Doppler velocimetry
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I have comprehensive textbook content and images. Here is a thorough, well-structured answer:
Doppler Velocimetry
Doppler velocimetry uses the Doppler effect to measure blood flow velocity waveforms in fetal and placental vessels. It is the most important non-invasive tool for assessing placental vascular resistance and fetal circulatory status, and its primary clinical application is in the surveillance and management of fetal growth restriction (FGR).
Principle
When ultrasound waves strike moving red blood cells, the reflected frequency is shifted proportional to the velocity of flow. Pulsed-wave Doppler places a sample gate over the vessel of interest and records the characteristic waveform of velocity over the cardiac cycle - a systolic peak and a diastolic component, the ratio of which reflects downstream vascular resistance.
Measured Indices
Three angle-independent indices are used (all are ratios of systolic to diastolic velocities, so they do not require precise angle correction):
| Index | Formula | Notes |
|---|---|---|
| S/D ratio | Peak systole / End diastole | Simple; becomes undefined when diastole = 0 |
| Resistance Index (RI) | (S - D) / S | Ranges 0-1 |
| Pulsatility Index (PI) | (S - D) / mean | Best at extremes; preferred clinically because it still yields a value when diastolic flow is absent or reversed |
The PI gives a better estimate of waveform characteristics than RI or S/D ratio and is the preferred index in clinical practice. - Creasy & Resnik's Maternal-Fetal Medicine, p. 1042
Umbilical Artery (UA) Doppler
The umbilical arteries arise from the common iliac arteries and carry no somatic branches, so they purely mirror placental vascular resistance - they are a direct "window" into placental function.
Normal physiology: As gestation advances, the number of tertiary stem villous vessels in the placenta increases, progressively reducing resistance. UA diastolic flow therefore increases with advancing gestation, and the S/D ratio, RI, and PI all fall.
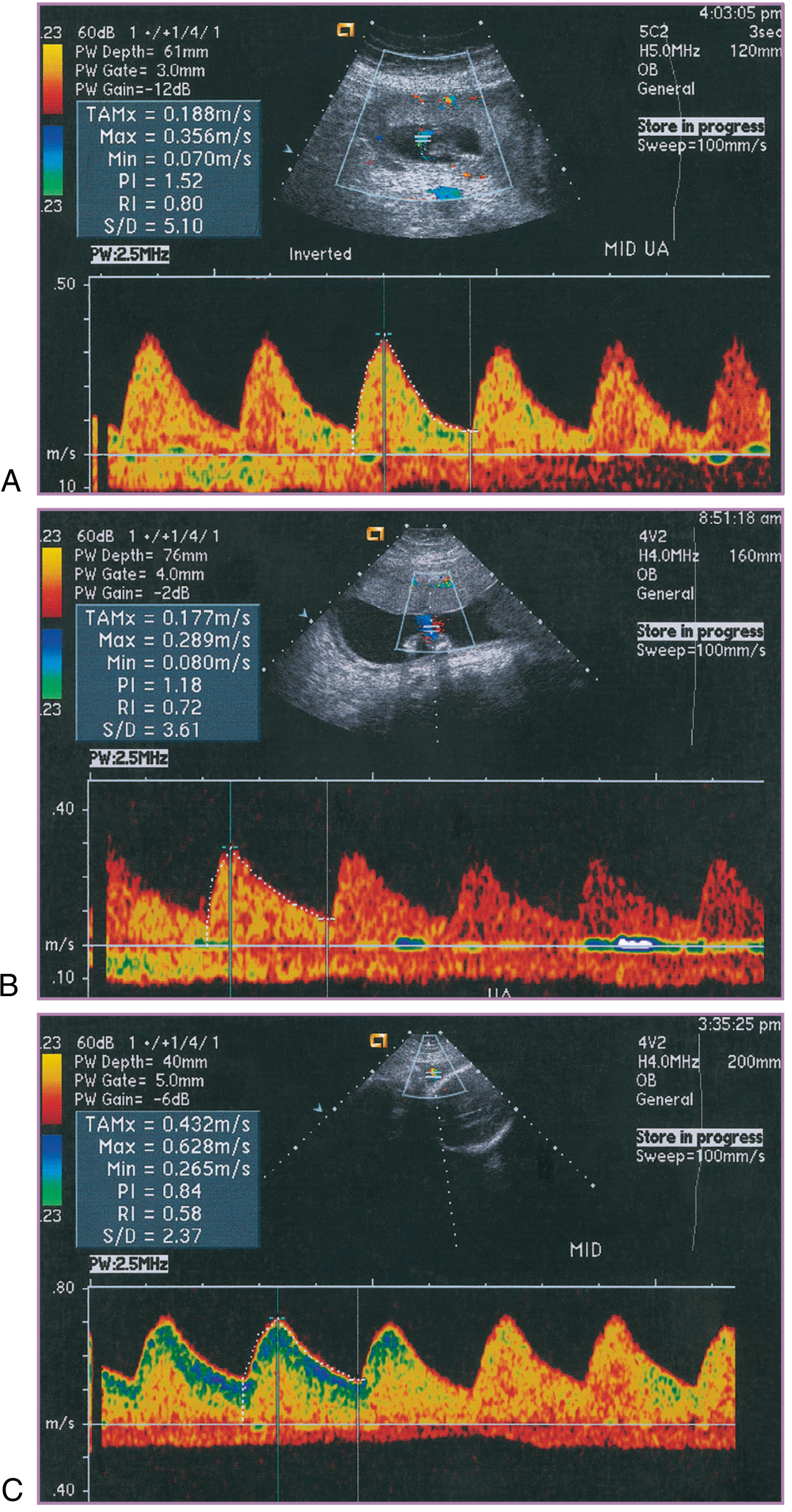
Figure: Normal umbilical artery resistance measured at mid-cord across the three trimesters. Diastolic velocities increase and PI falls progressively (A to C).
Pathologic spectrum: In preeclampsia, FGR, and chronic hypertension, pruning of placental terminal villous vessels raises resistance. As UA resistance rises, diastolic velocity falls progressively through four recognisable stages:
- Elevated PI / high S/D ratio - mildly increased resistance
- Diminished end-diastolic flow - rarely associated with significant neonatal morbidity
- Absent end-diastolic velocity (AEDV) - predicts increased perinatal morbidity and mortality
- Reversed end-diastolic velocity (REDV) - the placenta is so rigid that the pulse pressure causes recoil of the diastolic flow back toward the fetus; 5-fold increase in perinatal mortality vs. AEDV
