Gotts shunt
Reading File
Finding Sources
Finding Sources
Searching the Web
Potts shunt cardiac surgery congenital heart disease
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a full answer:
Potts Shunt
You likely meant the Potts shunt (not "Gotts"). This is a well-established surgical procedure in congenital heart disease and pulmonary hypertension.
What Is It?
The Potts shunt is a direct anastomosis between the descending aorta and the left pulmonary artery (LPA). It creates a systemic-to-pulmonary connection that is physiologically similar to a patent ductus arteriosus (PDA).
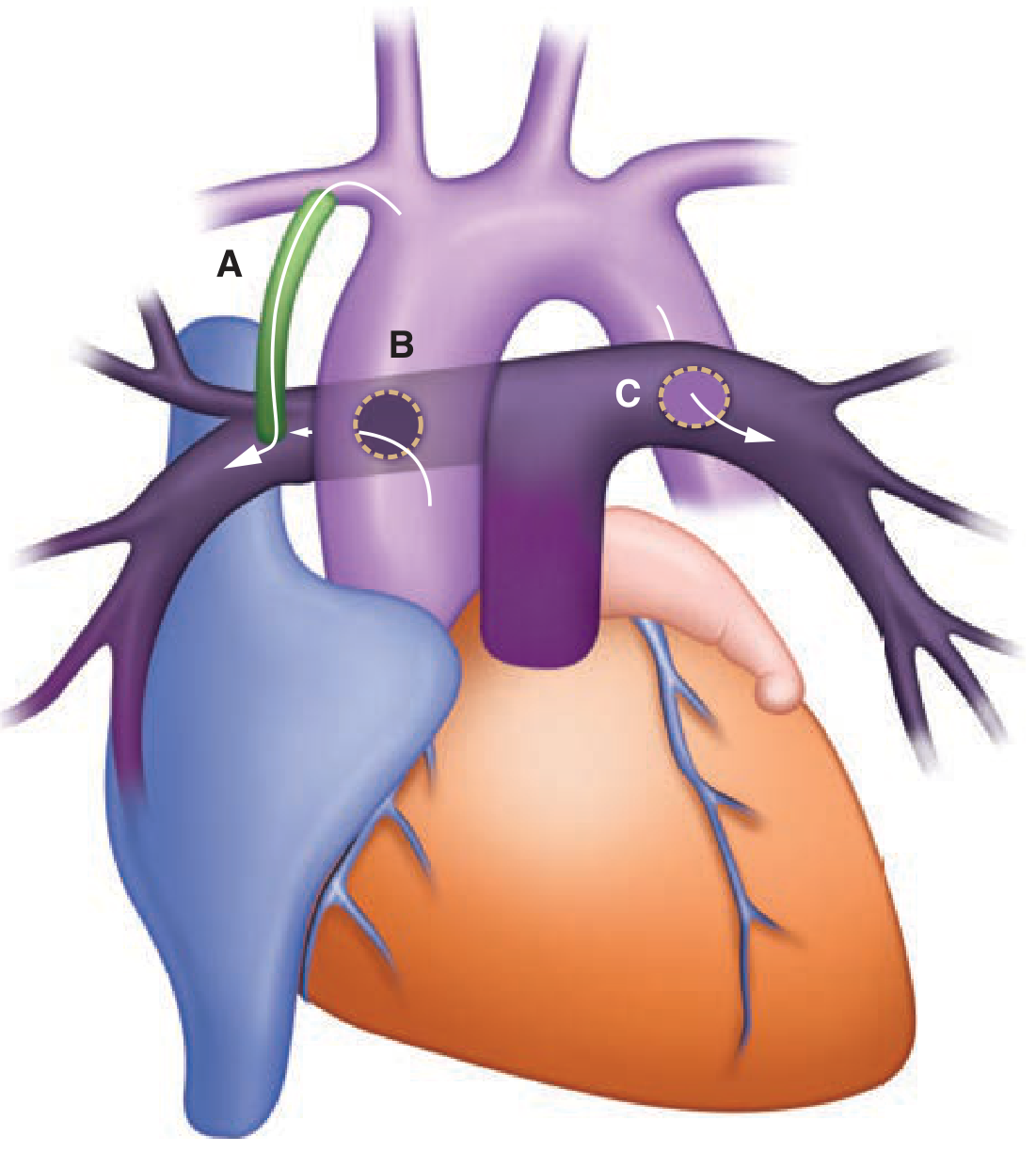
Diagram C shows the Potts shunt - descending aorta to left pulmonary artery.
