Explain simple mattress , horizontal matress and vertical mattress when they are used and preferred woth what kind pf suture materials and also suggest me short videos links which i can show during seminar presentation
Reading File
Finding Sources
Finding Sources
Searching the Web
simple interrupted horizontal vertical mattress suture technique video YouTube
Reading File
Reading File
Reading File
Searching the Web
simple interrupted suture technique video YouTube CSL suture tutorial
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Suture Techniques: Simple Interrupted, Horizontal Mattress & Vertical Mattress
1. Simple Interrupted Suture
Technique
The needle enters one skin edge perpendicular to the surface, travels across the wound at depth following the needle's curve, and exits the opposite side symmetrically. A reef (square) knot is tied, with just enough tension to gently evert the wound edges. Each suture is independent.
The key is to pass the needle in a "heart-shaped" arc - entering deeper than the exit point on each side - so the base of the suture is wider than the top. This automatically everts the wound edge and counteracts any tendency to invert during healing.
When to Use
- Most common general-purpose closure - the default skin suture
- Precise edge alignment in areas of moderate tension
- When partial suture removal over time is anticipated (alternating sutures can be removed early while leaving others for support)
- Wounds where edema or impaired healing is a concern (less vascular compromise than running sutures)
- Can be used as buried (deep dermal, absorbable) or epidermal (non-absorbable) sutures
Preferred Suture Materials
| Site | Material | Size |
|---|---|---|
| Face / ears | Non-absorbable monofilament (Nylon/Prolene) | 5-0 or 6-0 |
| Trunk / scalp (high tension) | Nylon / Prolene | 3-0 or 4-0 |
| Neck | Nylon / Prolene | 4-0 or 5-0 |
| Deep/buried layer | Absorbable (Vicryl/PDS) | 3-0 or 4-0 |
- Fitzpatrick's Dermatology, p. 3747
- Pye's Surgical Handicraft, p. 3143
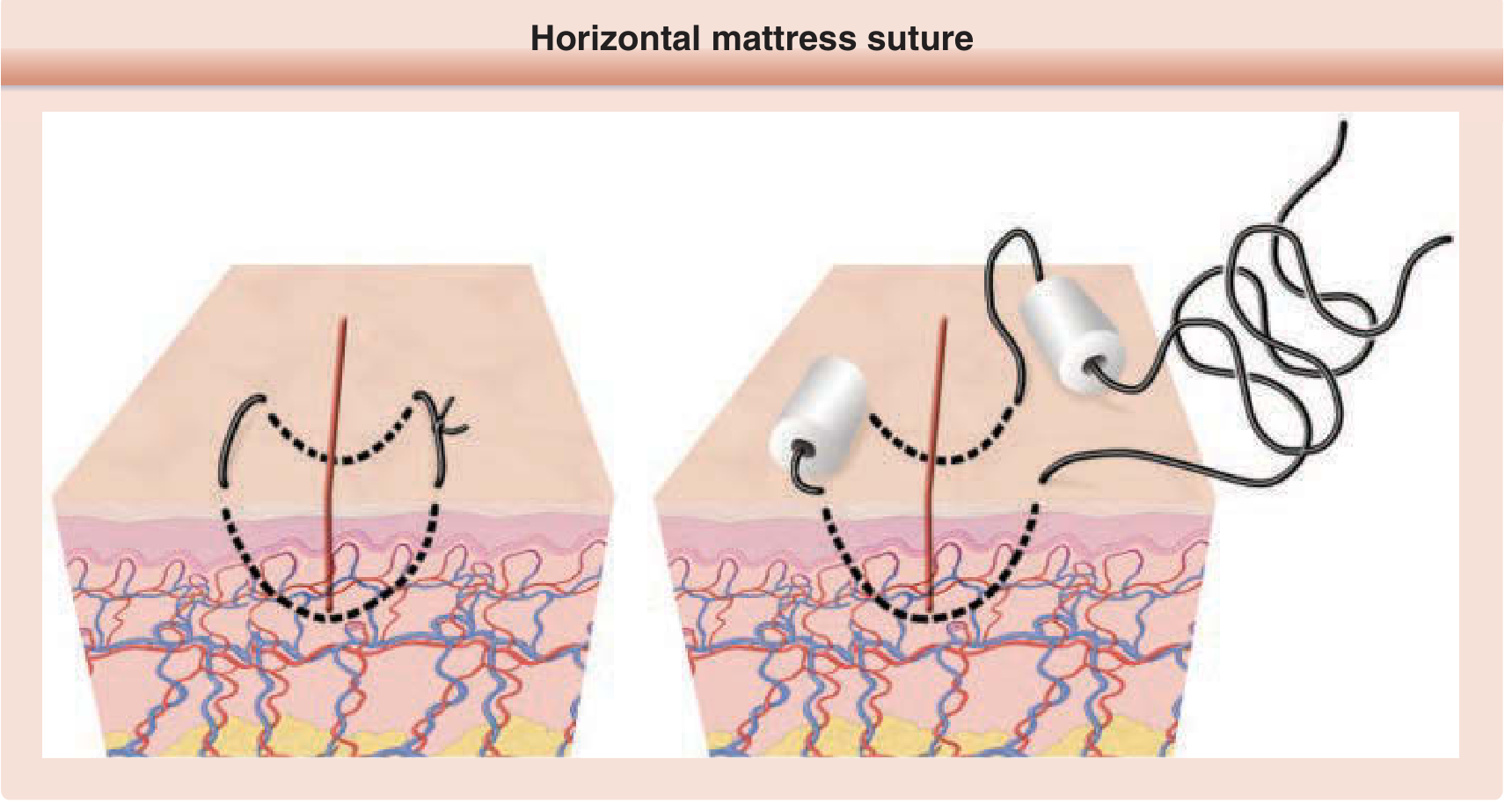
2. Horizontal Mattress Suture
Technique
- Place the first pass just like a simple interrupted suture (through both wound edges)
- Instead of tying, reinsert the needle ~5 mm along the wound (horizontal/parallel to the wound edge) from the exit point
- Pass back through both sides of the wound parallel to the first pass, at the same distance from the wound edge
- Tie the two free ends together, everting the edges
The suture loop lies parallel to the wound - hence "horizontal."
