Mechanism of gene transfer in bacteria
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough breakdown of all mechanisms of gene transfer in bacteria, drawn from Murray's Medical Microbiology 9e and Jawetz, Melnick & Adelberg's Medical Microbiology 28e.
Mechanisms of Gene Transfer in Bacteria
Bacteria exchange genetic material through horizontal gene transfer (HGT), which is fundamentally different from vertical (parent-to-offspring) inheritance. HGT drives evolution, antibiotic resistance spread, and acquisition of virulence factors. There are three major inter-cellular mechanisms plus transposition (intra/inter-cellular).
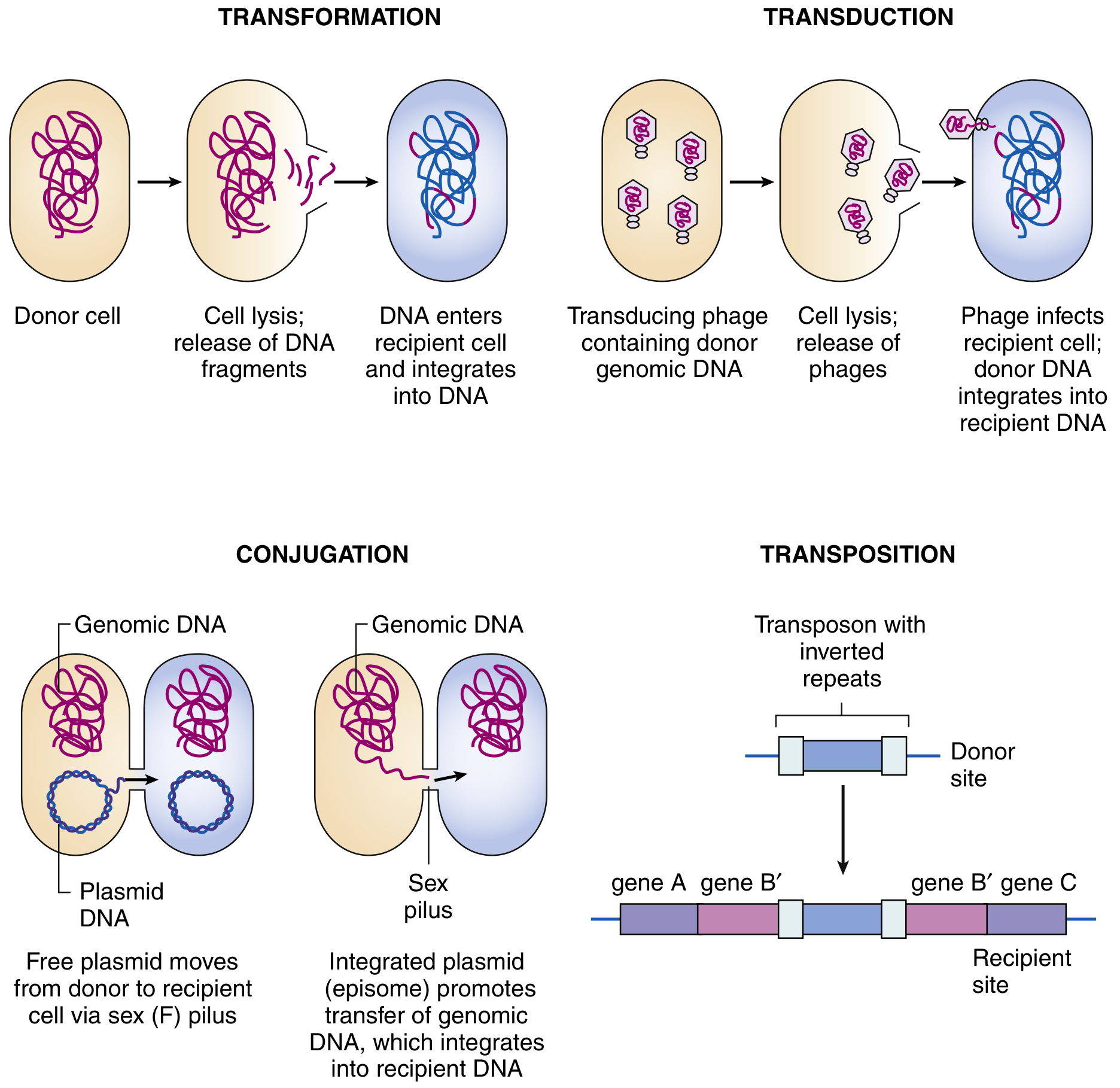
1. Transformation
Definition: The uptake and incorporation of naked (free) exogenous DNA from the environment into a recipient bacterial cell.