Historical Context (Classic Use)
Originally, the Potts shunt was used as a palliative procedure for cyanotic congenital heart disease (e.g., Tetralogy of Fallot, pulmonary atresia, tricuspid atresia) to augment pulmonary blood flow in infants who could not undergo definitive repair.
However, it has been largely abandoned for this original indication, because:
-
The defect created is difficult to size precisely - it can be undersized (ineffective) or oversized (causing excessive pulmonary flow)
-
Excessive flow triggers pulmonary vascular disease
-
The modified Blalock-Taussig (BT) shunt replaced it, as tube graft size can be precisely selected
-
Fuster and Hurst's The Heart, 15th Ed., p. 1952
Modern Use: Reverse Potts Shunt for Pulmonary Hypertension
The Potts shunt has found a major new application as a palliative procedure for end-stage / refractory pulmonary arterial hypertension (PAH) - particularly in children.
Rationale
By creating a right-to-left shunt at the great artery level, it:
- Reduces right ventricular (RV) afterload - the RV can eject into both the pulmonary artery and, via the shunt, the aorta
- Equalizes systemic and pulmonary pressures, preventing acute RV failure
- Mimics the Eisenmenger physiology - a state that, paradoxically, is associated with better survival than refractory PAH without a shunt
Key Hemodynamic Advantage Over Other Shunts
Compared to atrial septostomy (atrial level) or VSD (ventricular level), the Potts shunt has a unique anatomical advantage:
- It selectively channels desaturated blood to the lower body
- Preserves oxygenated blood delivery to the brain and myocardium (upper body receives pre-shunt, oxygenated blood)
- A 10-15% difference in pre- vs. post-shunt oxygen saturation is considered ideal
Evidence
In one series of 21 patients (mean follow-up >2.5 years), 18 of 21 discharged patients showed:
- Reduction in pulmonary hypertension medications
- Decrease in BNP biomarker
- Clinical improvement
Transcatheter Potts Shunt
A percutaneous/transcatheter variant has been developed as an alternative to open surgery, creating the LPA-to-descending aorta anastomosis via catheter. This has shown benefit in small case series of decompensated PAH.
- Murray & Nadel's Textbook of Respiratory Medicine
- Miller's Anesthesia, 10th Ed., p. 10856-10857
Surgical Approach & Anesthetic Considerations
- Performed via lateral thoracotomy or midline sternotomy
- Anesthetic management is high-risk in PAH patients
- In-hospital mortality: 15-20%
- Monitoring: both upper body (pre-shunt) and lower body (post-shunt) blood pressure and oxygen saturation must be tracked simultaneously
Comparison of Systemic-to-Pulmonary Shunts
| Shunt | Connection | Status |
|---|---|---|
| Modified BT shunt | Subclavian artery → ipsilateral PA (via tube graft) | Current standard for CHD palliation |
| Waterston shunt | Ascending aorta → right PA (direct) | Largely abandoned |
| Potts shunt | Descending aorta → left PA (direct) | Abandoned for CHD; used for PAH |
| Glenn shunt | SVC → PA (systemic vein to PA) | Used in single-ventricle staged palliation |
Summary
The Potts shunt is a direct descending aorta-to-left PA anastomosis. Originally a palliative procedure for cyanotic CHD (now replaced by the modified BT shunt), it has been repurposed as a reverse Potts shunt for end-stage pulmonary arterial hypertension. Its anatomical location offers the important advantage of sparing the brain and heart from hypoxic blood while unloading the failing right ventricle - making it superior in concept to atrial or ventricular level shunts for this purpose.