When to Use / Preferred Situations
- High-tension wounds where simple sutures would cut through or tissue would pull apart (e.g., back, shoulder, scalp with little subcutaneous tissue)
- Wounds where strong eversion is needed but subcutaneous tissue is sparse
- Hemostasis in highly vascular wounds (the horizontal loop compresses vessels)
- As temporary bridging sutures in high-tension closures - placed first to approximate edges, allowing buried sutures to be placed more easily, then removed
- Half-buried variant (Gillies corner stitch / 3-point stitch): ideal for suturing the tip/apex of V-shaped flaps (M-plasty, V-Y plasty, rotation flaps) - minimizes flap tip necrosis by avoiding trauma to the dermal vascular plexus
- Can use bolsters (pledgets) under the knot to spread tension and prevent tissue necrosis
Preferred Suture Materials
- Non-absorbable monofilament: Nylon (Ethilon) or Polypropylene (Prolene) 2-0 to 4-0 depending on site and tension
- Must be removed within 1-2 weeks (site-dependent) to avoid suture track scarring and tissue necrosis
- Bolsters or cotton pledgets may be used to protect skin under the knot
Caution: Not recommended on the face. The horizontal and vertical mattress stitches cause more ischemia inside their loops than simple sutures. Alternating the side of the wound on which the knot is tied can reduce wound tension.
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 800
- Fitzpatrick's Dermatology, p. 3747
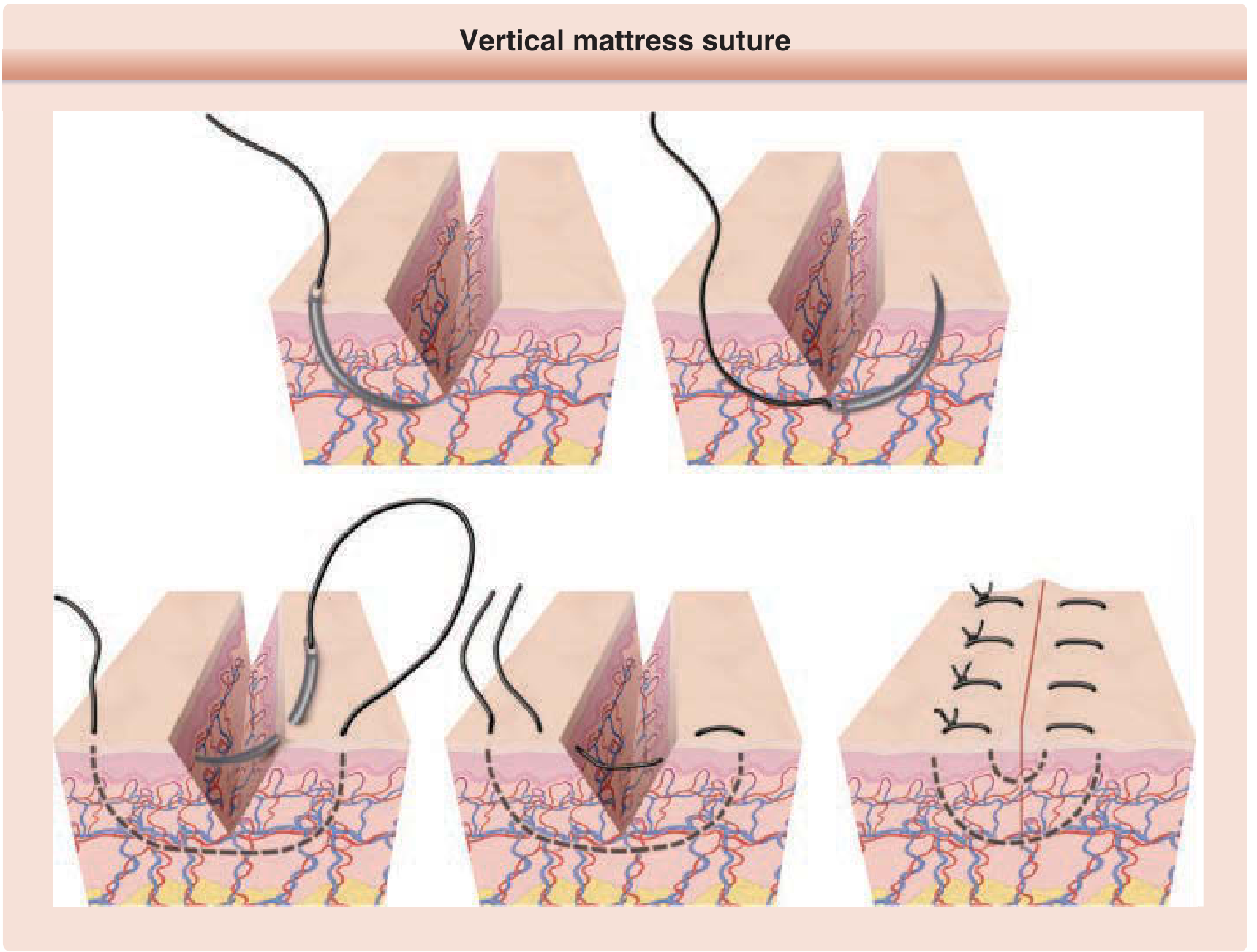
3. Vertical Mattress Suture (Donati Stitch / Far-Near-Near-Far)
Technique
- Outer (far) pass first: Enter skin far from the wound edge (8-10 mm), pass deep across the wound, exit far on the opposite side - like an exaggerated simple suture
- Inner (near) pass back: Reverse direction, reinsert the needle very close to the wound edge on the same side as the exit, pass more superficially (just dermis), exit close to the wound edge on the first side
- Two ends are now on the same side - tie with an instrument tie while everting edges
- Leave ~2 cm of short end outside skin before tying
The suture loop is in a vertical plane perpendicular to the wound - hence "vertical."
When to Use / Preferred Situations
- When maximum wound eversion is needed (the deep far pass everts + closes dead space; the superficial near pass precisely aligns the epidermal edges)
- Combines function of a buried deep suture + epidermal suture in one stitch - useful when layered closure is not possible
- Wounds with significant dead space beneath the skin
- High-tension wounds on the trunk, back, extremities
