic terminals, causing dilation of a healthy pupil. In Horner syndrome, no noradrenaline is being secreted, so cocaine has no effect
Step 2: Localise Pre- vs Postganglionic
Hydroxyamphetamine 1% (most sensitive)
- Normal or preganglionic Horner: pupil dilates (functioning 3rd-order nerve releases NE)
- Postganglionic Horner: pupil does NOT dilate (3rd-order neurone is dysfunctional, no NE to release)
Phenylephrine 1% (more widely available, comparable)
- Postganglionic Horner (established >10 days): pupil dilates and ptosis may improve (denervation hypersensitivity)
- Central/preganglionic and normal pupil: minimal or no dilation
Note: Do not perform sequential pharmacological tests within 3-5 days of each other (extended drug action)
Investigation
- Confirmed Horner syndrome → specialist neurological or neuro-ophthalmological referral
- Acute presentation = emergency - urgent imaging required
- Gold standard imaging: CT or MR angiography from aortic arch to circle of Willis (covers neck, carotid arteries, apical lung, thyroid, skull base)
- MRI with contrast if brainstem stroke suspected
- If features have been present >1 year with no other localizing signs, diagnostic yield from further investigation is very low
- Plain X-rays and carotid ultrasound have limited utility
Sweat Pattern for Localization
| Lesion Level | Anhidrosis Pattern |
|---|---|
| At/above common carotid artery | Entire ipsilateral face |
| Distal to carotid bifurcation | Absent, or confined to medial forehead and side of nose |
| Postganglionic (internal carotid) | Usually absent - sudomotor fibres travel with external carotid |
Bilateral Horner Syndrome
Rare. Causes include:
- Autonomic neuropathies
- High cervical cord transection
- Bilateral miosis may be subtle - pupillometry or observation of pronounced dilation lag when light is withdrawn helps detect it
Treatment
- Address the underlying cause
- The ptosis of Horner syndrome is mild; surgical correction can be considered at the patient's request
- Apraclonidine eye drops can be used as a temporizing measure to improve ptosis
Quick Comparison: Horner vs CN III Palsy vs Adie Pupil
| Feature | Horner Syndrome | CN III Palsy | Adie Pupil |
|---|---|---|---|
| Pupil size | Small (miosis) | Large (mydriasis) | Large (initially) |
| Ptosis | Mild (1-2 mm) | Severe (complete) | None |
| Light reflex | Normal | Absent | Absent/sluggish |
| Eye movements | Full | Limited (EOM palsy) | Full |
| Anisocoria worse in | Dark | Light | Light |
| Pain | If carotid dissection | If posterior communicating artery aneurysm | None |
Sources: Kanski's Clinical Ophthalmology 10e; Adams and Victor's Principles of Neurology 12e; Neuroanatomy through Clinical Cases 3e; Harrison's Principles of Internal Medicine 22e (2025)
This is a shared conversation. Sign in to Orris to start your own chat.