It's Gott's shunt
Finding Sources
Searching the Web
Gott shunt heparinized tube descending aortic surgery
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC6416372
Apologies for the mix-up! Here is a full answer on the Gott shunt:
Gott Shunt
What Is It?
The Gott shunt is a heparin-bonded (TDMAC-heparin coated) passive tube shunt used during surgery on the descending thoracic aorta to maintain distal aortic perfusion while the aorta is cross-clamped. It was developed specifically to avoid the need for systemic heparinization - a major advantage over other bypass circuits.
Purpose
When the descending thoracic aorta is cross-clamped for aneurysm repair or aortic dissection surgery, everything distal to the clamp becomes ischemic - including the:
- Spinal cord (risk of paraplegia)
- Kidneys (risk of renal failure)
- Visceral organs (mesenteric ischemia)
The Gott shunt bypasses the cross-clamp zone, passively diverting blood from the proximal aorta/left ventricle to the distal aorta, maintaining perfusion to these organs.
Construction & How It Works
- A 9 mm TDMAC-heparin coated tube (typically ~9-9.5 mm diameter)
- The heparin bonded to the inner surface of the tube prevents thrombosis within the shunt without requiring full systemic heparinization
- Flow is passive (driven by the pressure gradient between proximal and distal aorta) - no pump is needed
- Typical shunt flows: 1100-4900 mL/min (mean ~2500 mL/min)
Placement Sites
The shunt is inserted between a proximal and distal cannulation point:
| Proximal site | Distal site |
|---|---|
| Ascending aorta (preferred) | Descending aorta |
| Left ventricle apex | Femoral artery |
| Proximal descending aorta | Distal descending aorta |
The proximal and distal sites are chosen based on the location and extent of the aneurysm and whether there is concomitant aortic disease along the conduit.
Advantages
- No systemic heparin required - major benefit in patients at bleeding risk (e.g., traumatic aortic injury, dissection)
- Technically simple - no pump, oxygenator, or full bypass circuit needed
- Provides passive distal perfusion protecting spinal cord, kidneys, and viscera
- Can be placed quickly
Limitations
- Flow is passive and uncontrolled - cannot be actively adjusted (unlike left heart bypass)
- Provides less hemodynamic control compared to left heart bypass (LHB) or full cardiopulmonary bypass (CPB)
- Does not unload the proximal aorta/left ventricle as effectively
- Cross-clamping still causes significant proximal hypertension requiring pharmacologic management
As a result, many centers prefer left heart bypass (LHB) with a centrifugal pump (left atrium → femoral artery) for its superior flow control, though the Gott shunt remains a useful and simpler alternative.
Modified Gott Shunt
A modification described in recent literature adds an extra 10 mm tube from the side port of the ascending aortic cannula to the left subclavian artery, in addition to the standard ascending-to-descending connection. This simultaneously addresses:
- Spinal cord perfusion
- Left ventricular overload reduction
- Brain/cerebral perfusion
during complex distal arch and descending aortic surgery - described in PMC6416372.
Clinical Context
-
Used in open repair of descending thoracic aortic aneurysms and type B aortic dissections
-
Approach is usually via left thoracotomy
-
Has largely been superseded in elective cases by TEVAR (thoracic endovascular aortic repair), though open repair with the Gott shunt or LHB remains necessary when endovascular options are unsuitable
-
In-hospital use with a 9 mm shunt over 267 consecutive patients showed effective organ protection with mean shunt flow of ~2526 mL/min
-
Miller's Anesthesia, 10th Ed., p. 7986-7987
This is a shared conversation. Sign in to Orris to start your own chat.