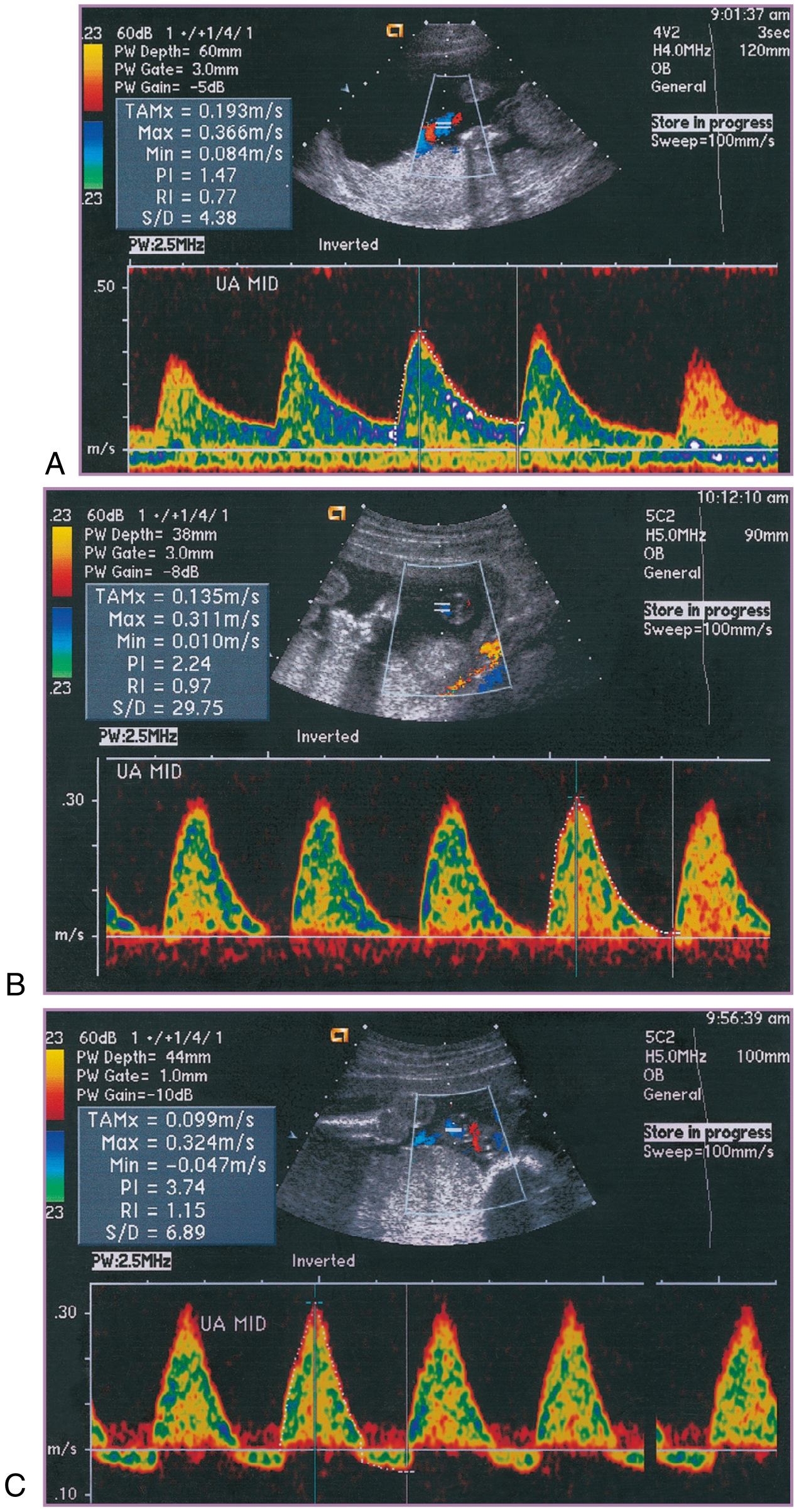
Figure: Progressive UA Doppler abnormality from near-normal at 18 weeks (PI=1.47) through AEDV (PI=2.24) to reversal of flow (PI=3.74, Min velocity = -0.047 m/s). The infant was delivered by caesarean section with umbilical venous pH 7.18.
Measurement technique: The sample gate should encompass the full vessel diameter to sample a single umbilical artery. A free loop of cord in mid-segment is conventionally chosen. Angle of insonation should be minimised (improves waveform quality), though the PI is itself angle-independent.
Clinical evidence: A Cochrane analysis of 19 RCTs confirmed that UA Doppler used in high-risk pregnancies is associated with:
- Fewer perinatal deaths (RR = 0.71; 95% CI 0.52-0.98)
- Fewer inductions of labour (RR = 0.89)
- Fewer caesarean sections (RR = 0.90)
In the PORTO study, small fetuses with normal UA Doppler had an adverse outcome rate of 1.3% vs. 11.5% in those with abnormal flow. - Creasy & Resnik's Maternal-Fetal Medicine, p. 1042
Middle Cerebral Artery (MCA) Doppler
The normal fetal response to hypoxaemia is vasodilatation of the cerebral vasculature to maintain brain oxygen delivery - the "brain-sparing" effect. This produces:
- Reduced MCA PI (increased diastolic flow)
- Reduced MCA S/D ratio
A normal MCA shows high resistance (high PI, low diastolic flow); brain-sparing reverses this.
