Leptospirosis pathogenesis and lab diagnosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
leptospirosis pathogenesis laboratory diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the full answer.
Leptospirosis: Pathogenesis and Laboratory Diagnosis
The Organism
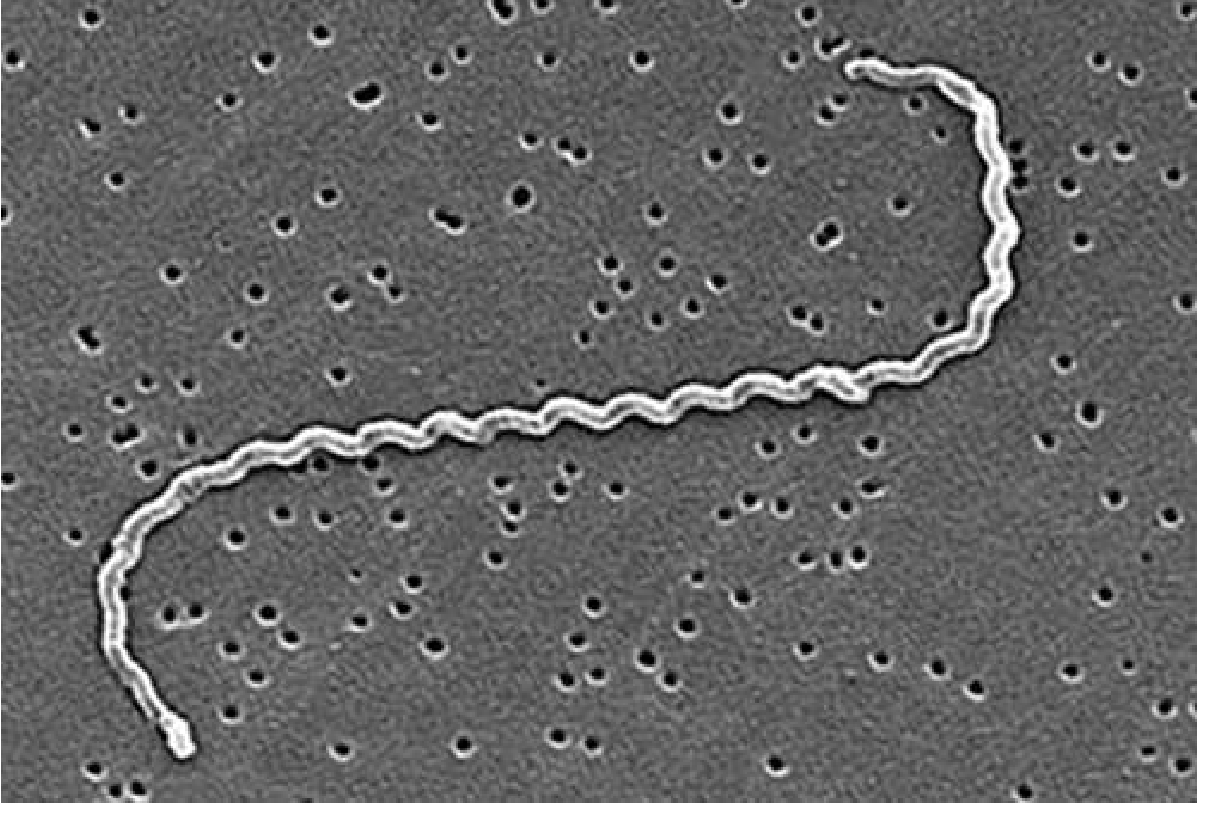
Leptospira interrogans - SEM showing helical morphology and characteristic hooked ends (Goldman-Cecil Medicine)
Leptospira (Greek: leptos = thin, speira = coil) are highly motile spirochetes, 0.1 µm in diameter and 6-20 µm long. The trailing end is hooked, giving the organism a question-mark shape in liquid medium - hence L. interrogans. They are:
- Gram-negative (but do not stain well with Gram stain)
- Aerobic
- Killed rapidly by desiccation, acidic pH, and common disinfectants
- Able to survive for days to weeks in neutral or alkaline water (pH > 7.0)
Over 25 serogroups and 250 serovars are recognised, though serovars have epidemiologic but not clinical significance.
Pathogenesis
Entry and Spread
Leptospires enter the body through:
- Small breaks or abrasions in skin (most common route in water-exposure scenarios)
- Conjunctival mucosa
- Upper alimentary tract mucosa after ingestion
The hooked ends driven by periplasmic flagella allow the organism to actively burrow into tissues. Once inside, leptospires disseminate widely via the bloodstream (leptospiremic phase) to virtually all organs, including the kidney, liver, brain, lungs, and CSF.
