Malaria from basics to clinical with differential diagnosis
Reading File
Finding Sources
Searching PubMed
"malaria"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have rich, comprehensive data from Harrison's 22E (2025), Robbins Pathology, and Rosen's Emergency Medicine. Let me compose the full answer.
Malaria: From Basics to Clinical with Differential Diagnosis
"Humanity has but three great enemies: Fever, famine, and war; of these by far the greatest, by far the most terrible, is fever." - William Osler, 1896
1. Overview and Epidemiology
Malaria is a protozoan disease transmitted by the bite of infected female Anopheles mosquitoes and remains the most important parasitic disease of humans. In 2022, there were an estimated 249 million cases in 85 endemic countries and 608,000 deaths (~1,660 deaths per day). Sub-Saharan Africa bears the overwhelming burden.
Geographic distribution:
- P. falciparum - predominates in sub-Saharan Africa, New Guinea, Hispaniola
- P. vivax - Central/South America, most of Asia, Horn of Africa
- P. malariae - most endemic areas, especially sub-Saharan Africa
- P. ovale - mainly Africa
- P. knowlesi - Southeast Asia (from macaque monkeys)
2. Causative Species
Six species of Plasmodium cause human malaria:
| Species | Fever Cycle | Intrahepatic Phase | Hypnozoites | Notes |
|---|---|---|---|---|
| P. falciparum | 48 h (tertian) | 5.5 days | No | Most lethal; high parasitemia possible |
| P. vivax | 48 h (tertian) | 8 days | Yes | Relapses; invades reticulocytes |
| P. ovale (curtisi & wallikeri) | 48 h | 9 days | Yes | Mild disease; two subspecies |
| P. malariae | 72 h (quartan) | 15 days | No | Low parasitemia; nephrotic syndrome |
| P. knowlesi | 24 h | 5 days | No | Monkey parasite; rapidly rising parasitemia; severe disease possible |
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 231
3. Life Cycle and Pathogenesis

Life cycle of P. falciparum showing hepatic and erythrocytic stages (Robbins & Kumar Basic Pathology)
Hepatic (Pre-erythrocytic) Stage
- Infected female Anopheles mosquito injects sporozoites during a blood meal
- Sporozoites travel to the liver within minutes, binding hepatocytes via thrombospondin-related adhesive protein and circumsporozoite protein (binding heparan sulfate proteoglycans)
- Intrahepatic schizogony: one sporozoite produces 10,000-30,000 daughter merozoites
- Infected hepatocytes burst, releasing merozoites into the bloodstream
- In P. vivax and P. ovale, some forms remain dormant as hypnozoites (cause of relapses weeks to years later)
Erythrocytic Stage
- Merozoites invade red blood cells (RBCs) - via binding to glycophorin (sialic acid residues) using a lectin-like molecule
- Intraerythrocytic stages: ring trophozoite → trophozoite → schizont → merozoites (rupture and re-invade every 48 h for most species, 24 h for P. knowlesi)
- Some trophozoites differentiate into gametocytes (the mosquito-infective stage)
- When parasitemia reaches ~50/μL blood (~100 million parasites total), symptomatic illness begins
Key Pathogenic Mechanism of P. falciparum: Cytoadherence
- Schizonts express PfEMP1 (P. falciparum erythrocyte membrane protein 1) on knob-like extensions of the RBC surface
- PfEMP1 binds endothelial adhesion molecules: ICAM-1, VCAM-1, CD36
- This causes sequestration of infected RBCs in deep capillary beds (brain, kidney, placenta), which is the key mechanism of severe disease
- Normally, RBCs bear negatively charged surfaces that repel endothelium; PfEMP1 overcomes this barrier
Mosquito Stage (Sexual Cycle)
- Male gametocyte exflagellates in the mosquito midgut
- Fusion with female gametocyte → zygote → ookinete (penetrates gut wall) → oocyst → releases sporozoites that migrate to salivary glands
4. Transmission Routes
- Mosquito bite (principal route) - infected female Anopheles, most active dusk to dawn
- Blood transfusion
- Needle sharing (injection drug use)
- Organ transplantation
- Congenital (maternal-fetal)
- "Airport malaria" - infected mosquito transported on aircraft, bites passengers/staff at destination without the disease establishing locally
- Rosen's Emergency Medicine, Ch. 122
5. Clinical Features
Incubation Period
- P. falciparum: 7-14 days (range 7-30 days; rarely up to 1 year if partial prophylaxis)
- P. vivax/P. ovale: 8-30 days (hypnozoite relapses months to years later)
- P. malariae: 15-30+ days (recrudescence decades later possible)
- P. knowlesi: 9-12 days
Prodrome
Malaise, headache, fatigue, myalgia, anorexia, nausea - may mimic influenza
The Classic Malarial Paroxysm (Febrile Cycle)
Corresponds to synchronous RBC lysis and merozoite release:
| Phase | Description | Duration |
|---|---|---|
| Cold stage | Sudden chills, rigors, teeth chattering | 15-60 min |
| Hot stage | High fever (39-41°C), headache, vomiting, seizures in children | 2-6 h |
| Sweating stage | Profuse diaphoresis, temperature falls, exhaustion | 2-4 h |
Note: Classic periodicity is often absent early in the illness, especially in non-immune travelers. Fever may be continuous or irregular initially.
Uncomplicated Malaria
- Fever (universal), headache, myalgia, arthralgia, nausea, vomiting, diarrhea
- Splenomegaly (common with repeated infections)
- Mild anemia
- Jaundice (mild)
Severe/Complicated Falciparum Malaria (WHO Criteria)
Cerebral malaria (most feared)
- Unarousable coma (Blantyre Coma Score < 3 in children; GCS < 11 in adults), seizures
- Pathology: sequestration of parasitized RBCs in cerebral microcirculation, ring hemorrhages, Dürck's granulomas
- Mortality 15-20% even with treatment
Severe anemia - Hgb < 5 g/dL or Hct < 15%; more common in children and pregnant women
Acute respiratory distress - Non-cardiogenic pulmonary edema from capillary leak; more common in adults and pregnant women
Acute kidney injury - "Blackwater fever" (massive hemolysis → hemoglobinuria → acute tubular necrosis); more common in adults
Hypoglycemia - Especially in children, pregnant women, and those on quinine (stimulates insulin secretion)
Circulatory shock ("algid malaria") - Systolic BP < 70 mmHg; often associated with Gram-negative bacteremia
Abnormal bleeding - DIC, thrombocytopenia
Hyperparasitemia - > 5% parasitized RBCs (> 2% in non-immune patients)
Relative incidence of severe complications:
| Complication | Non-pregnant Adults | Pregnant Women | Children |
|---|---|---|---|
| Anemia | + | ++ | +++ |
| Convulsions | + | + | +++ |
| Hypoglycemia | + | +++ | +++ |
| Jaundice | +++ | +++ | + |
| Renal failure | +++ | +++ | + |
| Pulmonary edema | ++ | +++ | + |
Malaria in Pregnancy
- Falciparum malaria: fetal loss, premature labor, low birth weight (~170 g reduction), maternal anemia
- Placental sequestration of infected RBCs (even in asymptomatic women)
- Maternal HIV co-infection worsens outcomes
- Unstable transmission areas: pregnant women prone to severe malaria with hypoglycemia, pulmonary edema
Malaria in Children
- Severe malarial anemia and cerebral malaria predominate
- Febrile convulsions common
- Hypoglycemia more frequent
- Splenomegaly, malnutrition from recurrent infections
6. Diagnosis
A. Peripheral Blood Smear (Gold Standard)
- Thick smear: detects parasites (concentration method, more sensitive, lower parasite density detectable)
- Thin smear: species identification, parasitemia quantification
- Repeat smears every 12-24 hours if initial smear is negative but suspicion remains high
Species differentiation on smear:
| Feature | P. falciparum | P. vivax | P. malariae | P. ovale |
|---|---|---|---|---|
| RBC size | Normal | Enlarged | Normal | Normal/slightly enlarged |
| Multiple rings/RBC | Common | Rare | Rare | Rare |
| Schüffner's dots | Absent | Present | Absent | Present |
| Ring form | Delicate, "appliqué" (accole) forms | Larger, amoeboid | "Band" forms | Compact |
| Gametocytes | Banana/crescent-shaped | Round | Round | Round |
| % parasitemia | Can be very high (>10%) | Usually <1% | Usually <1% | Usually <1% |