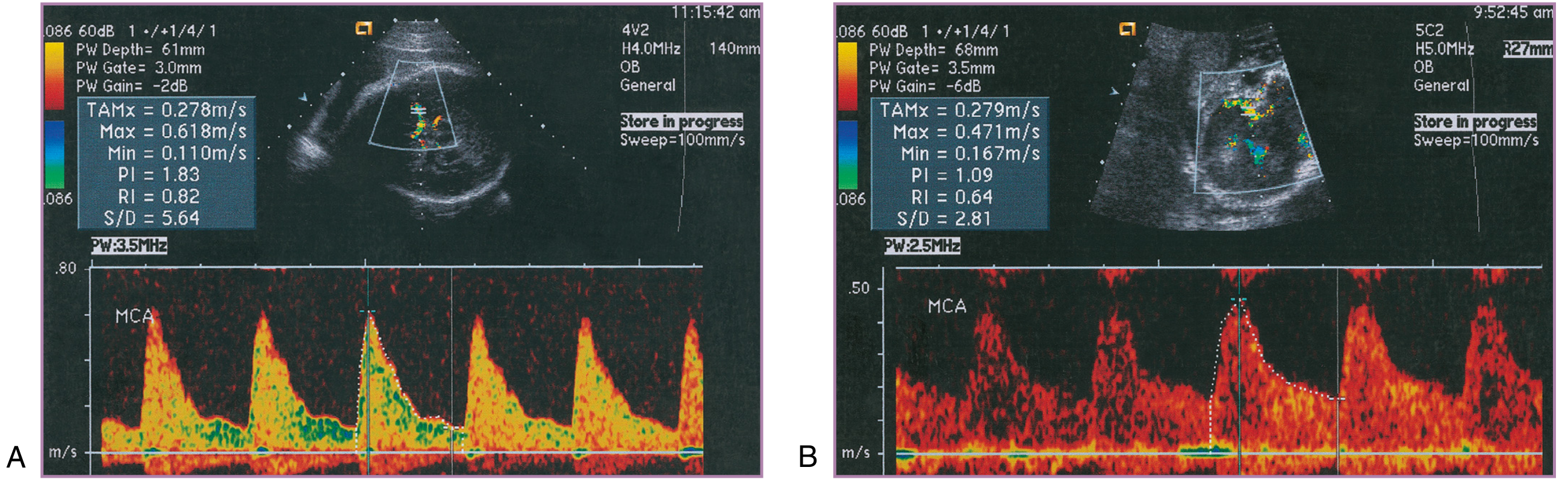
Figure: MCA Doppler centralization of flow. A = normal high-resistance MCA waveform. B = brain-sparing with falling resistance and increased diastolic velocities.
MCA Peak Systolic Velocity (PSV): A separate, independent application - MCA PSV >1.5 multiples of the median (MoM) for gestational age is the standard non-invasive screening tool for fetal anaemia (e.g. in Rh isoimmunisation or parvovirus infection). It has largely replaced invasive cordocentesis for this indication.
Cerebroplacental Ratio (CPR)
CPR = MCA PI / UA PI
A normal fetus has a CPR >1 (MCA resistance > UA resistance). When the CPR falls below 1, it signifies simultaneous placental insufficiency (high UA resistance) and cerebral redistribution (low MCA resistance).