Historical note: First discovered by Griffith (1928) in Streptococcus pneumoniae. Avery, MacLeod, and McCarty later identified DNA as the "transforming principle" (1944).
Steps:
- A donor bacterium lyses and releases DNA fragments into the environment.
- A competent recipient cell actively binds, takes up, and incorporates that DNA.
- The foreign DNA recombines with the homologous region of the recipient chromosome.
Competence: Only certain species are naturally competent - they produce specific DNA-binding and uptake proteins and recognize species-specific uptake sequences on the DNA. Naturally competent bacteria of medical importance include:
- Haemophilus influenzae
- Streptococcus pneumoniae
- Neisseria gonorrhoeae and N. meningitidis
- Bacillus spp.
Most other bacteria (e.g., E. coli) require artificial competence - induced by chemical treatment (CaCl2) or electroporation (high-voltage pulses) - a standard laboratory technique.
Significance: A major force in microbial evolution. Natural transformation contributes substantially to horizontal spread of antibiotic resistance across species boundaries, especially in biofilms and the gut flora.
2. Conjugation
Definition: Direct, contact-dependent transfer of DNA from a donor ("male") to a recipient ("female") cell via a sex pilus (type IV secretion system).
Key molecular players:
- The F (fertility) plasmid of E. coli is the prototype conjugative plasmid. It carries all genes needed for its own transfer, including pilus synthesis and initiation of DNA synthesis at the oriT (transfer origin).
- Cells carrying the F plasmid are F+ (donors); cells without it are F- (recipients).
Mechanism:
- The F+ cell extends the sex pilus, which contacts and retracts to bring the cells together.
- A nick is made at oriT and one strand of the F plasmid is transferred to the recipient in a 5' to 3' direction via a rolling-circle mechanism.
- Complementary strands are synthesized in both donor and recipient.
- The recipient becomes F+.
Variants:
| Type | Description |
|---|---|
| F+ × F- | F plasmid transfers; recipient becomes F+ |
| Hfr (High-frequency recombination) | F plasmid integrates into the chromosome; chromosomal DNA is transferred at high frequency but complete transfer is rare (~100 min at 37°C), so recipient usually stays F- |
| F' (F-prime) | F plasmid excises imprecisely, carrying a fragment of chromosomal DNA; transfers that gene copy to the recipient |
Scope: Conjugation occurs in most eubacteria and even between prokaryotes and plant, animal, or fungal cells. It is the most efficient mechanism for spreading resistance plasmids (e.g., R plasmids carrying multiple antibiotic resistance genes).
3. Transduction
Definition: Transfer of bacterial DNA from one cell to another via a bacteriophage (bacterial virus) as the vector.
Mechanism:
- A bacteriophage infects a donor bacterium.
- During packaging of phage DNA, bacterial DNA is accidentally (or specifically) packaged into phage capsids instead.
- This transducing particle infects a new recipient bacterium.
- The injected bacterial DNA recombines with the recipient's chromosome.
Types:
| Type | Phage | Mechanism | Genes transferred |
|---|---|---|---|
| Generalized transduction | Lytic phage (e.g., phage P1) | Random packaging of any bacterial DNA fragment during host chromosome degradation | Any bacterial gene; useful for genetic mapping |
| Specialized (restricted) transduction | Temperate phage (e.g., phage λ) | Imprecise excision of the integrated prophage carries flanking chromosomal genes | Only genes adjacent to the prophage insertion site (e.g., gal and bio genes for phage λ) |
Size limit: Transducing particles carry DNA no more than a few percent of the bacterial chromosome. Only closely linked genes can be co-transduced together.
Clinical importance: Pathogenicity islands are frequently transduced by phages. For example, two phages transport the islands responsible for converting benign Vibrio cholerae into the pathogenic epidemic form - encoding cholera toxin and toxin co-regulated pili.
4. Transposition (Transposons / "Jumping Genes")
Definition: Movement of discrete DNA segments called transposons within or between DNA molecules (chromosome to chromosome, plasmid to chromosome, or plasmid to plasmid) - within a single cell or facilitating transfer across cells when combined with the above mechanisms.