B. Rapid Diagnostic Tests (RDTs)
- Detect malaria antigens (HRP-2 for P. falciparum, pLDH or aldolase for other species)
- Sensitivity 95%+ for P. falciparum at >100 parasites/μL
- Results in 15-20 minutes
- Limited by: false negatives at low parasitemia, HRP-2 gene deletions (P. falciparum), inability to quantify
- Positive HRP-2 may persist for weeks after treatment (not useful for treatment response)
C. PCR
- Most sensitive (can detect submicroscopic parasitemia)
- Best for species confirmation, drug resistance genotyping
- Not for emergency diagnosis due to turnaround time
D. Laboratory Findings (Non-specific but Supportive)
- Thrombocytopenia (very common, often < 150,000; <50,000 in severe disease)
- Elevated LDH, bilirubin (hemolysis)
- Low haptoglobin
- Normocytic anemia
- Elevated creatinine (renal involvement)
- Hypoglycemia
- Elevated inflammatory markers (CRP, PCT) - but non-specific
7. Treatment
Uncomplicated Malaria
Uncomplicated P. falciparum (or unknown species in endemic area):
First-line: Artemisinin-based Combination Therapy (ACT)
- Artemether-lumefantrine (most widely used; 6-dose regimen over 3 days with fatty food)
- Artesunate-amodiaquine
- Artesunate-mefloquine
- Dihydroartemisinin-piperaquine
- Atovaquone-proguanil (20/8 mg/kg/day x 3 days with food) - preferred for travelers
Chloroquine-sensitive P. falciparum (very few areas remain): Chloroquine 25 mg base/kg over 3 days
Uncomplicated P. vivax / P. ovale:
- Chloroquine (if sensitive) OR ACT PLUS
- Primaquine (0.25-0.5 mg base/kg/day x 14 days) to eliminate hypnozoites and prevent relapse
- MUST screen for G6PD deficiency before primaquine (causes severe hemolysis in G6PD-deficient patients)
- Tafenoquine (single dose alternative to primaquine, also requires G6PD screening)
P. malariae: Chloroquine (no primaquine needed - no hypnozoites)
Severe/Complicated Falciparum Malaria (Medical Emergency)
Drug of choice: IV Artesunate (FDA-approved for severe malaria in the US)
- 12.4 mg/kg IV stat, then 2.4 mg/kg at 12 h and 24 h, then daily if needed
- Children < 20 kg: 3 mg/kg per dose
- 35% lower mortality vs. quinine in Southeast Asia; 22.5% lower in Africa
Alternative if artesunate unavailable:
- Artemether 3.2 mg/kg IM stat, then 1.6 mg/kg/day IM (erratic absorption)
- Quinine dihydrochloride 20 mg salt/kg over 4 h, then 10 mg salt/kg over 2-8 h every 8 h (monitor for QTc prolongation, hypoglycemia)
Artemisinin resistance (Southeast Asia): Artesunate + quinine together at full doses
Adjunctive management of severe malaria:
- Continuous blood glucose monitoring (especially with quinine)
- IV dextrose for hypoglycemia
- Anti-convulsants (IV diazepam for seizures; prophylactic phenobarbital not recommended)
- Careful fluid management (avoid fluid overload causing pulmonary edema)
- Renal replacement therapy for AKI
- Exchange transfusion (controversial; may be considered for > 10% parasitemia)
- NOT recommended: High-dose glucocorticoids, heparin, dextran, desferrioxamine (shown to be harmful or ineffective)
- ICU care and frequent reassessment
Transmission Blocking
A single low dose of primaquine (0.25 mg base/kg) is added to falciparum treatment in low-transmission areas to kill gametocytes and prevent onward transmission. This is safe even in G6PD deficiency at this dose.
8. Chemoprophylaxis
| Drug | Regimen | Notes |
|---|---|---|
| Atovaquone-proguanil | 1 tablet daily (start 1-2 days before, stop 7 days after travel) | Well tolerated; GI side effects |
| Doxycycline | 100 mg daily (start 1-2 days before, stop 4 weeks after) | Photosensitivity; contraindicated in pregnancy/children < 8 yr |
| Mefloquine | Weekly (start 2 weeks before, stop 4 weeks after) | Neuropsychiatric side effects; can use in pregnancy |
| Chloroquine | Weekly (only in sensitive areas) | Increasingly limited use |
| Primaquine | Daily (terminal prophylaxis for P. vivax) | Requires G6PD testing |
9. Differential Diagnosis
The key challenge: any febrile illness in a traveler returning from or resident in a tropical area must have malaria excluded first, as untreated falciparum malaria can be fatal within 24-48 hours.
Primary Differential Diagnoses
| Condition | Key Distinguishing Features |
|---|---|
| Typhoid fever (Salmonella typhi) | Relative bradycardia, rose spots, step-ladder fever pattern, prominent abdominal symptoms, positive blood/stool culture; splenomegaly without anemia; no parasites on smear |
| Dengue fever | Abrupt onset high fever, severe myalgia/arthralgia ("breakbone fever"), retro-orbital pain, rash (maculopapular, petechiae), marked thrombocytopenia and leukopenia, positive NS1 antigen/serology; no parasites |
| Leptospirosis | Weil's disease triad: jaundice, renal failure, hemorrhage; conjunctival suffusion (pathognomonic), history of freshwater/animal exposure, elevated CK; serology/PCR confirm |
| Viral hepatitis | Predominant jaundice and transaminase elevation, usually without cyclic fever pattern, dark urine/pale stool, hepatitis serology |
| Sepsis/Bacteremia | No specific geographic risk, positive blood cultures, often identifiable source (cellulitis, pneumonia, UTI); may co-occur with malaria |
| Typhus (Rickettsia) | Eschar at bite site, macular rash spreading centripetally, louse/tick/flea exposure; serology (Weil-Felix) |
| Influenza / COVID-19 | Respiratory predominance, no parasitemia, rapid antigen tests positive |
| Meningitis / Encephalitis | Meningeal signs (neck stiffness, Kernig's, Brudzinski's); CSF analysis differentiates from cerebral malaria - CSF in cerebral malaria is usually clear with normal/mildly elevated protein |
| Visceral leishmaniasis (Kala-azar) | Months of progressive fever, massive splenomegaly, pancytopenia, hypergammaglobulinemia; bone marrow/splenic aspirate shows amastigotes |
| African trypanosomiasis | Trypanosomal chancre, progressive neurological decline, sleep disturbance; blood smear shows trypomastigotes |
| Schistosomiasis (Katayama syndrome) | 4-8 weeks after freshwater exposure, urticarial rash, eosinophilia, positive serology |
| Melioidosis (Burkholderia pseudomallei) | Southeast Asia, N. Australia; pneumonia with abscess formation; culture confirms |
| Yellow fever | Jaundice + hemorrhage + renal failure; vaccination history; yellow fever belt Africa/S. America |
Key Differentiating Points
- Malaria: no eosinophilia (eosinophilia points to helminth infection)
- Malaria: thrombocytopenia is very common but non-specific
- Malaria: smear or RDT is diagnostic - always perform in febrile traveler
- In endemic areas: incidental parasitemia can coexist with another infection (especially in children) - treat for both if in doubt
- P. falciparum malaria in non-immune traveler: do not wait for classic periodicity - it may never appear before the patient deteriorates
10. Complications at a Glance
| Complication | Mechanism |
|---|---|
| Cerebral malaria | Sequestration in cerebral vessels, inflammatory cytokines (TNF-α, IL-1), BBB disruption |
| Severe anemia | RBC destruction (hemolysis), dyserythropoiesis, bone marrow suppression, splenic sequestration |
| Acute kidney injury / Blackwater fever | Massive hemolysis → hemoglobinuria → ATN; microvascular obstruction in renal vessels |
| Hypoglycemia | Parasite glucose consumption; quinine-induced hyperinsulinemia; cytokine-mediated gluconeogenesis inhibition |
| Pulmonary edema (ARDS) | Capillary sequestration, cytokine storm, increased vascular permeability |
| Nephrotic syndrome | P. malariae causes immune complex glomerulonephritis (quartan nephropathy) |
| DIC | Thrombocytopenia, consumption coagulopathy |
| Splenomegaly/rupture | Hyperreactive malarial splenomegaly in chronic infection |
11. Special Populations
- Pregnancy: Falciparum associated with placental sequestration, low birth weight, maternal mortality. ACT (except artesunate monotherapy in 1st trimester) + IPTp (intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine) recommended by WHO.