- When tissue has a strong tendency to invert (wound edges that keep rolling inward)
- Useful when you cannot place buried sutures (infected wound, limited access)
Preferred Suture Materials
- Non-absorbable monofilament: Nylon (Ethilon) or Polypropylene (Prolene) 2-0 to 4-0 for body; 4-0 to 5-0 for less-tension sites
- Must be removed within 1-2 weeks - high risk of paired suture track scars ("railroad tracks") if left too long, especially since this is a high-tension suture that can embed into skin
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 799-800
- Fitzpatrick's Dermatology, p. 3748
- Pye's Surgical Handicraft, p. 3145
Side-by-Side Comparison Table
| Feature | Simple Interrupted | Horizontal Mattress | Vertical Mattress |
|---|---|---|---|
| Plane of suture | Vertical arc | Horizontal / parallel to wound | Vertical, perpendicular to wound |
| Eversion | Moderate | Strong | Very strong |
| Dead space closure | No | No | Yes (deep pass) |
| Tension handling | Moderate | High (bridging) | High |
| Hemostasis | Minimal | Good | Moderate |
| Face use | Yes | Avoid | Avoid |
| Flap tips | Not ideal | Half-buried variant ideal | No |
| Track mark risk | Low (if removed early) | High | Very high |
| Removal timing | 5-14 days (site) | 7-14 days | 7-14 days |
| Preferred material | Nylon/Prolene; Vicryl (buried) | Nylon/Prolene 2-0 to 4-0 | Nylon/Prolene 2-0 to 4-0 |
Recommended Video Links for Seminar Presentation
These are all short, clear, step-by-step HD demonstration videos:
Simple Interrupted Suture:
- Simple Interrupted Suture (CSL - HD) - focused technical execution
- Simple Interrupted + Instrument Tie (CHOP) - great for showing the knot technique
Horizontal Mattress Suture:
- Horizontal Mattress Suture (CSL) - general info + technique demonstration
Vertical Mattress Suture (Donati):
- Vertical Mattress Stitch (CSL) - focused technical execution
- Interrupted Vertical Mattress (A.S.A. Series) - includes measurements (8-10 mm bite)
All three CSL (Clinical Skills Lab) videos follow the same format with an intro and step-by-step breakdown, making them ideal to play back-to-back in a seminar. Each is under 5-6 minutes.
Key clinical pearl: The main disadvantage shared by both mattress sutures is that they cause more ischemia inside the loop than simple sutures. To minimize necrosis: place them at least a few mm from the wound edge, avoid overtightening, use bolsters when needed, and remove them promptly within 7-14 days. - Roberts & Hedges', p. 1335
This is a shared conversation. Sign in to Orris to start your own chat.