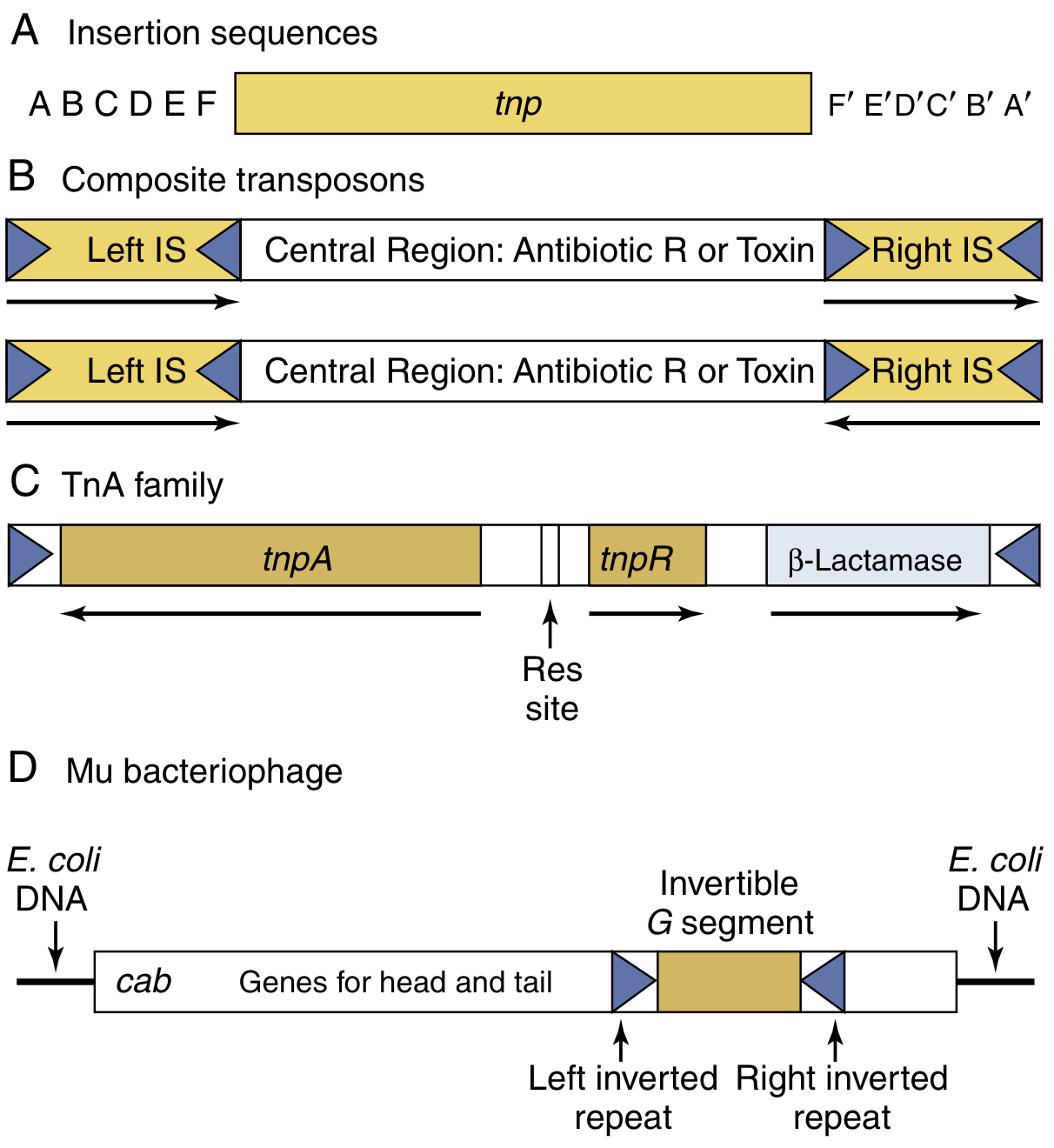
Types of transposons:
| Type | Structure | Features |
|---|---|---|
| Insertion sequences (IS) | 150-1500 bp; inverted repeats flanking a transposase gene | Simplest mobile elements; code only for their own transposase |
| Composite transposons | Central region (resistance/toxin genes) flanked by two IS elements | Carry antibiotic resistance or virulence genes; IS elements allow movement |
| TnA family (e.g., Tn3) | Carries tnpA (transposase), tnpR (resolvase), and a resistance gene (e.g., β-lactamase) | Replicative transposition using a res site |
| Phage-associated | Exemplified by phage Mu | Transposition is coupled to phage replication |
Mechanism: Transposase enzyme recognizes inverted repeats and catalyzes "cut and paste" or replicative insertion into a new target site.