- Asplenic patients: Higher risk of severe disease; extra vigilance for prophylaxis.
- Sickle cell trait: Partial protection against severe falciparum malaria (selective pressure underlying HbS prevalence in endemic areas).
- G6PD deficiency: Primaquine and tafenoquine are absolutely contraindicated in severe G6PD deficiency; screening mandatory.
12. Prevention
- Insecticide-treated bed nets (ITNs) - single most effective intervention
- Indoor residual spraying (IRS)
- Chemoprophylaxis for travelers (see table above)
- RTS,S/AS01 (Mosquirix) and R21/Matrix-M - approved malaria vaccines; primarily for children in Africa; 30-75% efficacy against clinical malaria
- Larval source management, environmental control
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 231 - Malaria
- Robbins & Kumar Basic Pathology, Ch. 10 - pp. 392-394
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Ch. 122
- Goldman-Cecil Medicine, Ch. 316
- Brenner & Rector's The Kidney (renal complications)
Explain me typhoid from basics to clinical but in simplified language and easy version explain everything
Reading File
Finding Sources
Searching PubMed
"typhoid fever"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have everything. Here is the full, simplified, easy-to-understand guide to typhoid fever.
🌡️ Typhoid Fever - From Basics to Clinical (Simple Version)
1. What Is Typhoid? (The Simple Story)
Think of typhoid like this: a nasty bacteria gets into your food or water, you swallow it, it sneaks past your stomach, enters your gut, gets into your blood, and then causes a serious infection that lasts weeks.
It is NOT just a stomach bug. Typhoid is a whole-body (systemic) infection that can be fatal if not treated.
Its real name is Enteric Fever (enteric = related to the gut). But "typhoid fever" is the name everyone uses.
2. The Culprit: What Causes It?
The germ is a bacteria called Salmonella Typhi (also written S. typhi).
A milder version is caused by Salmonella Paratyphi (A, B, or C) - this gives a similar but less severe illness called paratyphoid fever.
Important fact: Only humans carry this bacteria. There is no animal reservoir. So the infection comes from another infected person - directly or via contaminated food/water.
3. How Does It Spread? (Simple Chain of Infection)
Infected person's poop/urine
↓
Contaminates water or food
↓
You eat or drink it
↓
Bacteria enter your body
↓
You get sick (and can then spread it too)
Common ways it spreads:
- Drinking unclean water or water mixed with sewage
- Eating street food or unwashed fruits/vegetables
- Ice made from contaminated water
- Food handled by someone who is infected (even if they look healthy)
- Chronic carriers - people who recovered from typhoid but still carry the bacteria silently in their gallbladder and pass it in their stool for years
Who is at risk?
- People living in or traveling to South Asia (India, Pakistan, Bangladesh, Nepal), Southeast Asia, Africa, and Latin America
- Young children and teenagers in endemic areas
- Anyone drinking unclean water
Fun/scary fact: A famous example is "Typhoid Mary" - a cook in early 1900s New York who had no symptoms herself but infected dozens of families by cooking for them. She was a chronic carrier.
4. How Does It Enter and Spread in the Body? (The Journey of the Bacteria)
Let's trace what happens after you swallow the bacteria, step by step:
Step 1 - Swallowed
You swallow S. typhi in food or water. Most bacteria are killed by stomach acid. But if you swallowed a large enough dose, some survive.
Step 2 - Gut Wall Entry
The bacteria reach the small intestine (specifically the terminal ileum). There, they sneak through special cells called M cells that normally sample what's in the gut. From here, the bacteria are engulfed by immune cells (macrophages) in the gut wall.
Step 3 - Lymph Nodes (The "First Base")
The bacteria travel to lymph nodes in the gut called Peyer's patches and mesenteric lymph nodes. Here they multiply inside macrophages. This is the incubation period (no symptoms yet).
Step 4 - Into the Blood (Bacteremia)
After multiplying in the lymph nodes, bacteria spill into the bloodstream. This is when fever starts. This "first bacteremia" is brief and often goes unnoticed.
Step 5 - Organs Get Infected
The bacteria then travel via blood to the liver, spleen, bone marrow, and gallbladder, where they multiply again massively. Tiny foci of infected cells called "typhoid nodules" form in the liver, spleen, and bone marrow.
Step 6 - Second Bacteremia = Full Illness
The bacteria re-enter the blood in large numbers. This produces the full clinical picture of typhoid: prolonged high fever, feeling terrible, abdominal symptoms.
Step 7 - Back to the Gut (The Dangerous Bit)
Bacteria from the gallbladder drain back into the intestine, causing re-infection of Peyer's patches. These lymphoid patches swell, ulcerate, and can perforate - the most feared complication.
5. What Happens in the Body (Pathology)
| Location | What Happens |
|---|---|
| Peyer's patches (ileum) | Enlarge like plateaus (up to 8 cm), then ulcerate - oval ulcers along the length of the intestine |
| Mesenteric lymph nodes | Swell and become inflamed |
| Liver | Typhoid nodules (tiny clusters of macrophages), mild hepatitis |
| Spleen | Enlarges (splenomegaly) - red pulp expands |
| Bone marrow | Macrophage proliferation - leads to anemia, low WBC |
| Gallbladder | Bacteria colonize, especially if there are gallstones; carrier state |
6. Timeline of the Illness (Week by Week)
This is the classic step-ladder fever pattern. Think of it as the disease unfolding over 4 weeks like a story.
Incubation Period (Days 1-14, no symptoms)
- Average 10-14 days from swallowing the bacteria to feeling sick
- Can range from 5 to 21 days depending on how much bacteria you swallowed and your immunity
🗓️ Week 1 - "Something is Wrong"
- Fever starts low and rises step by step each day (step-ladder pattern)
- Headache (very common, ~80% of patients)
- Dry cough (~30%)
- Body aches, tiredness, feeling generally unwell
- Constipation more common than diarrhea early on
- The patient doesn't look very sick yet - easily mistaken for flu
🗓️ Week 2 - "Full Blown Illness"
- High fever (39-40.5°C / 103-105°F) - continuous, not going up and down like malaria
- Relative bradycardia - the heart rate is lower than expected for such a high fever (normally fever raises heart rate, but in typhoid the bacteria slow it)
- Rose spots appear on the trunk and chest
Rose spots: faint, salmon-colored, blanching spots on the trunk - appear in ~30% of patients in the 2nd week. They disappear in 2-5 days. (Harrison's, 22E)
- Coated tongue (white fur on the tongue)
- Distended, tender abdomen
- Spleen and sometimes liver become enlarged (hepatosplenomegaly)
- Patient looks toxic and very unwell
- Diarrhea may develop ("pea soup" diarrhea - loose, greenish)
🗓️ Week 3 - "The Danger Zone" ⚠️
- High fever continues
- Complications start appearing:
- Intestinal perforation (ulcers burst through the gut wall) - sudden severe abdominal pain, board-like abdomen, peritonitis
- Intestinal bleeding - blood in stool
- Patient may become confused, drowsy ("muttering delirium")
- Most deaths occur in this week if untreated
🗓️ Week 4 - Recovery (if treated) or Deterioration (if not)
- With treatment: fever comes down, patient improves
- Without treatment: fever gradually settles but patient is very weak
- Relapses can occur in 5-10% of patients even after antibiotics
- Untreated typhoid has 10-20% mortality (mostly in young children)
7. Symptoms Summary Table
| Symptom | How Common | Notes |
|---|---|---|
| Fever | >75% | Prolonged, continuous, up to 4 weeks if untreated |
| Headache | ~80% | Often severe |
| Anorexia (no appetite) | ~55% | Very common |
| Abdominal pain | 30-40% | Not always present! |
| Cough | ~30% | Dry cough |
| Diarrhea | 22-28% | NOT always present; can have constipation instead |
| Constipation | 13-16% | More common early in illness |
| Nausea/vomiting | 18-24% | |
| Rose spots | ~30% | Faint - easily missed, especially on dark skin |
| Relative bradycardia | <50% | Classic but often absent |
| Splenomegaly | 5-6% | More common with longer illness |
| Coated tongue | 51-56% | White fur |
Key teaching point: Typhoid is a great "masquerader." It doesn't always present classically. Many patients have no abdominal pain, no rose spots, and no bradycardia. The only constant feature is prolonged fever with a history from an endemic area.