Immune Evasion
Leptospires carry a surprisingly rich arsenal of mechanisms to evade the innate immune system:
- Leptospiral proteins bind LPS and peptidoglycan, shielding these targets from pattern-recognition receptors
- Outer membrane proteins (OMPs) bind complement regulators (e.g., factor H), rendering organisms resistant to complement-mediated killing
- Disruption of endothelial cell junctions facilitates dissemination across tissue barriers
Organ-Level Pathogenesis
Kidney (universal involvement):
- Leptospires colonize the proximal renal tubules
- The outer membrane contains cytotoxic glycolipoprotein (GLP) and LipL32 (a highly immunogenic lipoprotein) that impair tubular Na⁺/K⁺-ATPase activity
- This causes impaired sodium/water reabsorption, potassium wasting, and the characteristic paradoxical hypokalemia (non-oliguric AKI stage)
- Histologically: interstitial nephritis with cellular infiltration and edema of the renal interstitium
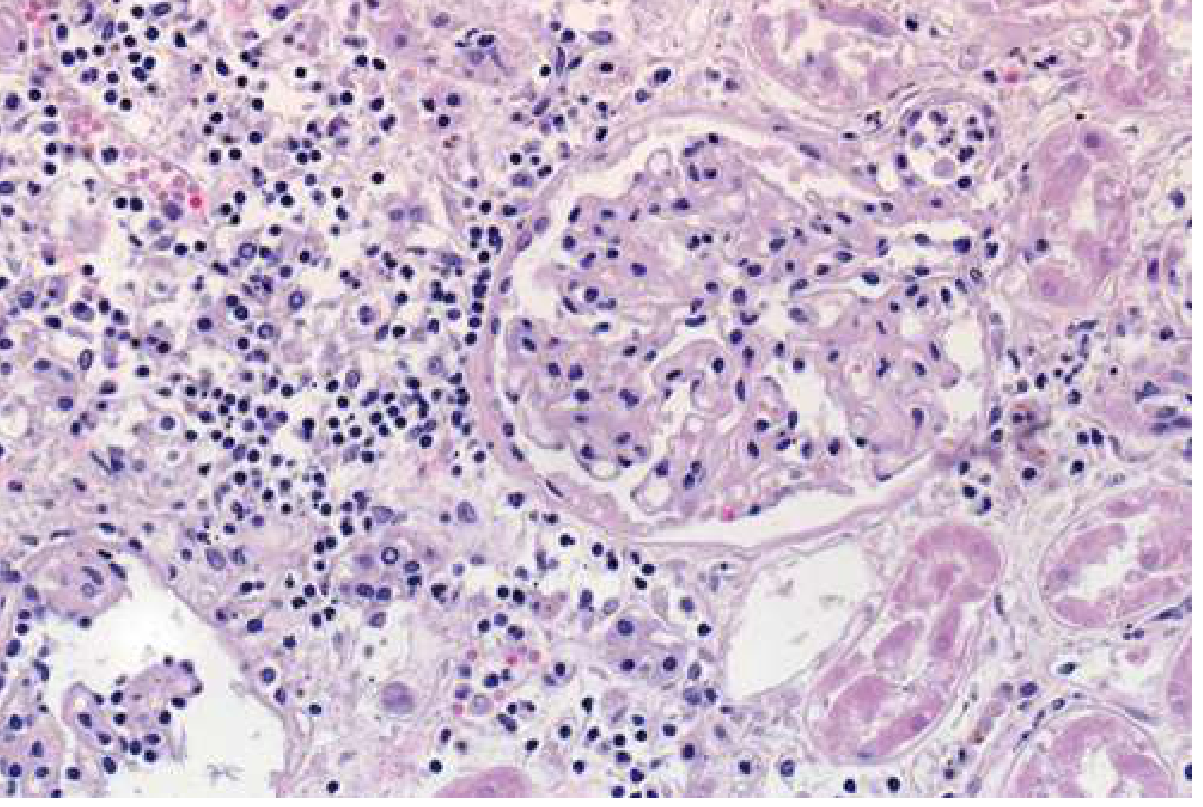
Renal interstitial nephritis in leptospirosis (Goldman-Cecil Medicine)
Liver:
- Leptospires in hepatic sinusoids cause hepatocellular disruption → bile leakage and jaundice
- Aminotransferases are only mildly-to-moderately elevated (unlike viral hepatitis), but direct bilirubin is disproportionately elevated
Lungs:
- Disruption of pulmonary vascular endothelium + thrombocytopenia + coagulation disorders → pulmonary hemorrhage / diffuse alveolar hemorrhage
- This is the most life-threatening feature of severe leptospirosis (Weil's disease variant)
Hemostasis:
- Thrombocytopenia and coagulopathy (elevated PT/INR, aPTT, D-dimer) from vasculitis and endothelial injury
- Usually mild bleeding (petechiae, ecchymoses), but can escalate to severe GI or pulmonary hemorrhage
Biphasic Disease Course
| Phase | Timing | Key Features |
|---|---|---|
| Leptospiremic phase | Days 1-7 | Bacteremia; organisms in blood, CSF, urine; high fever, chills, myalgia, conjunctival suffusion |
| Immune (leptospiruric) phase | Days 7-14+ | Agglutinating antibodies appear; bacteremia clears; immune-mediated organ damage; Weil's disease may manifest |
The rising antibody titer during the second phase suggests an immunologic component to pathogenesis - this is why antibiotics are less effective once this phase begins, and why leptospires are typically absent from CSF in leptospiral meningitis despite meningitic signs.