Medical significance: Transposons can inactivate genes by inserting into them. More importantly, they shuttle resistance genes between plasmids and chromosomes, amplifying the spread of multi-drug resistance. The evolution of vancomycin-resistant S. aureus (VRSA) is a direct result of: conjugation of a VRE resistance plasmid into MRSA, followed by transposon jumping of the vancomycin-resistance gene (Tn1546) into the S. aureus multiresistance plasmid.
Summary Comparison
| Feature | Transformation | Conjugation | Transduction | Transposition |
|---|---|---|---|---|
| DNA source | Free/naked environmental DNA | Donor cell (direct contact) | Bacteriophage | Within same cell or between cells |
| Requires cell contact | No | Yes | No | No |
| Vector | None | Sex pilus (F plasmid) | Bacteriophage | Transposase enzyme |
| DNA transferred | Any (if competent) | Plasmid or chromosomal | Limited (~2% chromosome) | Specific mobile element |
| Restriction | Species-specific uptake sequences | Usually same/related species | Limited by phage host range | Sequence-specific insertion |
| Key example | S. pneumoniae virulence transfer | E. coli F plasmid / R plasmids | Phage λ specialized; Phage P1 generalized | Tn1546 in VRSA |
Sources:
- Murray's Medical Microbiology 9e, Ch. 13 (Mechanisms of Genetic Transfer Between Cells)
- Jawetz, Melnick & Adelberg's Medical Microbiology 28e, Ch. 7 (Bacterial Genetics)
Rt pcr uses and advantages over conventional pcr
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough answer. Let me compile it.
RT-PCR and Real-Time PCR: Uses and Advantages Over Conventional PCR
Important clarification on terminology: The abbreviation "RT-PCR" is used in two overlapping ways in the literature:
- RT-PCR = Reverse Transcriptase PCR - detects RNA by converting it to cDNA first
- Real-time PCR (qPCR) = detects/quantifies DNA or RNA during amplification using fluorescence
- Real-time RT-PCR = combines both - converts RNA to cDNA, then quantifies it in real time (e.g., COVID-19 testing)
This answer covers all three in relation to conventional (end-point) PCR.
Conventional (End-Point) PCR - Brief Recap
Conventional PCR amplifies a DNA target through three cyclic steps:
- Denaturation at ~95°C - melts double-stranded DNA into single strands
- Annealing - sequence-specific primers bind their complementary target
- Extension at 72°C - Taq polymerase synthesizes new DNA strands
The product is detected after amplification is complete, typically by gel electrophoresis (agarose gel with ethidium bromide or SYBR staining). Results are qualitative ("band present or absent") with only rough quantification possible.
Part 1: RT-PCR (Reverse Transcriptase PCR)
Principle
Since conventional PCR requires a DNA template, it cannot directly amplify RNA. RT-PCR adds a reverse transcriptase (RT) enzyme step before PCR to convert RNA into complementary DNA (cDNA), which is then amplified normally.
Enzymes used:
- MMLV (Moloney Murine Leukemia Virus) reverse transcriptase
- AMV (Avian Myeloblastosis Virus) reverse transcriptase
- Thermostable enzymes with dual RT + DNA polymerase activity (e.g., Thermus spp. derivatives)
One-Step vs. Two-Step RT-PCR
| Feature | One-Step | Two-Step |
|---|---|---|
| Enzymes | Both RT and Taq in one tube | Separate RT reaction, then PCR |
| Priming | PCR primers used for both steps | Random hexamers or oligo-dT for RT; specific primers for PCR |
| Convenience | Higher | Lower |
| Flexibility | Limited (one target per RT) | Multiple targets from single RT reaction |
| Use case | Routine clinical diagnostics | Research, multiple target detection |
Uses of RT-PCR
| Application | Examples |
|---|---|
| RNA virus detection | Influenza, HIV, Hepatitis C, SARS-CoV-2, measles, West Nile virus, Hepatitis E, Poliovirus |
| Gene expression profiling | Determines which genes a cell is actively transcribing (mRNA analysis) |
| Cancer diagnostics | Detection of specific mRNA transcripts, fusion genes (e.g., BCR-ABL in CML) |
| Virology/epidemiology | SARS confirmation requires RT-PCR on ≥2 different clinical specimens |
| Prenatal/genetic diagnosis | Detection of expressed alleles |
Advantages of RT-PCR over Conventional PCR (for RNA targets)
- Can detect RNA - conventional PCR simply cannot amplify RNA; RT-PCR is the only option for RNA viruses and mRNA
- Detects active transcription - mRNA analysis reveals whether genes are being actively expressed, not just present in the genome
- More sensitive for RNA viruses - viral RNA in serum/CSF/stool can be detected at very low copy numbers
- Single-enzyme formats are more specific and efficient than older two-enzyme systems, with fewer secondary structure problems
Part 2: Real-Time PCR (qPCR) and Real-Time RT-PCR
Principle
Real-time PCR monitors amplification as it happens during each cycle, using fluorescent dyes or probes. The fluorescence signal rises as more amplicon is produced, generating the characteristic S-shaped amplification curve.
