Adenoids
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
adenoids anatomy nasopharynx
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of adenoids drawn from authoritative otolaryngology and family medicine textbooks.
Adenoids (Pharyngeal Tonsil)
Anatomy & Location
The adenoid (pharyngeal tonsil) is a mass of lymphoid tissue situated on the posterior wall of the nasopharynx. It is part of Waldeyer's ring — the ring of lymphoid tissue that includes the palatine tonsils, adenoid, and lingual tonsils, which together guard the entrance to the aerodigestive tract. The adenoids sit in close proximity to the eustachian tube orifices and the paranasal sinuses, explaining their role in both otitis media and sinusitis.
Embryology
Adenoids develop at 16 weeks of gestation as a subepithelial infiltration of lymphocytes — later than the palatine tonsil (8 weeks) and lingual tonsil (6.5 weeks).
— K.J. Lee's Essential Otolaryngology
Normal Growth Pattern
The adenoids (along with the palatine tonsils) progressively enlarge between ages 2–8 years and are largest in relation to the airway between 3–6 years of age. They typically involute during adolescence.
— Cummings Otolaryngology
Histology & Epithelium
The luminal surface of the adenoids is comprised of multiciliated and secretory epithelial cells (unlike the posterior pharynx which is dominated by squamous epithelium). This specialized epithelium facilitates antigen sampling and immune surveillance.
— Murray & Nadel's Textbook of Respiratory Medicine
Clinical Significance
1. Adenoid Hypertrophy
Adenoid hypertrophy is common in children. In adults, its presence should raise suspicion for a lymphoproliferative disorder or HIV infection.
Symptoms in children:
- Chronic nasal obstruction and mouth breathing
- Rhinorrhea and postnasal drip
- Snoring and sleep-disordered breathing
- Recurrent otitis media (via eustachian tube dysfunction)
- Cough
Adenoid facies: Children with chronic nasal obstruction from adenoid hypertrophy develop a classic appearance — open-mouth posture, periorbital edema, and a narrow face.
Diagnosis: Usually clinical; confirmed with lateral neck radiography.
— Textbook of Family Medicine
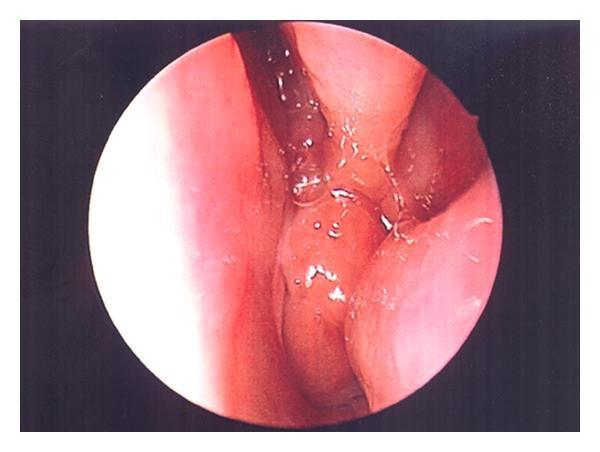
Endoscopic appearance of adenoid hypertrophy:
2. Obstructive Sleep Apnea (OSA)
Enlarged tonsils and adenoids are the most common cause of pediatric OSA, producing nasopharyngeal and oropharyngeal narrowing. Adenotonsillectomy is first-line therapy, with a cure rate of approximately 60%.
— Cummings Otolaryngology
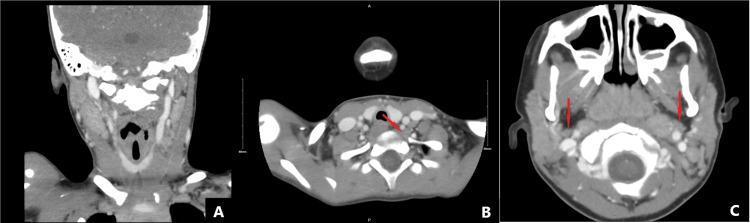
CT imaging — adenoid enlargement with cervical lymphadenopathy:
3. Chronic Rhinosinusitis (CRS)
Adenoids in children with CRS are heavily colonized with biofilm — 88–99% of the mucosal surface area is covered with biofilm, compared with 0–6.5% in children with OSA. The adenoids act as a bacterial reservoir, and their bacteriology mirrors that of the middle meatuses. This explains why adenoidectomy can resolve sinusitis even when adenoid size is not the primary issue.
— Cummings Otolaryngology
4. Otitis Media
Adenoid hypertrophy causes functional obstruction of the eustachian tube, contributing to recurrent acute otitis media (AOM) and otitis media with effusion. Adenoidectomy (regardless of adenoid size) is helpful in children with chronic otitis media with effusion requiring multiple sets of tympanostomy tubes.
— K.J. Lee's Essential Otolaryngology
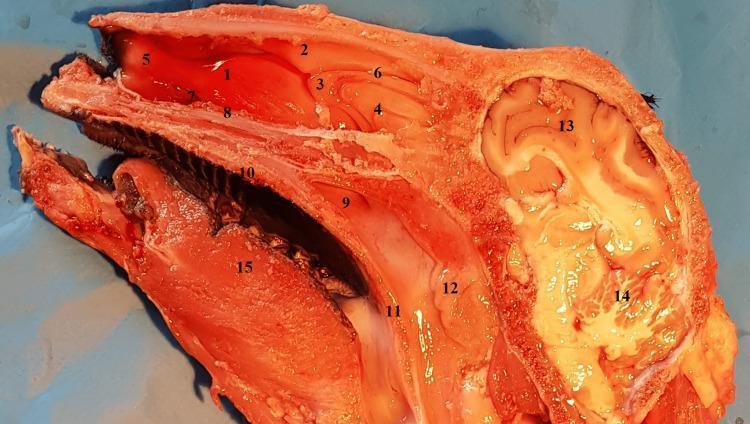
Nasopharyngeal anatomy (sagittal section showing adenoid position):
Indications for Adenoidectomy
| Indication | Notes |
|---|---|
| OSA / adenotonsillar hypertrophy | Adenotonsillectomy; first-line for pediatric OSA |
| Recurrent/chronic AOM | Adenoidectomy ± tubes; especially for multiple tube sets |
| Chronic rhinosinusitis | When adenoid biofilm burden is a driver |
| Dysphagia, speech abnormalities, or occlusive abnormalities due to hypertrophy | Adenotonsillectomy |
| Recurrent acute tonsillitis | 6–7 episodes/year, 5/year for 2 years, or 3/year for 3 years |
— K.J. Lee's Essential Otolaryngology, Cummings Otolaryngology
Key Points Summary
| Feature | Detail |
|---|---|
| Location | Posterior wall of nasopharynx |
| Waldeyer's ring component | Yes (with palatine and lingual tonsils) |
| Embryologic development | 16 weeks (subepithelial lymphocytic infiltration) |
| Peak size | Ages 3–6 years |
| Epithelium | Multiciliated and secretory (not squamous) |
| Adult hypertrophy | Consider lymphoma / HIV |
| Diagnosis | Clinical ± lateral neck X-ray |
| Biofilm role in CRS | Major — adenoidectomy effective even when size is not the driver |
This is a shared conversation. Sign in to Orris to start your own chat.