Mechanism of labour in details note
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and excellent diagrams. Let me compile the detailed note.
Mechanism of Labour - Detailed Note
Overview
The mechanism of labour refers to the series of passive cardinal movements the fetus undergoes to negotiate the birth canal during delivery. These movements are dictated by three factors:
- Pelvic dimensions and configuration (the passage)
- Size and presentation of the fetus (the passenger)
- Strength of uterine contractions (the power)
The fundamental principle is that the fetus follows the path of least resistance, adapting the smallest achievable diameter of the presenting part to the most favorable dimensions and contours of the birth canal.
The following description applies to the vertex presentation, occiput anterior position - the most common and normal presentation.
Prerequisite Terminology
Before understanding the mechanism, key terms must be defined:
| Term | Definition |
|---|---|
| Lie | Relationship of fetal long axis to uterine long axis (longitudinal, transverse, oblique). Longitudinal lie occurs in >99% of term pregnancies. |
| Presentation | The portion of fetal body nearest to or foremost in the birth canal. |
| Vertex/Occiput presentation | Head sharply flexed with occipital fontanelle as presenting part - the normal presentation. |
| Position | Relationship of presenting part to maternal pelvis (left or right). Occiput anterior (OA) is most common and normal. |
| Station | Level of presenting part relative to ischial spines (cm above = negative, below = positive). |
| Biparietal diameter (BPD) | The greatest transverse diameter of the fetal head; ~9.5 cm at term. |
Stages of Labour
| Stage | Onset | Completion |
|---|---|---|
| First (latent + active phases) | Onset of active labour | Complete cervical dilation (10 cm) |
| Second | Complete dilation | Delivery of baby |
| Third | Delivery of baby | Delivery of placenta |
| Fourth | Delivery of placenta | Contracted uterus |
- Contractions in active labour: every 2-3 minutes, lasting ~1 minute, intensity ~40 mmHg
- Uterine contractions cause progressive effacement then dilation to 10 cm
The 7 Cardinal Movements of Labour
The mechanism of labour in vertex presentations consists of:
Engagement → Flexion → Descent → Internal Rotation → Extension → External Rotation (Restitution) → Expulsion
(Note: Some texts list 6 movements, combining engagement with descent)
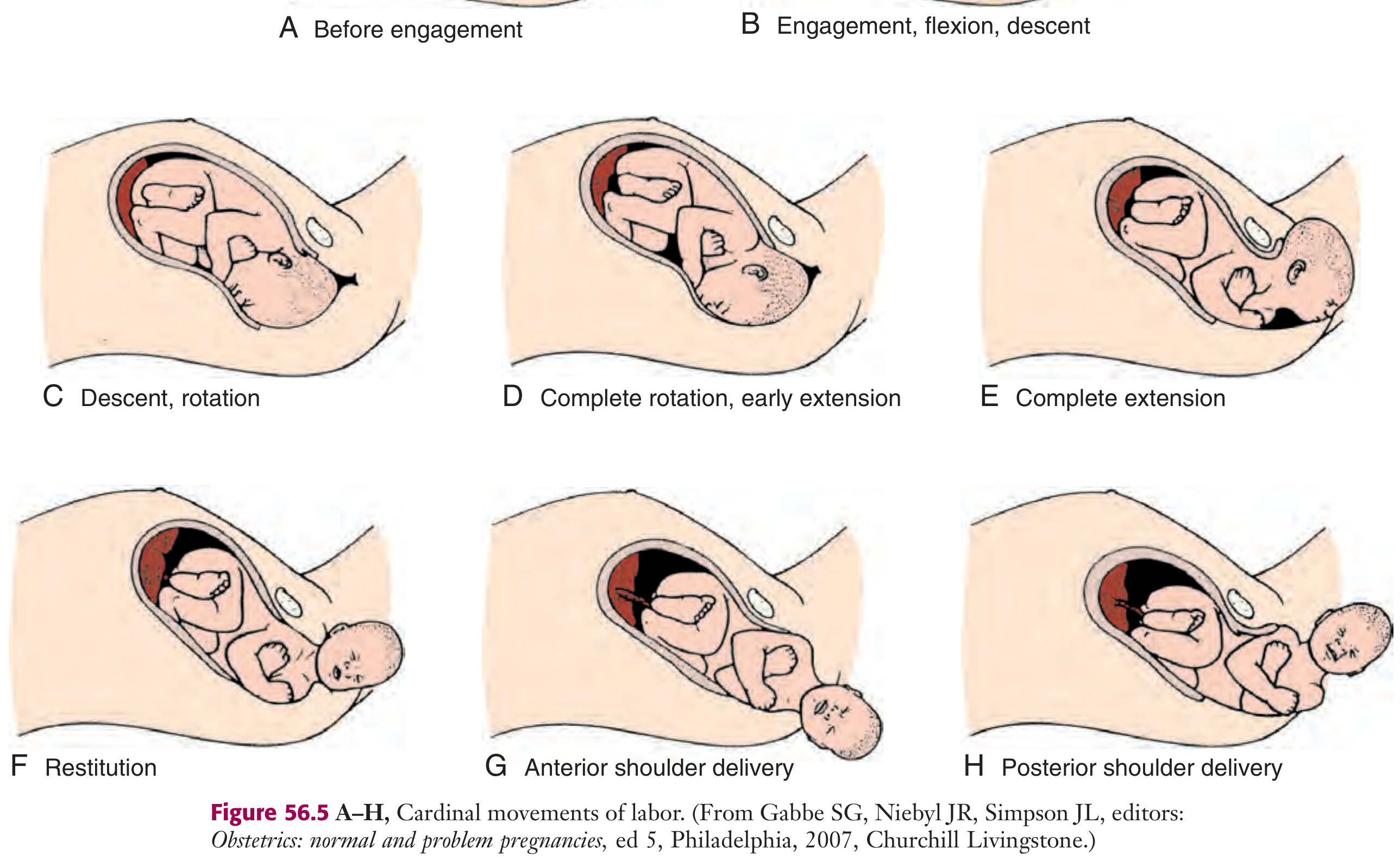
Figure 56.5: Cardinal movements of labour (A-H) - Roberts & Hedges' Clinical Procedures in Emergency Medicine
1. Engagement
Definition: The mechanism by which the greatest transverse diameter of the head - the biparietal diameter (BPD) in occiput presentations - passes through the pelvic inlet.
- The fetus is said to be engaged when the presenting part is at 0 station (level of ischial spines)