8. Complications (When Things Go Wrong)
Complications occur in about 27% of hospitalized patients, especially if diagnosis is delayed.
Dangerous (Life-threatening) Complications
| Complication | What Is It? | When? |
|---|---|---|
| Intestinal perforation (1%) | Ulcerated Peyer's patches burst through the gut - peritonitis | Week 3-4 |
| Intestinal bleeding (6%) | Ulcers bleed - can be severe | Week 3-4 |
| Typhoid encephalopathy | Confusion, delirium, even coma | Any week |
| Myocarditis | Heart muscle inflammation | Week 2-3 |
| DIC (rare) | Blood clotting system goes haywire | Severe cases |
Other Complications
- Meningitis, Guillain-Barre syndrome (nerve damage)
- Pneumonia
- Hepatitis (liver inflammation)
- Cholecystitis (gallbladder infection)
- Pancreatitis
- Hemolytic anemia
- Hemophagocytic syndrome (HLH) - rare but life-threatening (macrophages start destroying blood cells)
The Carrier State
- After recovery, 1-5% of patients become chronic carriers
- Bacteria live silently in the gallbladder (especially if gallstones present)
- They shed bacteria in stool for years with no symptoms
- This is a major source of ongoing transmission in the community
9. Diagnosis (How Do Doctors Confirm It?)
A. Blood Culture - The Best Test 🥇
- Most reliable: Positive in 80-90% of patients during the first week of fever
- You take blood and grow the bacteria in a lab
- Takes 3-5 days for results
- Sensitivity drops after antibiotics are started
B. Bone Marrow Culture - The Most Sensitive 🥇🥇
- Can still be positive even after antibiotics have been started
- But it's invasive (needle into the bone) - reserved for cases where blood culture is negative but suspicion is high
C. Stool and Urine Culture
- Stool culture becomes positive in week 2-3 (when bacteria re-enter the gut via bile)
- Less sensitive than blood culture
D. Widal Test (The Old Test - Controversial)
- Blood test that looks for antibodies against S. typhi (H and O antigens)
- Problems:
- Takes 7-10 days to turn positive (antibodies take time to develop)
- Many false positives (can be positive from past infection, other Salmonella, or even vaccination)
- Many false negatives early in disease
- Not reliable alone - needs to be combined with clinical picture
- Still widely used in low-resource settings because it's cheap
- A rising titre (4-fold rise in paired samples) is more meaningful than a single reading
E. Typhidot / Rapid Antigen Tests
- Detect IgM and IgG against S. typhi
- Faster and more specific than Widal
- Increasingly available in endemic countries
F. PCR
- Very sensitive and specific
- Not widely available in most endemic areas
Typical Lab Findings (Non-specific but helpful)
| Finding | What You See |
|---|---|
| White blood cells (WBC) | Low (leukopenia) - unusual for a bacterial infection! |
| Platelets | Often low |
| Liver enzymes (SGOT/SGPT) | Mildly elevated |
| Anemia | Often present |
| ESR/CRP | Elevated |
Memory trick: Most bacterial infections raise the WBC. Typhoid lowers it. If you see a patient with prolonged fever, travel history, and low WBC - think typhoid!
10. Treatment (How Do You Treat It?)
First-line Antibiotics
| Drug | How Given | Notes |
|---|---|---|
| Ceftriaxone (3rd gen cephalosporin) | IV, 1-2 g/day x 10-14 days | Best for severe/hospitalized cases |
| Azithromycin | Oral, 500 mg/day x 7 days | Good for uncomplicated typhoid; works against many resistant strains |
| Ciprofloxacin | Oral or IV | Resistance rising rapidly - especially from South/Southeast Asia; use only if susceptibility confirmed |
Drugs That No Longer Work Well (Due to Resistance)
- Chloramphenicol - was first-line for decades, now MDR strains resist it
- Ampicillin
- Co-trimoxazole (trimethoprim-sulfamethoxazole)
Drug-resistant Typhoid - A Growing Crisis
- MDR (Multi-Drug Resistant) = Resistant to chloramphenicol + ampicillin + co-trimoxazole
- XDR (Extensively Drug Resistant) = Also resistant to fluoroquinolones AND 3rd gen cephalosporins
- XDR typhoid emerged in Pakistan (Sindh province) in 2016 and is spreading
- XDR is treated with azithromycin or carbapenems (last resort)
For Severe Typhoid (Shock, Encephalopathy, High Fever)
- Add dexamethasone (steroid) - reduces inflammation and mortality in very severe cases
- IV fluids for rehydration
- Blood transfusion if anemia is severe
- Surgery if intestinal perforation occurs (emergency bowel repair + peritonitis washout)
Follow-up
- Relapses occur in 5-10% - treat again with same antibiotic (bacteria usually remain sensitive)
- Check stool cultures after treatment to confirm clearance
- Chronic carriers: prolonged antibiotics (ciprofloxacin x 4 weeks) can eliminate carriage in many; cholecystectomy (gallbladder removal) if antibiotics fail
11. Differential Diagnosis (What Else Can Look Like Typhoid?)
Because typhoid has vague symptoms, many illnesses can mimic it. The key question is always: "Prolonged fever in someone from/traveling to an endemic area - what else could this be?"
| Disease | How to Tell It Apart |
|---|---|
| Malaria | Cyclical fever (not continuous), chills and rigors, positive blood smear or RDT for malaria parasite; WBC often normal |
| Dengue fever | Sudden onset, severe bone pain, rash with petechiae, marked thrombocytopenia + leukopenia, positive NS1 antigen test; fever lasts only 5-7 days |
| Viral hepatitis | Jaundice predominant, very high liver enzymes (>10x normal), positive hepatitis serology; less fever |
| Tuberculosis (miliary) | Longer history (weeks to months), night sweats, weight loss, CXR abnormalities, positive TB tests |
| Infective endocarditis | Heart murmur, embolic phenomena, positive blood cultures (different organisms), echo shows vegetations |
| Leptospirosis | Freshwater/animal contact, conjunctival redness (suffusion), muscle pain especially calves, jaundice + renal failure (Weil's disease) |
| Brucellosis | Contact with animals/unpasteurized dairy, undulant fever (rises and falls), joint pain, positive brucella serology |
| Amoebic liver abscess | Right upper quadrant pain and tenderness, elevated right hemidiaphragm on CXR, ultrasound shows liver abscess |
| Rickettsial disease (Scrub typhus) | Eschar at tick/mite bite site (pathognomonic), rash, forest/scrub exposure, responds to doxycycline |
| Visceral leishmaniasis (Kala-azar) | Months of fever, massive splenomegaly, marked weight loss, darkening of skin, pancytopenia |
| COVID-19 / Influenza | Respiratory symptoms dominant, rapid antigen/PCR tests confirm |
Quick Clinical Clue Table
| Clue | Think Of |
|---|---|
| Fever + relative bradycardia + rose spots + coated tongue | Typhoid |
| Fever + rigors + blood smear positive | Malaria |
| Fever + retro-orbital pain + rash + leukopenia | Dengue |
| Fever + eschar at bite site | Scrub typhus |
| Fever + jaundice + muscle pain + red eyes | Leptospirosis |
| Fever + undulant pattern + joint pain + animal contact | Brucellosis |
12. Prevention (How to Stop It?)
Personal Hygiene (Most Important!)
