Lscs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of LSCS (Lower Segment Caesarean Section):
Lower Segment Caesarean Section (LSCS)
LSCS refers to a caesarean delivery performed through the lower uterine segment, specifically using the low transverse (Kerr) incision - the most widely used technique today. It replaced the older classical (fundal) incision due to significantly better outcomes.
Definition & Historical Context
The evolution of caesarean delivery into a safe procedure is one of the most important developments in modern perinatal medicine. 19th-century maternal mortality from caesarean operations was 85% or greater. Introduction of the low-segment incision - which allows exclusion of the uterine wound from the peritoneal cavity - dramatically reduced postoperative peritonitis. Further advances (blood transfusion, antibiotics, regional anesthesia) reduced mortality to nearly zero in skilled hands. - Creasy & Resnik's Maternal-Fetal Medicine, p. 958
Types of Uterine Incision
There are three main options for the uterine incision:
| Type | Name | Notes |
|---|---|---|
| Low transverse | Kerr incision | Standard; LSCS proper; best healing, allows VBAC |
| Low vertical | Krönig incision | Used for preterm, transverse lie, anterior placenta previa |
| Classic (fundal) | Classical CS | Upper segment; reserved for emergencies; highest rupture risk |
The Kerr (low transverse) incision is preferred because:
- Heals well
- Lower risk of rupture in subsequent pregnancies
- The uterine wound can be covered by bladder peritoneum, reducing risk of ileus, peritonitis, and adhesions
- Pfenninger & Fowler's Procedures for Primary Care, p. 1135; Creasy & Resnik, p. 964
Indications
Caesarean delivery is indicated any time delivery must be accomplished and vaginal delivery poses greater risk to the mother or fetus than abdominal delivery. Common indications include:
Fetal indications:
- Fetal distress / non-reassuring CTG
- Malpresentation (breech, transverse lie)
- Very low birth weight (<1500 g)
- Fetal spinal or abdominal wall abnormalities
- Active genital herpes at onset of labour
- Cord prolapse
Maternal indications:
- Placenta previa / placenta accreta
- Cephalopelvic disproportion (CPD)
- Failure of labour to progress (dystocia)
- Previous uterine surgery / prior CS with classical incision
- Severe preeclampsia with failed induction
- Maternal HIV (for prevention of vertical transmission)
Other:
- Multiple gestation with non-vertex first twin
- Macrosomia (EFW >4500 g, or >4000 g in diabetic mother)
- Repeat caesarean
- Elective (maternal request - controversial)
Four indications account for 90% of the increase in CS rates in the US: dystocia, repeat CS, breech presentation, and fetal distress. - Creasy & Resnik, p. 958