- At engagement, the BPD (~9.5 cm) has passed through the pelvic inlet
- Timing:
- In primiparous women: occurs in the last 2 weeks of pregnancy (pre-labour lightening)
- In multiparous women: may occur only at the onset of active labour
- The head typically engages in the transverse diameter of the pelvic inlet in most women
- "Lightening" - the descent of the fetal head into the pelvis before labour - reduces fundal height and increases pelvic pressure
2. Flexion
Definition: Passive bending of the fetal head so the chin approximates the chest, minimizing the presenting cross-sectional diameter.
- Flexion converts the presenting diameter from the occipito-frontal (~11.5 cm) to the smaller suboccipito-bregmatic diameter (~9.5 cm)
- This reduction in diameter is critical for both engagement and descent through the narrow pelvic inlet
- Flexion is a passive movement, occurring as the head encounters resistance from the pelvic floor and cervix
- In most cases, flexion is necessary for both engagement and descent to occur
3. Descent
Definition: The downward passage of the fetal presenting part through the birth canal.
- Descent is gradually progressive but not necessarily continuous
- It is driven by:
- Uterine contractions (primary force)
- Abdominal muscle contractions (bearing down/pushing by the mother)
- Straightening and extension of the fetal body
- In the first stage of labour, descent is slow; it accelerates dramatically in the second stage
- Descent occurs simultaneously with all other cardinal movements - it is the one movement that continues throughout the entire process
- The perineum begins to bulge as the fetal head reaches the introitus
4. Internal Rotation
Definition: The rotation of the fetal head (presenting part) within the pelvis so that the occiput moves from its original transverse position to the anteroposterior position.
- Occurs as the head descends past the ischial spines
- The occiput gradually moves anteriorly toward the symphysis pubis (occiput anterior, OA) - the normal and most common outcome
- Less commonly, the occiput rotates posteriorly toward the hollow of the sacrum (occiput posterior, OP) - this is a malposition that may cause a longer, more difficult labour
- Internal rotation aligns the long axis of the fetal head with the anteroposterior diameter of the pelvic outlet, the widest diameter at that level
- This movement is also passive, driven by the shape of the pelvic floor (levator ani muscles form a gutter that guides the head to rotate anteriorly)
- The head rotates approximately 45 degrees in OA positions (from the oblique or transverse to the anteroposterior diameter)
5. Extension
Definition: After internal rotation, as the flexed head reaches the pelvic outlet and vulvar introitus, the head extends around the subpubic arch.