- "Boil it, cook it, peel it, or forget it" - the traveler's rule
- Drink only boiled or bottled water
- Avoid ice made from tap water
- Avoid street food and raw vegetables in endemic areas
- Wash hands thoroughly after toileting and before eating
Vaccination
Two typhoid vaccines are available:
| Vaccine | Type | How Given | Duration |
|---|---|---|---|
| Ty21a (Vivotif) | Live oral vaccine | 4 capsules on alternate days | ~5 years |
| Vi polysaccharide (Typhim Vi) | Injected | Single shot | ~3 years |
| Typhoid Conjugate Vaccine (TCV - Typbar-TCV) | Injected | Single shot | Longer (conjugate = better memory) |
- TCV is now recommended by WHO for children in endemic areas (given from 6 months of age)
- Neither vaccine is 100% protective - good hygiene is still essential
Public Health Measures
- Clean water supply and sewage treatment - the single biggest prevention
- Identifying and treating chronic carriers (especially food handlers)
- Proper food hygiene and inspection
13. Quick Summary Card
TYPHOID IN A NUTSHELL
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Caused by: Salmonella Typhi (bacteria)
How spread: Contaminated food/water (feco-oral route)
Incubation: 10-14 days (range 5-21)
Key symptoms: Prolonged fever + headache + coated tongue
Classic signs: Relative bradycardia + rose spots + splenomegaly
Labs: Leukopenia (LOW white cells!) + mild liver enzymes↑
Diagnosis: Blood culture (gold standard)
Danger: Gut perforation in week 3-4
Treatment: Ceftriaxone (IV) or Azithromycin (oral)
Prevention: Clean water + hand hygiene + vaccination
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 171 - Enteric (Typhoid) Fever
- Robbins & Kumar Basic Pathology - Ch. 13
- Tintinalli's Emergency Medicine, Ch. 162
- Park's Textbook of Preventive and Social Medicine
Explain me dengue from basics to clinical
Finding Sources
Searching PubMed
"dengue"[MeSH Terms] AND "clinical features"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the data I need from multiple authoritative textbooks. Let me write the comprehensive, simplified dengue guide.
🦟 Dengue Fever - From Basics to Clinical (Simple Version)
1. What Is Dengue? (The Big Picture)
Dengue is a viral infection spread by mosquito bites. It is one of the most common and fastest-spreading tropical diseases in the world - the WHO reports a 30-fold increase in cases over the last 30 years.
Here is the short version: a mosquito bites you, injects a virus, your immune system fights it hard, and that fight causes fever, severe body pain, and sometimes dangerous bleeding and shock.
About 400 million people are infected every year. Of these, around 100 million get sick with symptoms, and about 40,000 die - mostly from the severe form of dengue.
2. The Culprit: What Causes Dengue?
Dengue is caused by the Dengue Virus - a type of Flavivirus (same family as Zika, Yellow Fever, and Japanese Encephalitis).
There are 4 types (serotypes): DEN-1, DEN-2, DEN-3, and DEN-4.
This is the key thing to understand:
🔑 Getting infected with one type gives you lifelong protection only against that type. You can get dengue up to 4 times in your lifetime - once with each serotype. And the second infection is often MORE severe than the first.
3. How Does It Spread? (The Transmission Story)
The Main Route: Mosquito Bite
Infected person's blood
↓
Mosquito (Aedes aegypti) bites and sucks infected blood
↓
Virus multiplies inside the mosquito (takes ~8-12 days)
↓
Infected mosquito bites another person
↓
You get dengue
The mosquito villain: Aedes aegypti
- Smaller than a regular mosquito
- Has distinctive white stripes on black body and legs
- Bites during the day (especially morning and late afternoon) - unlike malaria mosquitoes that bite at night
- Breeds in small collections of clean, stagnant water - flower pots, tyres, water tanks, bottle caps, even the base of a toilet
- Lives close to humans - a domestic mosquito
- Aedes albopictus (tiger mosquito) can also transmit dengue but is less efficient
Other (Rare) Routes
- Vertical transmission (mother to baby during pregnancy/delivery) - ~20% risk
- Blood transfusion or organ donation
- Breastfeeding (rare)
- Needlestick injury in healthcare settings
Where does it occur?
Dengue is found across tropical and subtropical regions: South Asia, Southeast Asia, Pacific Islands, Latin America, Caribbean, Africa. Local outbreaks have also occurred in southern USA, France, Italy, and Spain.
4. How the Virus Makes You Sick (Pathogenesis)
Step 1 - The Mosquito Injects the Virus
When the mosquito bites, dengue virus enters your skin. Dendritic cells and macrophages (your immune system's scouts) in the skin pick up the virus.
Step 2 - Virus Spreads to Lymph Nodes
The infected immune cells carry the virus to nearby lymph nodes, where it multiplies.