Weil's Disease (Severe Leptospirosis)
Caused predominantly by L. interrogans serovar Icterohaemorrhagiae. Defined by the classic triad:
- Jaundice (direct hyperbilirubinemia)
- Acute renal insufficiency (AKI)
- Bleeding (thrombocytopenia, coagulopathy)
With multiorgan failure (ARDS, shock, myocarditis), mortality can reach 10-40%.
Laboratory Diagnosis
A high index of suspicion is needed. Diagnosis is staged by timing in the disease course:
1. Direct Detection Methods
| Method | Optimal Timing | Comments |
|---|---|---|
| PCR (DNA amplification) | Days 1-7 (leptospiremic phase) | Most sensitive early method; performed on blood, urine, or CSF; increasingly feasible even in resource-limited settings |
| Blood culture | Days 1-7 | Requires special media (EMJH/Fletcher's); organisms take weeks to grow (slow, rarely attempted); collect before antibiotics |
| Urine culture | Days 7-14+ | Organism shed in urine during/after immune phase |
| Dark-field microscopy | Theoretically early | Not recommended - very low yield, high false positives from fibrin and debris |
2. Serological Methods (Mainstay of Diagnosis)
Microscopic Agglutination Test (MAT) - Gold Standard
- Uses live or formalin-killed leptospires of multiple serovars
- Patient serum at increasing dilutions is mixed with antigen; agglutination read under dark-field microscopy
- Diagnostic criteria:
- Seroconversion (negative → positive)
- Four-fold rise in titer between acute and convalescent samples
- Single titer ≥ 1:400 (in endemic areas, ≥ 1:800)
- Limitations: Limited to reference labs; requires expertise and live antigen maintenance; serovars vary by region
IgM-based Tests (Genus-specific)
- IgM ELISA: IgM antibodies become detectable during the first week of illness; widely used for acute diagnosis
- Lateral flow / dipstick rapid tests: FDA-approved kits available (e.g., Leptocheck-WB, Lepto Tek Dri Dot); useful in endemic areas
- Limitation: May cross-react with other spirochetal infections (Lyme, syphilis); not serovar-specific
3. Non-specific Laboratory Findings
These support the diagnosis and assess severity:
| Investigation | Typical Finding |
|---|---|
| CBC | Leukocytosis (>80% neutrophils), thrombocytopenia |
| Coagulation | Elevated PT/INR, aPTT, D-dimer |
| LFTs | Mild-to-moderate ALT/AST elevation; disproportionately high direct bilirubin |
| Renal function | Elevated BUN and creatinine; urinalysis shows pyuria, hematuria, proteinuria |
| Electrolytes | Hypokalemia (paradoxical - due to tubular potassium wasting despite oliguria) |
| CSF | Aseptic meningitis picture: increased cells (predominantly lymphocytes), elevated protein, normal glucose |
| Chest CT | Diffuse ground-glass opacities and airspace nodules (diffuse alveolar hemorrhage) |
| CRP / Procalcitonin | Both elevated; helpful to differentiate from dengue (usually normal in dengue) |
Diagnostic Approach by Disease Stage
Day 1-7 (Leptospiremic Phase):
→ PCR on blood/CSF (most sensitive)
→ Blood culture (EMJH medium, but results take weeks)
→ IgM ELISA (may be negative this early)
Day 7-14+ (Immune Phase):
→ MAT (paired sera: acute + convalescent)
→ IgM ELISA (now usually positive)
→ Urine PCR or culture
→ Non-specific labs for severity assessment
Key Summary Points
- Leptospirosis is a biphasic illness - direct bacterial damage in phase 1, immune-mediated damage in phase 2
- The kidney is universally involved; non-oliguric AKI with hypokalemia is characteristic
- MAT is the gold standard serologic test but requires reference labs; paired sera 4-fold rise is diagnostic
- PCR is the most sensitive test in the first week (leptospiremic phase)
- Dark-field microscopy is not recommended due to poor sensitivity and specificity
- Procalcitonin and CRP help distinguish leptospirosis from dengue (a common mimicker)
- Treatment: penicillin (all forms), doxycycline or ceftriaxone as alternatives
Sources: Goldman-Cecil Medicine (29e), Sherris & Ryan's Medical Microbiology (8e), Comprehensive Clinical Nephrology (7e), Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.