- The occiput reaches and comes to lie beneath the inferior aspect of the pubic symphysis
- The nape of the neck pivots under the symphysis pubis (the subpubic arch becomes the fulcrum)
- The head then extends (un-flexes) as it rotates upward around the pubic symphysis
- The following structures emerge over the perineum in sequence:
- Occiput
- Bregma (anterior fontanelle)
- Forehead
- Nose
- Mouth
- Chin
- Immediately after delivery, the head drops downward so the chin lies over the maternal anal region
- The attendant supports the perineum with one hand and controls the fetal head with the other, providing gentle counterpressure to prevent rapid, traumatic extension
6. External Rotation (Restitution)
Definition: After delivery of the head, it rotates back to its anatomically correct position relative to the fetal trunk.
- The delivered head rotates to the transverse position it occupied at the time of engagement
- This is because the shoulders, which were engaged in the oblique or transverse diameter of the pelvic inlet, are now internally rotating to align with the anteroposterior diameter of the pelvic outlet (the same process the head underwent)
- External rotation of the head mirrors this internal rotation of the shoulders
- This is also a passive movement
- In OA delivery: the occiput rotates to face the mother's thigh (left or right depending on original fetal position)
- Clinical significance: After external rotation, the attendant checks for nuchal cord (present in ~25-35% of deliveries) and assists shoulder delivery by applying gentle traction
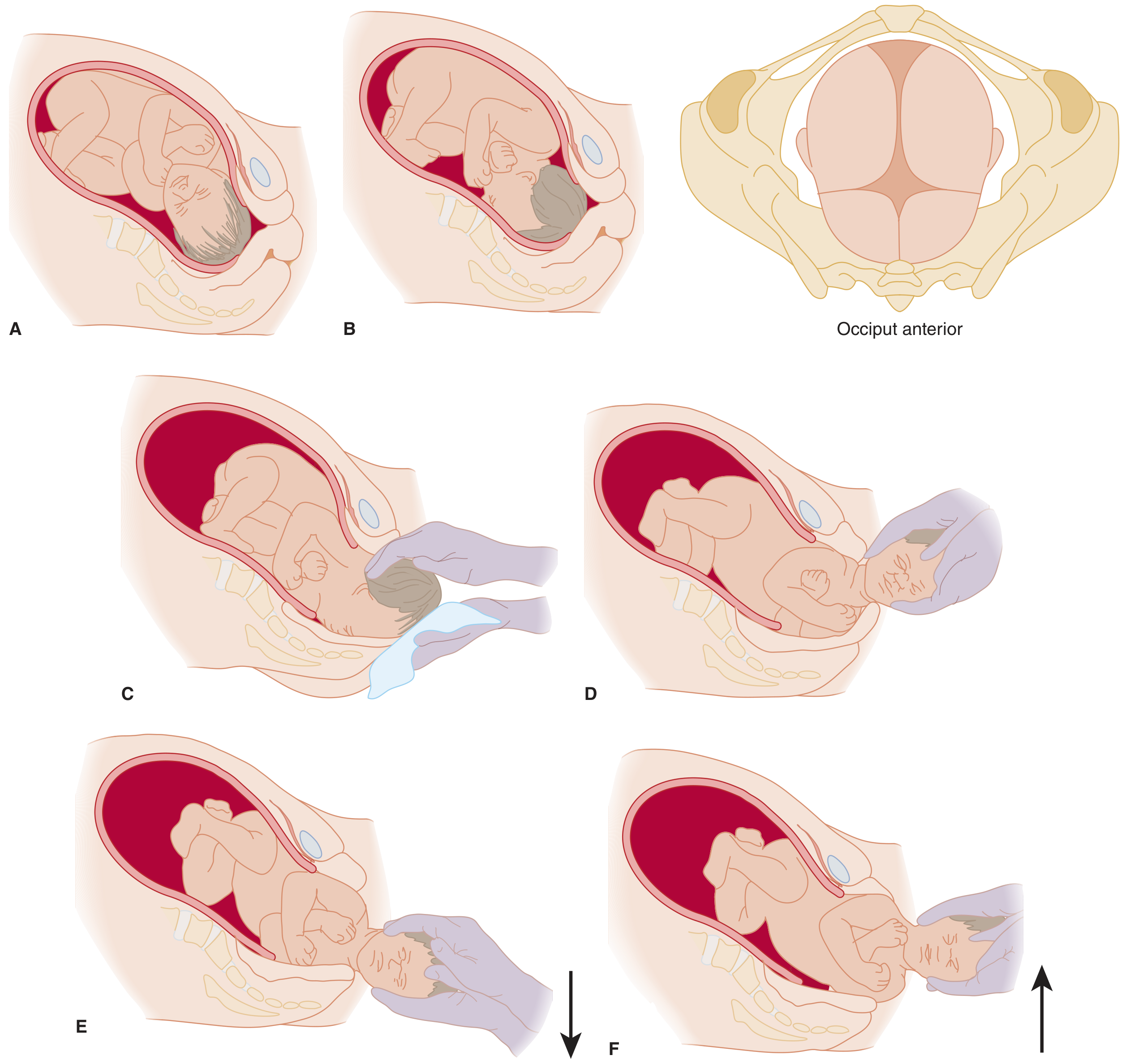
Movements of normal delivery for a vertex presentation - Tintinalli's Emergency Medicine
7. Expulsion
Definition: Delivery of the remainder of the fetal body after delivery of the head and shoulders.