Step 3 - Virus Gets Into the Blood (Viremia)
After multiplying, virus enters the bloodstream - this is called viremia. This is when fever starts. Viremia peaks in the first 3-5 days of illness.
Step 4 - Your Immune System Launches a War
Your body detects the virus and releases massive amounts of chemical signals called cytokines (especially TNF-α, IL-6, IL-8). This "cytokine storm" causes:
- High fever
- Severe muscle and bone pain
- Headache
Step 5 (In Severe Dengue) - The Vessels Start Leaking
In severe dengue (DHF), the immune response damages blood vessel walls, making them leaky like a sieve. Plasma (fluid from blood) leaks out of vessels into surrounding tissues. This causes:
- Rising hematocrit (blood gets thicker as fluid leaks out)
- Swelling in the belly (ascites) and chest (pleural effusion)
- Shock if enough fluid leaks out
Why Does the 2nd Infection Cause Worse Disease? - Antibody-Dependent Enhancement (ADE)
This is one of the most important concepts in dengue:
When you had your first dengue infection, your body made antibodies against that serotype. When you get infected with a different serotype, those old antibodies try to fight but can't neutralize the new virus. Instead, they grab onto the virus and carry it directly into macrophages via Fc receptors - like a Trojan Horse. This makes the infection worse, causing more viral replication and more severe inflammation. This is called Antibody-Dependent Enhancement (ADE).
This is also why babies born to dengue-immune mothers can get severe dengue - the maternal antibodies do the same thing.
5. Classification of Dengue (The WHO System)
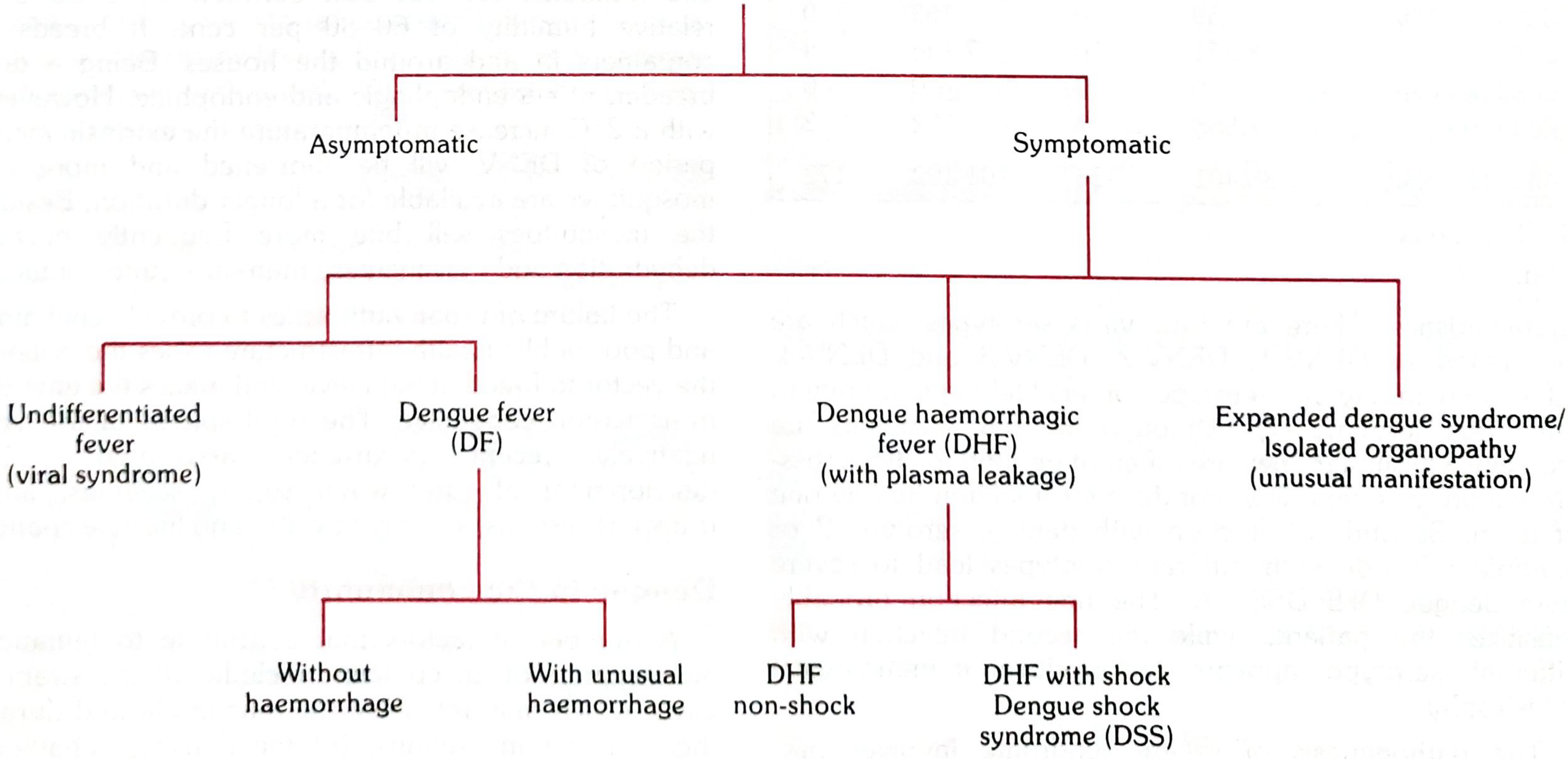
Classification of dengue virus infection manifestations (Park's Textbook of Preventive and Social Medicine)
The 2009 WHO Classification (Most Used Today):
1. Dengue Without Warning Signs - mild, manageable at home
2. Dengue With Warning Signs - needs hospital admission and monitoring
3. Severe Dengue - life-threatening, needs ICU-level care
6. The Three Phases of Dengue - The Story of the Illness
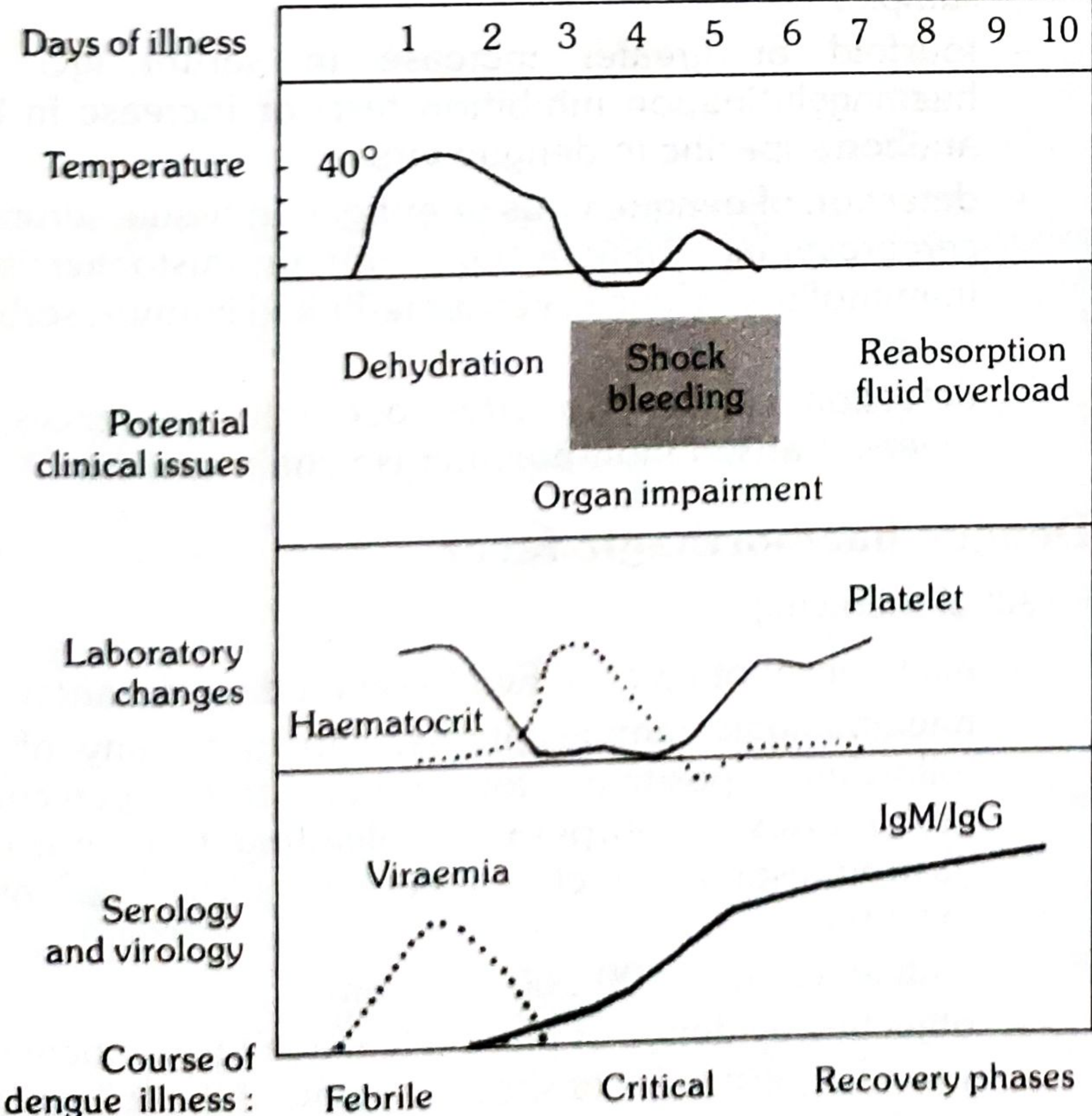
Course of dengue illness showing the 3 phases - notice how platelet drops and hematocrit rises during the critical phase (Park's Textbook)
🔴 Phase 1 - FEBRILE PHASE (Days 1-3)
What's happening: The virus is multiplying in your blood. Your immune system is fighting hard.
Symptoms:
- Sudden high fever (39-40°C / 102-104°F) - starts abruptly, like someone switched a switch
- Severe headache - especially behind the eyes (retro-orbital pain - pain when you move your eyes or press on them)
- Severe muscle, joint, and bone pain - so bad the old name was "Breakbone Fever" - patients feel like their bones are breaking
- Facial flushing - face looks red and flushed
- Nausea, vomiting, loss of appetite
- Mild rash (flushing of face, neck, chest - not the classic rash yet)
- Sore throat, injected (red) throat
In the lab:
- Leukopenia (WHITE BLOOD CELLS FALL) - very characteristic, starts early
- Platelets begin to drop
🧠 Easy way to remember: Dengue = "FETCH" - Fever sudden, Eyes hurt (retro-orbital), Throbbing bones (breakbone), Check blood (low WBC), High temperature fast
⚠️ Phase 2 - CRITICAL PHASE (Days 3-7, around defervescence)
What's happening: The fever begins to drop (defervescence) - but DON'T be fooled! This is the most dangerous phase. The virus is clearing, but the immune damage to blood vessels is at its peak.
The Big Danger: Plasma Leakage
- Blood vessel walls become leaky
- Fluid (plasma) leaks from vessels into tissues
- This phase lasts only 24-48 hours but can be lethal
Warning Signs (signals the patient is entering danger - needs hospitalization NOW):
- ⚡ Severe abdominal pain or tenderness
- ⚡ Persistent vomiting (≥3 times in 24 hours)
- ⚡ Sudden bleeding from nose, gums, or skin (mucosal bleeding)
- ⚡ Blood in vomit or stool
- ⚡ Swelling of belly or fluid around lungs
- ⚡ Lethargy, restlessness, or sudden irritability
- ⚡ Liver enlargement >2 cm
- ⚡ Rapid decrease in platelet count alongside rising hematocrit
Lab findings in this phase:
- Platelets crash (can go below 20,000 - normal is 150,000-400,000!)
- Hematocrit rises by ≥20% (blood is concentrating as fluid leaks out)
- Liver enzymes (AST/ALT) go up
If plasma leakage is severe → Dengue Shock Syndrome (DSS):
- Cold, clammy extremities
- Rapid, weak pulse
- Narrowed pulse pressure (≤20 mmHg) - e.g., BP = 100/80 instead of 120/70
- Hypotension
- Decreased urine output
🔑 The paradox: The fever drops, the patient and family feel relieved - but this is actually the most dangerous moment. A patient who "improves" on day 4 can collapse into shock on day 5.
🟢 Phase 3 - RECOVERY PHASE (Days 7-10)
What's happening: The leaked plasma is reabsorbed back into the blood vessels. The body starts healing.