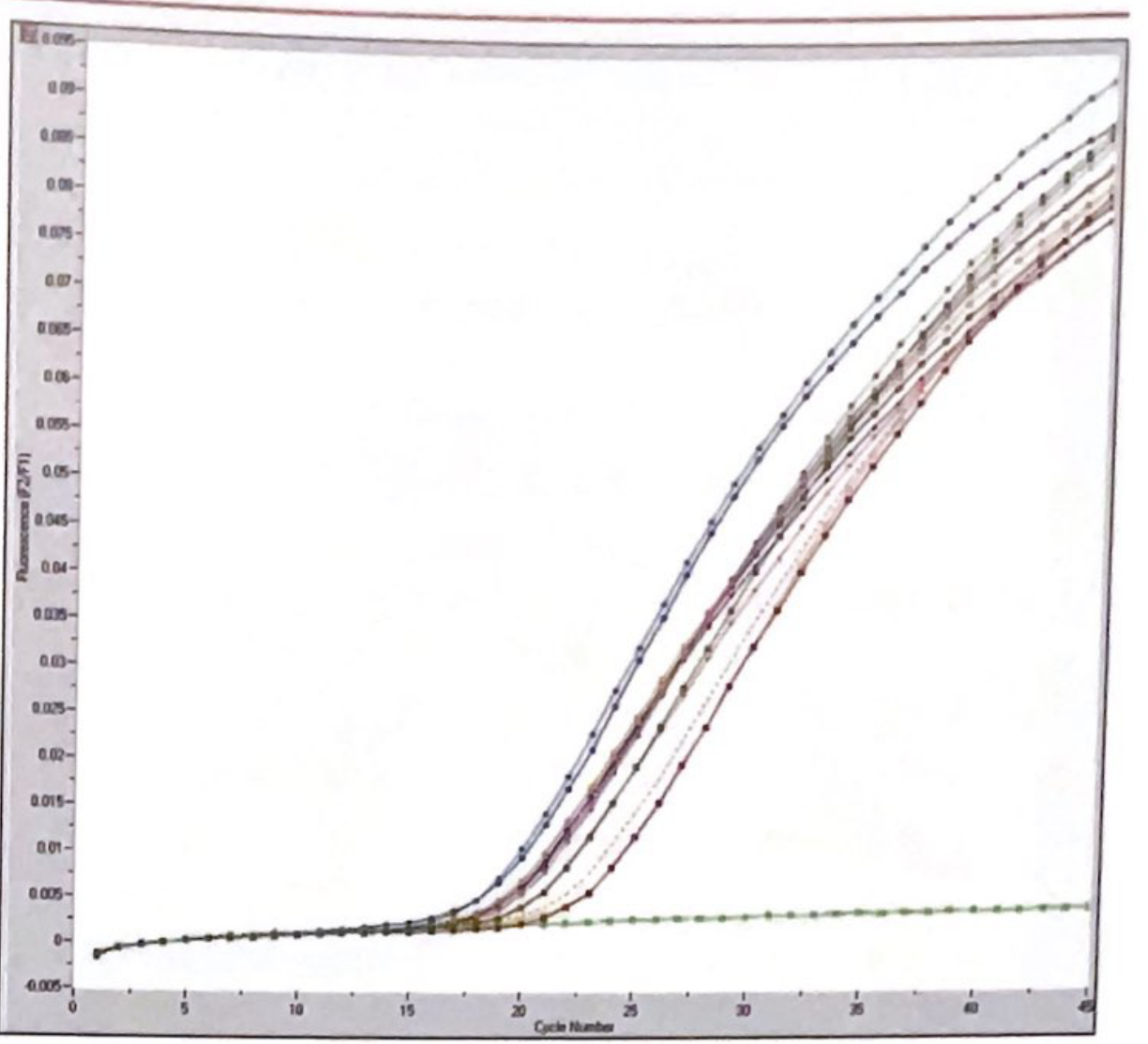
Key concept - Ct (Cycle threshold): The cycle number at which fluorescence crosses a threshold. The Ct value is inversely proportional to the log of initial template concentration - the more target present, the lower (earlier) the Ct.