- The shoulders descend in a path similar to that traced by the head
- The shoulders rotate anteroposteriorly for delivery
- Anterior shoulder is delivered first, beneath the symphysis pubis (gentle downward traction on the fetal head)
- Posterior shoulder is then delivered across the perineum (gentle upward traction)
- The remainder of the fetal body follows the axis of the birth canal
- After the anterior shoulder is delivered, the rest of the body delivers quickly
- Caution: Jerky or aggressive traction on the head during shoulder delivery can injure the brachial plexus
Summary Table: Cardinal Movements at a Glance
| Movement | Diameter Entering | Location | Key Point |
|---|---|---|---|
| Engagement | BPD enters inlet | Pelvic inlet | 0 station; lightening in primips |
| Flexion | OFD → SOB diameter | Inlet/pelvic brim | Passive; reduces diameter |
| Descent | Continuous | Throughout canal | Primary movement; driven by contractions |
| Internal rotation | Head turns AP | At ischial spines / mid-pelvis | Occiput → anterior; guided by pelvic floor |
| Extension | Head un-flexes | Pelvic outlet / introitus | Subpubic arch as fulcrum |
| External rotation | Head realigns with trunk | After head delivery | Restitution; reflects shoulder rotation |
| Expulsion | Shoulders and trunk | Pelvic outlet | Anterior shoulder first |
OFD = occipito-frontal diameter; SOB = suboccipito-bregmatic diameter; BPD = biparietal diameter; AP = anteroposterior
Mechanism in Breech Presentation
In breech presentations, the widest engaging diameter is the bitrochanteric diameter (between the greater trochanters of the fetal femurs).
- The hips engage in an oblique diameter of the pelvic inlet
- As descent occurs, the anterior hip descends faster than the posterior
- Internal rotation brings the bitrochanteric diameter into the AP diameter of the outlet
- Lateral flexion allows the anterior hip to catch beneath the symphysis pubis, so the posterior hip is born first
- The body rotates to allow shoulder engagement in an oblique orientation
- The anterior shoulder descends to the AP diameter; posterior shoulder delivers first by lateral flexion
- The head engages in the same diameter as the shoulders
- Subsequent flexion, descent, and rotation of the head bring the posterior neck under the symphysis pubis
- The head is born in flexion
Clinical Notes
- Asynclitism: At engagement, the fetal head may be slightly tilted laterally (anterior or posterior asynclitism). Mild anterior asynclitism is common and self-corrects with descent.
- Moulding: Overlapping of fetal skull bones at the sutures allows the head to adapt to the shape of the birth canal - normal and resolves after birth.
- Caput succedaneum: Oedema of the presenting scalp due to pressure during labour - a normal finding.
- Second stage management: Uterine contractions last up to 1.5 minutes with resting phases <1 minute. The clinician's role is to control the birth, preventing sudden forceful expulsion that could cause perineal or fetal injury.
- Third stage (placental delivery): Placenta normally delivers 10-30 minutes after the infant. Only gentle cord traction is applied - aggressive traction risks uterine inversion.
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine, 7e, pp. 1350-1352 | Tintinalli's Emergency Medicine, 9e, pp. 681-682 | Textbook of Family Medicine, 9e, pp. 502-503
This is a shared conversation. Sign in to Orris to start your own chat.