Contraindications
There are no absolute contraindications - it is considered a life-saving procedure. The only relative contraindication is patient refusal after full informed consent. - Pfenninger & Fowler, p. 1135
Pre-operative Preparation
- Obtain informed consent (risks: anesthesia complications, bladder/ureter injury, bowel injury, hemorrhage, infection, hysterectomy, fetal injury, uterine rupture in future labours)
- IV antibiotic prophylaxis: cefoxitin 1 g IV (or clindamycin 600 mg if penicillin-allergic) - administered after cord clamping
- Left lateral tilt (wedge under right hip or table tilt) to avoid aortocaval compression
- Insert urinary catheter
- Regional anesthesia preferred (spinal or epidural)
Step-by-Step Surgical Technique (Low Transverse / Kerr)
- Position: Left tilt to decompress the aorta and inferior vena cava
- Anaesthesia: Spinal, epidural, or general
- Skin incision: Pfannenstiel incision - ~13-15 cm, 2 fingerbreadths above the symphysis pubis, using a no. 20 blade
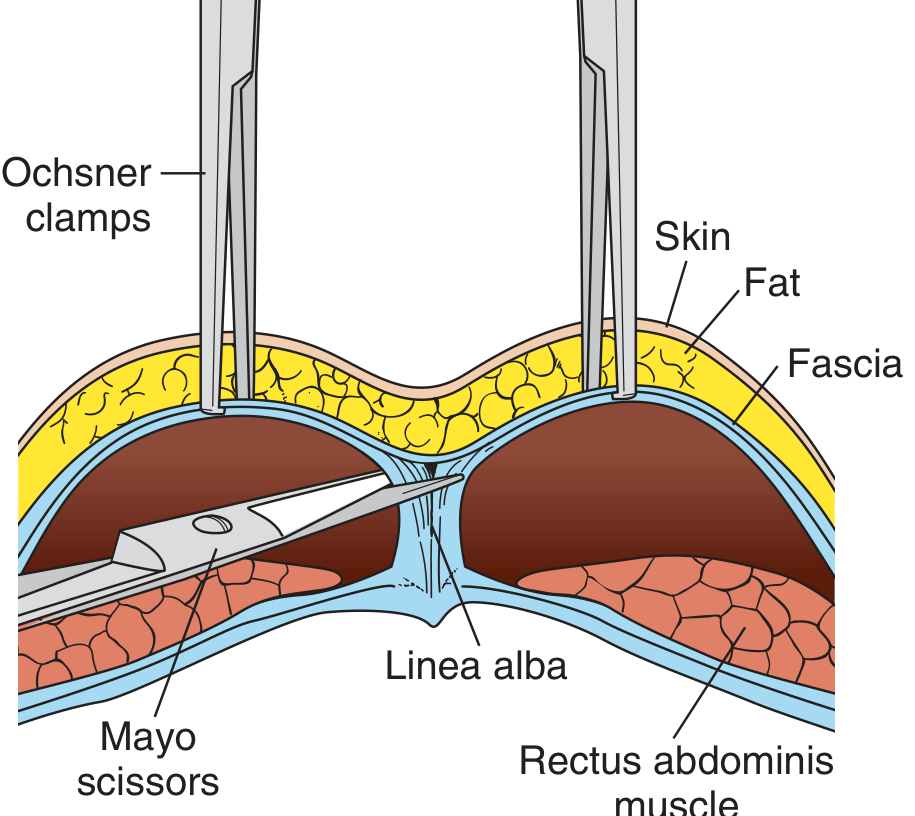
- Fascia: Incise and extend laterally and superiorly in a curvilinear fashion with curved Mayo scissors
- Rectus muscles: Separate bluntly in the midline (vertically)
- Peritoneum: Tent with two hemostats, incise above the urachus; extend bluntly
- Bladder retraction: Place DeLee bladder blade
- Bladder flap: Pick up vesicouterine peritoneum, incise transversely, and bluntly dissect bladder inferiorly away from the lower uterine segment; reapply blade
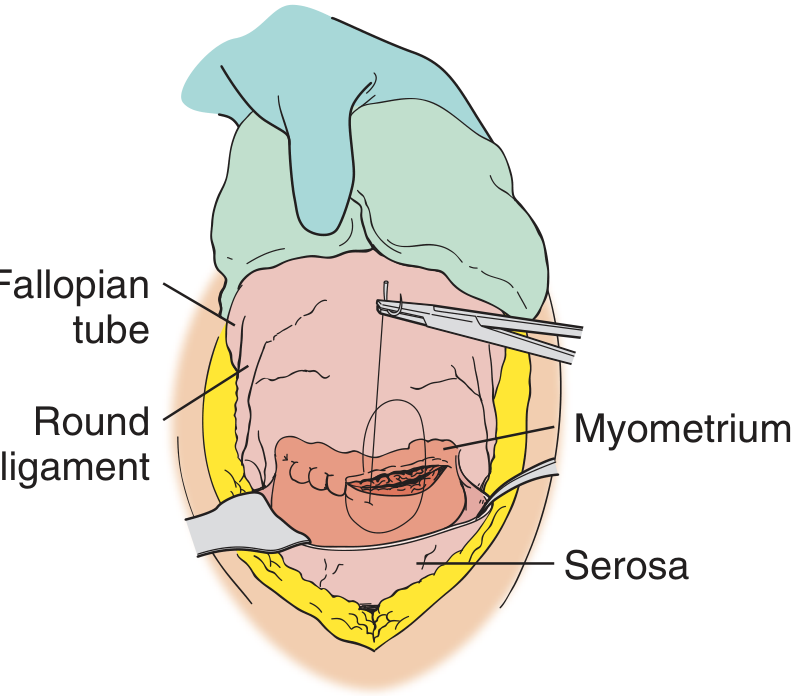
- Uterine incision: Score the lower uterine segment over the fetal head with a no. 20 blade (2-3 cm initial incision, millimeter by millimeter to avoid injuring fetal parts). Announce "uterine incision" to alert anesthesiologist and neonatologist
- Extend incision: Bluntly with fingers, or with bandage scissors (superolaterally) - total ~10-11 cm
- Rupture membranes: With Allis clamp (if intact)
- Deliver fetal head: Cupped hand over occiput, wrist straight, lift upward - assistant applies gentle fundal pressure. If head is deeply impacted, assistant pushes from below vaginally
- Deliver shoulders and body: Suction mouth and nose; deliver anterior shoulder then posterior shoulder. Clamp and cut cord
- Deliver placenta: Manual extraction bluntly with fingers; remove membranes with ring forceps
- Uterine closure: Running locked stitch of 0 chromic catgut (or Vicryl) - uterus may be exteriorized or closed in situ
- Peritoneal closure: Optional
- Fascial closure: Continuous absorbable suture
- Skin closure: Subcuticular or staples
- Pfenninger & Fowler's Procedures for Primary Care, pp. 1136-1138
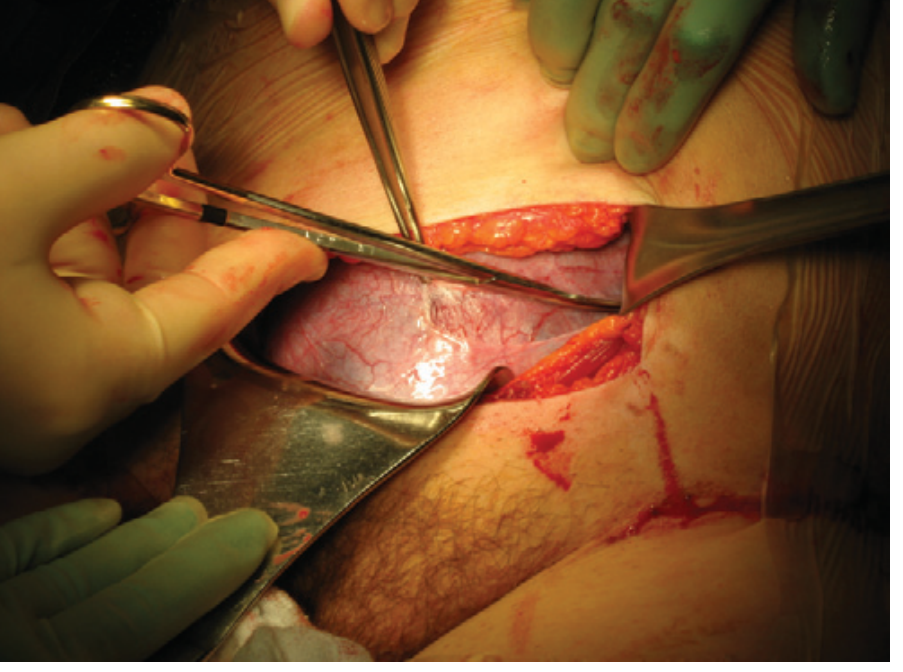
Surgical Images
Complications
Intraoperative (~2% of CS):