In the PORTO study, adverse neonatal outcome was 18% with CPR <1 vs. 2% with CPR >1. A follow-up 3-year neurodevelopmental assessment showed significantly poorer neurological outcome in FGR fetuses with CPR <1. However, the most appropriate CPR threshold and its additive value over UA PI alone remain under study. - Creasy & Resnik's Maternal-Fetal Medicine, p. 1043
Ductus Venosus (DV) Doppler
The ductus venosus (DV) is a narrow, tapered conduit shunting umbilical venous blood directly into the inferior vena cava (IVC) at the right atrium. Its hourglass shape creates high-velocity flow (Venturi effect), delivering oxygenated blood toward the foramen ovale. The DV waveform has three phases corresponding to cardiac events:
- S-wave (ventricular systole)
- D-wave (ventricular diastole/passive filling)
- a-wave (atrial systole) - the most diagnostically important
Pathologic progression:
- As placental resistance rises, the a-wave becomes progressively deeper (increased afterload)
- Absent a-wave - significant cardiac compromise
- Reversed a-wave - onset of significant cardiac impairment; preterminal in context of severe FGR
- Reversed a-wave, particularly before 30 weeks, is used to help time delivery in AEDV/REDV cases
Uterine Artery Doppler
Doppler of the uterine artery assesses adequacy of trophoblastic invasion of the spiral arteries (physiological conversion). Normally, resistance falls dramatically in the second trimester. Persistent high resistance (elevated PI) or a characteristic "notch" in the diastolic waveform at 20-24 weeks predicts risk of preeclampsia and FGR.
Doppler in Multiple Gestation
UA, MCA, and aortic Doppler findings are similar for singleton, twin, and triplet fetuses. UA Doppler is employed whenever multiple gestation is complicated by significant growth restriction or discordance. - Creasy & Resnik's Maternal-Fetal Medicine, p. 2843
Doppler and IUGR Management Protocol
| Doppler Finding | Management |
|---|---|
| Normal UA + normal MCA | Deliver at 39 weeks; weekly BPP/NST |
| Elevated UA PI or low MCA PI | Twice-weekly NST/BPP from 25 weeks; deliver at 37 weeks |
| AEDV at ≥33 weeks | Proceed to delivery |
| AEDV at <33 weeks | Use NST/BPP to delay; deliver if BPP becomes abnormal |
| REDV at ≥30 weeks | Delivery indicated |
| REDV at <30 weeks | Hospitalise; daily testing; individualize |
| Reversed DV a-wave | Ominous; delivery urgently considered at any gestation |
Summary of Vessel-Specific Information
| Vessel | What it measures | Abnormal finding | Clinical meaning |
|---|---|---|---|
| Umbilical artery | Placental resistance | AEDV, REDV | Placental insufficiency, FGR |
| Middle cerebral artery | Cerebral resistance | Low PI (brain-sparing) | Fetal hypoxaemia, redistribution |
| MCA PSV | Cerebral blood velocity | >1.5 MoM | Fetal anaemia |
| Ductus venosus | Cardiac function + central venous pressure | Absent/reversed a-wave | Cardiac decompensation |
| Uterine artery | Spiral artery conversion | Notch, high PI | Risk of preeclampsia/FGR |
| CPR (MCA PI / UA PI) | Combined placental + cerebral status | <1 | Adverse perinatal outcome |
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (pp. 724, 1042-1045); The Developing Human: Clinically Oriented Embryology (p. 381)
References from williams 26th edition
Finding Sources
Finding Sources
Finding Sources
Unfortunately, Williams Obstetrics 26th edition is not available in the textbook library. The library's obstetrics/gynecology collection contains only:
- Creasy & Resnik's Maternal-Fetal Medicine (which was used for the previous answer)
- Berek & Novak's Gynecology
Williams Obstetrics (26th ed., Cunningham et al., 2022) is not indexed in this database, so I cannot pull direct references or page citations from it.
What I can offer instead:
- The previous answer is fully sourced from Creasy & Resnik's Maternal-Fetal Medicine - the most authoritative dedicated maternal-fetal medicine reference, which covers the same content as Williams with greater depth on Doppler.
- If you have a specific topic or question from Williams (e.g., a specific chapter, table, or clinical scenario), I can search the library for equivalent content from available books.
- If you want, I can also search PubMed for the primary studies that Williams Obstetrics cites on Doppler velocimetry (e.g., the PORTO study, Cochrane reviews on UA Doppler), and present those as citable references.
Would any of these alternatives be helpful?
This is a shared conversation. Sign in to Orris to start your own chat.