Signs of recovery:
- Fever gone, patient feels better
- Good urine output returns
- Appetite comes back
- Platelet count starts rising (recovery sign)
- Hematocrit falls as fluid returns to vessels
Danger in this phase: Fluid overload
- If the patient was given too much IV fluid during the critical phase, the fluid that returns to the vessels can cause pulmonary edema (fluid in the lungs) and breathing difficulty
- Bradycardia (slow heart rate) can occur
- A new rash may appear: the classic "white islands in a sea of red" - islands of normal skin surrounded by red flush
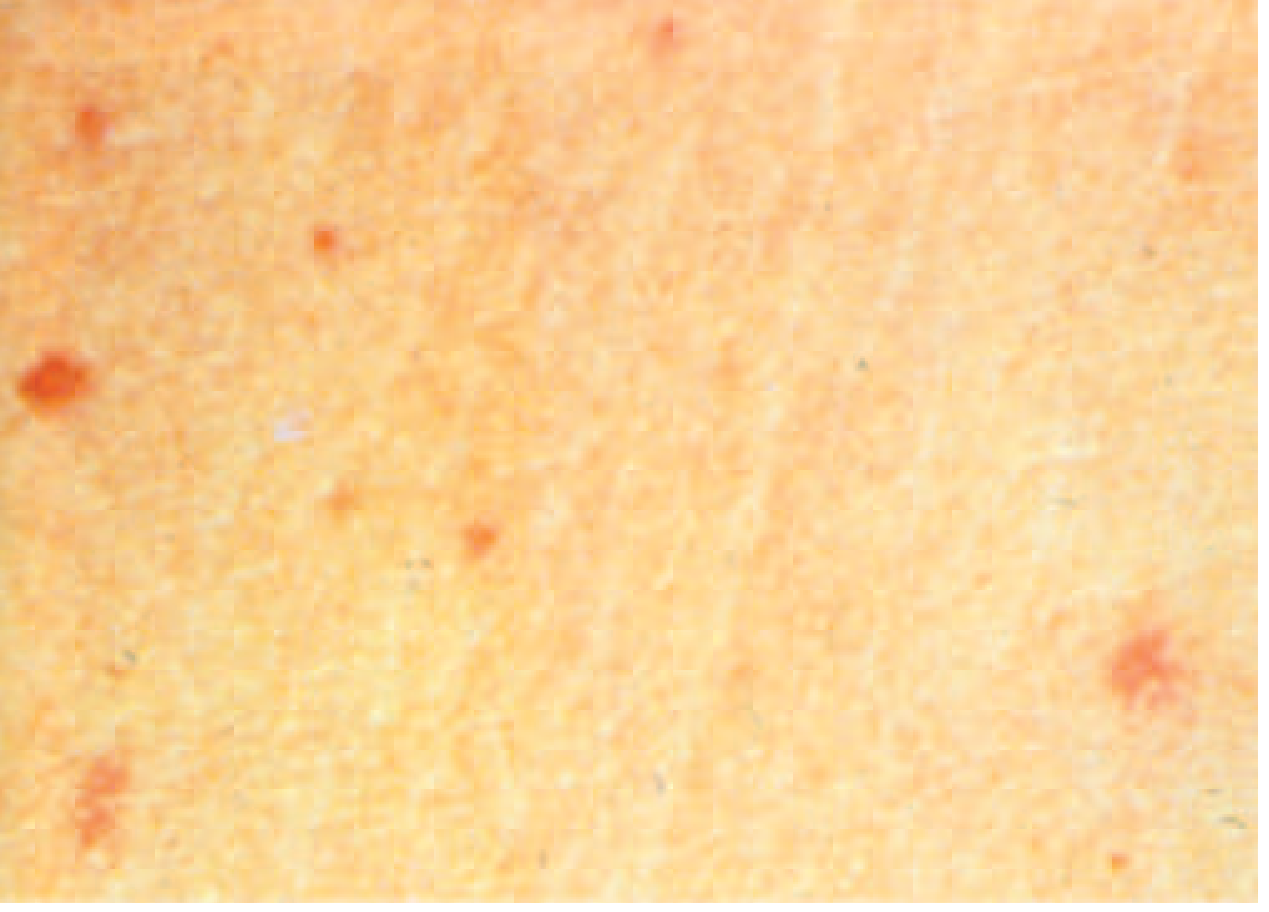
7. The Classic Dengue Rash
There are actually two different rashes in dengue:
| Rash | When | What it Looks Like |
|---|---|---|
| Early flush rash | Days 1-2 (febrile phase) | Diffuse redness of face, neck, chest - like sunburn |
| Late maculopapular rash | Days 3-5 (late febrile to recovery) | Red spots with islands of normal skin; starts trunk, spreads to arms and legs; may itch |
The late rash is described as "white islands in a sea of red" - it looks like red skin with pale circular patches within it. This is almost diagnostic of dengue.
8. Bleeding in Dengue
Dengue causes bleeding through several mechanisms:
- Thrombocytopenia - low platelets = poor clotting
- Vasculopathy - leaky damaged vessels allow red cells to escape
- DIC (Disseminated Intravascular Coagulation) - in severe cases, clotting factors are consumed
Types of bleeding from mild to severe:
- Petechiae (tiny red dots under skin from capillary bleeding)
- Easy bruising (ecchymoses)
- Nosebleeds (epistaxis)
- Bleeding gums
- Heavy periods in women (menorrhagia)
- Blood in vomit (hematemesis) or stool (melena)
- Internal bleeding (rare, severe)
Tourniquet Test (Rumple-Leede Test): A quick bedside test for dengue
- Inflate BP cuff to midpoint between systolic and diastolic for 5 minutes
- Positive: ≥10 petechiae per 2.5×2.5 cm area
- In DHF: usually ≥20 petechiae
- It shows the fragility of blood vessels
9. Severe Dengue (DHF/DSS) - The Dangerous Form
Who Gets Severe Dengue?
- People with second dengue infection (different serotype) - most common reason
- Infants of dengue-immune mothers (maternal ADE)
- Young children
- Patients infected with DEN-2 serotype (most virulent)
- People with certain genetic factors
Grades of DHF (Old WHO Classification)
| Grade | Features |
|---|---|
| Grade I | Fever + positive tourniquet test; no spontaneous bleeding |
| Grade II | Grade I + spontaneous bleeding (skin, nose, gums) |
| Grade III (DSS) | Grade II + circulatory failure (weak pulse, narrow pulse pressure) |
| Grade IV (DSS) | Profound shock - undetectable BP and pulse |
Severe Dengue (2009 WHO Classification) includes:
- Severe plasma leakage causing shock or fluid accumulation with breathing difficulty
- Severe bleeding (clinician-assessed)
- Severe organ involvement:
- Liver: AST or ALT ≥1000 IU/L
- Brain: altered consciousness, encephalitis
- Heart: myocarditis, arrhythmia
- Kidneys: acute kidney injury
10. Unusual/Expanded Dengue Manifestations
Beyond the classic picture, dengue can affect almost any organ:
| Organ | Complication |
|---|---|
| Brain | Encephalitis, meningitis, seizures, ADEM (post-dengue brain inflammation) |
| Heart | Myocarditis, arrhythmias, heart block |
| Liver | Hepatitis, liver failure |
| Kidneys | Acute kidney injury |
| Eyes | Uveitis, retinal hemorrhage |
| Pancreas | Pancreatitis |
| Blood | Hemophagocytic lymphohistiocytosis (HLH) - macrophages destroy blood cells |
These are called "expanded dengue syndrome" or "unusual dengue" and can occur even without plasma leakage.
11. Diagnosis (How Is Dengue Confirmed?)
Day-by-Day Testing Strategy
The right test depends on which day of fever you are on:
| Day of Illness | Best Test | Why |
|---|---|---|
| Day 1-5 (Febrile phase) | NS1 Antigen test | Virus is actively multiplying; NS1 is a viral protein released into blood |
| Day 1-5 | PCR (RT-PCR) | Most sensitive; detects viral RNA directly |
| Day 5+ (After fever drops) | IgM antibody test | Immune system has made antibodies by now |
| Primary vs. Secondary infection | IgM + IgG | IgM dominant in primary; IgG rises rapidly in secondary |
| Anytime (less specific) | Widal-like serology (HAI test) | Less specific, older method |
NS1 Antigen Test
- Detects the Non-Structural Protein 1 (NS1) of dengue virus
- Positive in first 5 days
- Quick result (15-30 minutes)
- Sensitivity ~80-90% in primary infection, slightly lower in secondary (ADE clears NS1 faster)
IgM/IgG ELISA
- IgM rises from day 5, peaks at 2 weeks
- IgG: low in primary infection; rises rapidly (within 1-2 days of fever) in secondary infection
- High IgG with low IgM = secondary dengue (higher risk of severe disease)
Important Lab Monitoring (Not Diagnostic But Essential)
| Test | What to Look For |
|---|---|
| CBC (Full blood count) | Serial platelet count + hematocrit trend |
| Hematocrit | Rising = plasma leakage occurring |
| Platelets | Falling rapidly = warning sign |
| Liver enzymes | Elevated in most cases |
| Albumin | Falls with plasma leakage |
| Chest X-ray / Ultrasound | Pleural effusion, ascites = confirms plasma leakage |
12. Management (How Is It Treated?)
🔑 There is NO specific antiviral drug for dengue. Treatment is entirely supportive.