Detection Chemistries
| Type | Agent | Principle |
|---|---|---|
| Intercalating dyes | SYBR Green I | Binds to ALL double-stranded DNA, fluoresces brightly; non-specific |
| TaqMan probes | Oligonucleotide with fluorophore + quencher | Probe is degraded by Taq's 5'→3' exonuclease activity during extension, releasing fluorescence; highly specific |
| Molecular beacons | Hairpin probe with fluorophore + quencher | Opens on target binding, separating fluorophore from quencher |
| FRET probes | Two adjacent hybridization probes | Fluorescence resonance energy transfer on hybridization |
Uses of Real-Time PCR
| Domain | Application |
|---|---|
| Infectious disease | Quantification of viral load (HIV, HCV, HBV, CMV); bacterial load; SARS-CoV-2 |
| Oncology | MRD (minimal residual disease) monitoring; gene copy number; tumor burden (BCR-ABL quantification in CML) |
| Genotyping | SNP detection; melting curve analysis to distinguish wild-type from variant |
| Blood banking | NAT (nucleic acid testing) for HIV, HCV, HBV in donor blood |
| Rapid karyotype | Quantitative multiplex PCR for rapid prenatal chromosome analysis |
| Gene expression | Quantitative mRNA measurement in research and diagnostics |
Part 3: Advantages of RT-PCR / Real-Time PCR Over Conventional PCR
| Feature | Conventional PCR | Real-Time PCR / RT-PCR |
|---|---|---|
| RNA detection | Not possible | Possible (via reverse transcription) |
| Quantification | Not possible (only qualitative) | Precise quantification (copies/mL) |
| Sensitivity | High but not quantitative | Higher - detects down to ~3 copies/reaction (95% probability) |
| Contamination risk | High - post-PCR handling needed for gel | Greatly reduced - closed-tube system; no post-PCR manipulation |
| Turnaround time | Longer (gel electrophoresis required) | Faster - no gel step; melting curve replaces gel |
| Specificity | Relies on gel band size | Probe-based chemistries add a third level of specificity |
| Multiplex capability | Limited | Multiple targets in one tube with different fluorescent labels |
| Automation | Partial | Fully automatable; reduced hands-on time |
| Gene expression | Cannot assess mRNA expression | mRNA quantification by RT-qPCR is standard |
| Melting curve analysis | Not available | Immediate post-PCR; distinguishes wild-type from mutant; identifies nonspecific products |
| Viral load monitoring | Not applicable | Standard of care for HIV, HBV, HCV, CMV management |
| Closed-tube system | No | Yes - "the most effective way of preventing contamination" |
Key Summary of Advantages (from Tietz Laboratory Medicine, 7e)
"Real-time PCR quickly became the method of choice for most molecular diagnostic laboratories because of its increased sensitivity/specificity and turnaround times... A significant advantage of real-time PCR is the turnaround time with which samples can be analyzed due to the elimination of post-PCR processing steps. Using melting curve analysis instead of gel electrophoresis results in a much faster method for analyzing PCR results."
Clinical Examples Illustrating Superiority
-
COVID-19 (SARS-CoV-2): Real-time RT-PCR is the gold standard - detects viral RNA (not possible with conventional PCR), gives result within hours, closed tube reduces lab contamination
-
HIV management: Real-time PCR measures viral load (copies/mL) to guide ART decisions and monitor treatment response - impossible with conventional PCR
-
CML monitoring: BCR-ABL transcript quantification by RT-qPCR detects minimal residual disease down to 1 cell in 100,000 - conventional PCR cannot provide this sensitivity or quantification
-
MRSA/VRSA evolution: Transposon-mediated resistance spread is studied using RT-PCR gene expression assays to track which resistance genes are being actively transcribed
Sources:
- Tietz Textbook of Laboratory Medicine, 7e - "Reverse Transcriptase-PCR" and "Real-time PCR" sections
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Ch. 69 (Molecular Diagnostics)
- Quick Compendium of Clinical Pathology, 5e - Molecular techniques section
This is a shared conversation. Sign in to Orris to start your own chat.