- Anesthesia accidents (aspiration, failed intubation, drug reactions)
- Hemorrhage
- Bladder laceration (10x more common than in operative vaginal delivery)
- Bowel injury (especially with adhesions from prior surgery)
- Amniotic fluid embolism
- Uterine extension (especially into uterine vessels)
- Scalpel laceration of fetus (rare)
Immediate postoperative:
- Atelectasis
- Endomyometritis
- Urinary tract infection
- Wound hematoma, dehiscence, infection, or necrotizing fasciitis
- Thromboembolic disease (DVT/PE)
- Paralytic ileus
Long-term:
- Repeat CS in subsequent pregnancies (>75% in the US)
- Uterine rupture in subsequent labour (0.5-1% with low transverse scar)
- Placenta previa or accreta (2-3x increased risk, rising with each CS)
- Ectopic pregnancy / scar ectopic
- Infertility (possibly from postpartum infection / tubal damage)
- Intraabdominal adhesions leading to bowel obstruction
- Creasy & Resnik, pp. 960-962
Vaginal Birth After Caesarean (VBAC)
Previous LSCS with a low transverse uterine incision and a non-recurring indication does NOT mandate repeat CS. A trial of labour (TOLAC) is appropriate in suitable candidates:
- Non-recurrent indication for prior CS
- One prior vaginal birth
- Spontaneous labour onset
- Facility with capacity for emergency CS
Risk of uterine rupture with TOLAC after one low-transverse CS: 0.5-1.0% (much lower than after classical incision). Major complications are significantly higher in failed VBAC attempts. Women with >80% probability of vaginal success are ideal candidates. - Creasy & Resnik, p. 963
Classical incision substantially increases rupture risk and usually mandates elective repeat CS before labour onset.
Anaesthesia Considerations
- Spinal anaesthesia is the most common method - rapid onset, reliable block
- Epidural preferred when epidural already in place for labour
- CSE (combined spinal-epidural) is also used
- General anaesthesia reserved for true emergencies or when regional is contraindicated
- Key risk: maternal hypotension from sympathetic block - managed with left lateral tilt, IV fluids, vasopressors (ephedrine/phenylephrine)
- Intubation for GA carries aspiration risk (full stomach in pregnancy) - rapid sequence induction mandatory
Key Points Summary
| Feature | Detail |
|---|---|
| Incision type | Pfannenstiel (skin); low transverse Kerr (uterus) |
| Anesthesia | Spinal preferred |
| Prophylactic antibiotic | Single dose after cord clamping |
| Uterine closure | 1 or 2 layer running locked absorbable suture |
| VBAC eligibility | Yes, after low transverse incision |
| Repeat CS scar rupture | 0.5-1% |
| Most common indication | Dystocia / failure of labour to progress |
This is a shared conversation. Sign in to Orris to start your own chat.