Group A - Dengue Without Warning Signs (Home Management)
- Rest
- Paracetamol (acetaminophen) for fever and pain - doses every 6 hours
- Oral hydration - drink plenty of fluids (oral rehydration salts, coconut water, fruit juice, soup)
- DO NOT give: Aspirin, ibuprofen, or any NSAID - they thin blood and can cause serious bleeding
- Monitor at home: Watch for warning signs. Return to hospital immediately if any appear.
- Daily platelet check if falling
Group B - Dengue With Warning Signs (Hospital Admission Required)
IV Fluid Therapy is the cornerstone:
- Start with isotonic fluids (Normal Saline or Lactated Ringer's)
- Give cautiously - just enough to maintain circulation
- Monitor urine output (target: 0.5-1 mL/kg/hour)
- Check hematocrit every 4-6 hours - if rising, increase rate; if falling with clinical improvement, slow down
Blood products:
- Platelet transfusion: Only for platelets <10,000 with active bleeding (NOT just for a low number alone in a stable patient)
- Fresh Frozen Plasma (FFP): For DIC or coagulopathy with bleeding
- Packed Red Cells: If significant hemorrhage
Group C - Severe Dengue / Shock (ICU)
Dengue Shock Protocol:
- Immediate IV fluid resuscitation - 10-20 mL/kg isotonic fluid bolus over 1 hour
- Reassess: If improved, reduce rate gradually
- If not improved: repeat bolus, consider colloids (Dextran 40, HES)
- AVOID fluid overload - this is as dangerous as the shock itself
- Monitoring: BP, pulse, urine output, hematocrit every 1-2 hours
- Treat complications (hypoglycemia, metabolic acidosis, organ failure)
Recovery Phase Alert:
- During recovery, the leaked fluid re-enters the vessels
- Stop IV fluids early in recovery phase to avoid pulmonary edema
- Patient may develop bradycardia (slow heart rate) - usually benign
What NOT to Do
- ❌ No aspirin or NSAIDs (increases bleeding risk)
- ❌ No prophylactic platelets (in absence of bleeding)
- ❌ No antibiotics (it's viral - antibiotics do nothing)
- ❌ No steroids (not proven to help; may cause harm)
- ❌ Don't over-hydrate (fluid overload causes pulmonary edema in recovery)
13. Differential Diagnosis (What Can Look Like Dengue?)
| Disease | How to Tell It Apart |
|---|---|
| Malaria | More cyclic fever with rigors; no bone pain; positive blood smear/RDT for parasite; no characteristic rash |
| Typhoid | Prolonged step-ladder fever; relative bradycardia; coated tongue; low WBC but not as rapid; no retro-orbital pain; positive blood culture |
| Chikungunya | Very similar presentation! But joint pain is more severe and persistent; no plasma leakage; no platelet drop; positive chikungunya serology |
| Zika virus | Mild fever, rash, conjunctivitis (red eyes); milder disease; mainly concerning in pregnancy (microcephaly) |
| Influenza | Respiratory symptoms (cough, runny nose) more prominent; rapid flu test positive; no rash, no retro-orbital pain |
| Measles | High fever + rash + Koplik's spots in mouth; unvaccinated children; cough + conjunctivitis + coryza (3 C's); rash starts on face then spreads down |
| Rubella | Milder fever, lymphadenopathy (behind ears), rash spreads face to trunk; mainly concern in pregnancy |
| Leptospirosis | Jaundice + renal failure + red eyes (conjunctival suffusion); animal/water exposure history |
| Meningococcemia | Petechial rash similar to dengue but rapidly progresses, non-blanching purpura, meningism (neck stiffness); septic appearance; very unwell |
| Scrub typhus | Eschar (black scab at bite site); rash but starts on trunk; exposure to scrub/forest |
| Viral hepatitis | Jaundice prominent; AST/ALT very high (>10x); no rash; hepatitis serology positive |
Quick "Dengue vs Others" Cheat Sheet
| Feature | Dengue | Malaria | Chikungunya | Typhoid |
|---|---|---|---|---|
| Fever onset | Sudden | Cyclic (or continuous) | Sudden | Step-ladder |
| Retro-orbital pain | ✅ Classic | ❌ | ✅ (mild) | ❌ |
| Bone/joint pain | ✅✅ Severe | ✅ Mild | ✅✅ Severe joints | ✅ Mild |
| Rash | ✅ "White islands" | ❌ | ✅ Maculopapular | ✅ Rose spots |
| Thrombocytopenia | ✅✅ Marked | ✅ Mild | ✅ Mild | ✅ Mild |
| Leukopenia (low WBC) | ✅✅ | Usually normal | ✅ | ✅✅ |
| Plasma leakage/shock | Severe dengue only | In falciparum | ❌ | ❌ |
| Diagnostic test | NS1 antigen | Blood smear/RDT | Serology/PCR | Blood culture |
14. Prevention
Personal Protection
- Use mosquito repellents containing DEET, picaridin, or IR3535
- Wear long sleeves and pants during daytime (Aedes bites during the day!)
- Use window screens and air conditioning
- Sleep under bed nets (especially for daytime naps in children)
Eliminating Breeding Sites (Most Important)
Aedes mosquitoes breed in tiny collections of clean water. The rule: "Tip, Toss, Turn, and Treat"
- Tip out water from flower pots, tyres, buckets
- Toss or cover any container that can hold water
- Turn over unused containers
- Treat water tanks with larval insecticide (Temephos/Bacillus thuringiensis)
- Change water in flower vases weekly
- Clean blocked gutters
Vaccines
Dengvaxia (CYD-TDV):
- First dengue vaccine, approved in ~17 countries
- 3-dose schedule (0, 6, 12 months)
- Only approved for ages 9-45 years
- Critical point: Only for people who have had dengue before (seropositive)
- Giving it to someone who has never had dengue can make their first infection MORE severe (the vaccine mimics a first infection, so subsequent real infection behaves like a dangerous second infection)
- FDA-approved in the USA for ages 9-16 in endemic areas with confirmed prior dengue
Qdenga (TAK-003): Newer vaccine with different efficacy profile, approved in some countries.
Novel approach - Wolbachia-infected mosquitoes:
- Releasing Aedes mosquitoes infected with Wolbachia bacteria reduces viral replication inside the mosquito
- Trials in Colombia showed 95-97% reduction in dengue cases in treated areas - revolutionary approach
15. Quick Summary Card
DENGUE IN A NUTSHELL
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Caused by: Dengue Virus (4 serotypes: DEN-1,2,3,4)
Spread by: Aedes aegypti mosquito (day-biting)
Incubation: 4-7 days
3 Phases: Febrile → Critical → Recovery
Key symptoms: Sudden fever + breakbone pain + retro-orbital
pain + rash + low WBC + low platelets
Danger signs: Abdominal pain, persistent vomiting,
mucosal bleeding, restlessness, ↑ hematocrit
Labs: Thrombocytopenia + leukopenia + ↑ hematocrit
Diagnosis: NS1 antigen (early) / IgM antibody (late)
Treatment: Paracetamol + fluids (NO aspirin/NSAIDs!)
Severe dengue: IV fluids carefully; treat shock; no steroids
Prevention: Remove stagnant water + repellent + vaccine
(only if prior dengue)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. on Emerging Infectious Diseases
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.)
- Tintinalli's Emergency Medicine, Ch. 162
- Red Book 2021 (AAP Committee on Infectious Diseases)
- Park's Textbook of Preventive and Social Medicine
Dengue from basic to clinical
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.