Indication vitamin E
Indications for Vitamin E
1. Vitamin E Deficiency States (Primary Indication)
- Celiac disease, chronic cholestatic liver disease, small-intestinal resection, or bariatric surgery
- Cystic fibrosis - deficiency presents with areflexia and hemolytic anemia
- Prolonged cholestasis in children
- Abetalipoproteinemia (Bassen-Kornzweig syndrome) - impaired absorption of fat-soluble vitamins; high-dose vitamin E (5000-7000 mg/d) is required
- Familial isolated vitamin E deficiency (AVED) - due to mutation in the α-tocopherol transfer protein gene (TTPA); causes spinocerebellar ataxia
- Chylomicron retention disease (Anderson disease) and familial hypobetalipoproteinemia
- Premature/very-low-birth-weight infants - supplementation prevents hemolysis and retinopathy
- Adults: 800-1200 mg/d of α-tocopherol
- Children: 400 mg/d (water-miscible esters) orally, or 2 mg/kg/d IM
- Abetalipoproteinemia: up to 5000-7000 mg/d
2. Neurological Manifestations of Deficiency
- Spinocerebellar syndrome - ataxia, areflexia, loss of vibration and position sense
- Peripheral neuropathy
- Ophthalmoplegia, skeletal myopathy, pigmented retinopathy
- Mimics Friedreich's ataxia
3. Neonatal/Premature Infants
- Prevention and treatment of hemolytic anemia in very-low-birth-weight infants
- Protection against oxygen-induced retrolental fibroplasia (retinopathy of prematurity)
- Reduced risk of bronchopulmonary dysplasia and intraventricular hemorrhage of prematurity
4. Non-alcoholic Steatohepatitis (NASH/NAFLD)
- Vitamin E may have favorable therapeutic effects in non-cirrhotic, non-diabetic patients with NASH (nonalcoholic steatohepatitis)
- It is among the most studied antioxidants for NAFLD treatment in adults and pediatric studies
5. Macular Degeneration
- When given in combination with other antioxidants (e.g., vitamin C, zinc - AREDS formula), vitamin E may help prevent age-related macular degeneration (AMD)
6. Immune Function Enhancement
- High doses (60-800 mg/d) have shown improved immune function and reduced upper respiratory infections (colds) in nursing home residents in controlled trials
7. Hepatic Rickets (Adjunct)
- α-Tocopheryl polyethylene glycol-1000 succinate (TPGS) - a water-soluble form of vitamin E - is used as an adjunct in hepatic rickets unresponsive to oral vitamin D, as it enhances fat-soluble vitamin absorption by forming micelles
Indications Lacking Convincing Evidence (Not Recommended)
- Cardiovascular disease prevention - intervention studies show no efficacy
- Cancer prevention - no efficacy shown; doses >400 mg/d may increase all-cause mortality and prostate cancer risk (especially with selenium)
- Sexual performance enhancement
- Intermittent claudication
- Anti-aging
- Hemolytic-uremic syndrome
Toxicity / Contraindications
- Doses >800 mg/d reduce platelet aggregation and interfere with vitamin K metabolism - contraindicated with warfarin and antiplatelet agents (aspirin, clopidogrel)
- GI side effects (nausea, flatulence, diarrhea) at doses >1 g/d
- High concentrations have cytotoxic effects on lymphocytes in vitro - caution with mega-doses
Create a comparison table of vitamin E forms and bioavailability
Vitamin E Forms and Bioavailability - Comparison Table
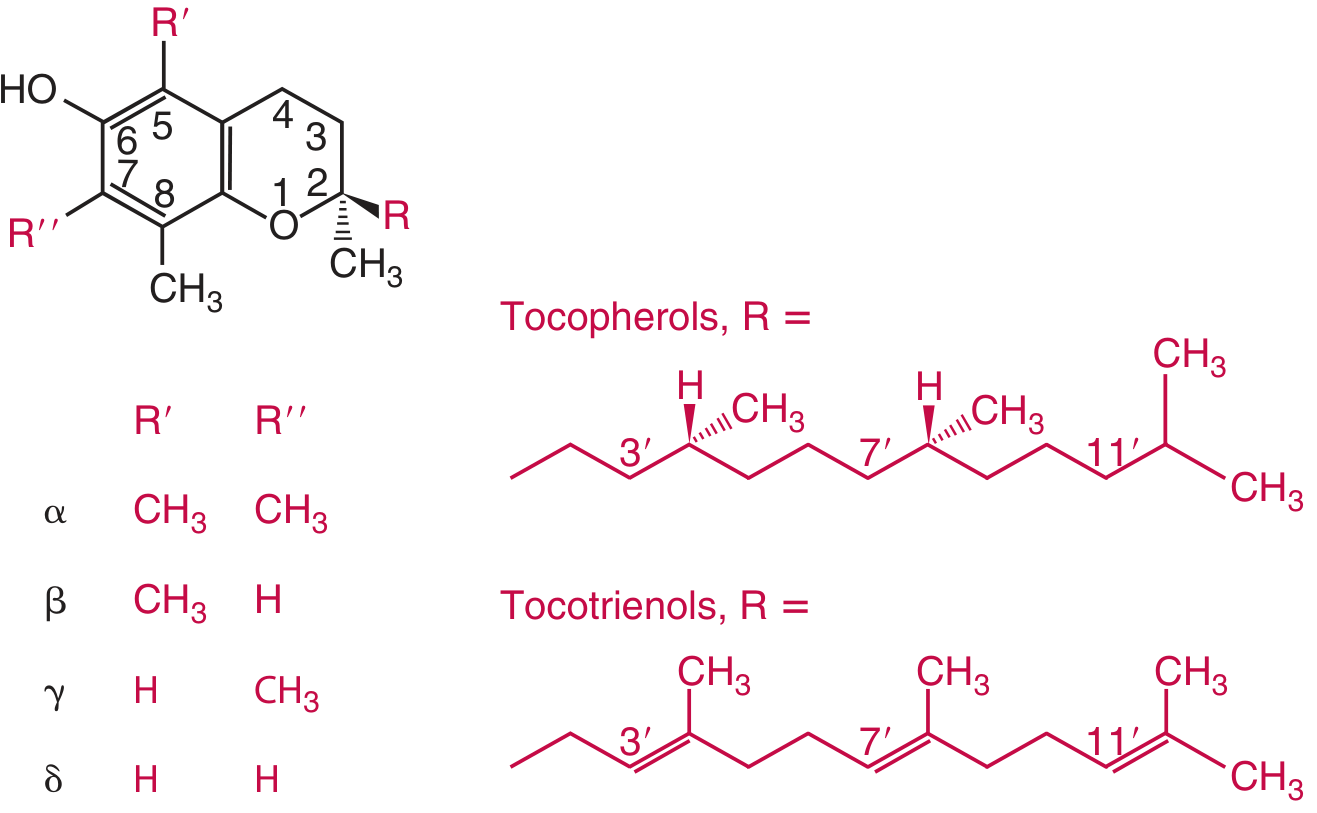
Part 1: The 8 Natural Forms
| Form | Class | Methyl Groups (positions 5 & 7) | Side Chain | Relative Biological Activity (α-TE equivalent) |
|---|---|---|---|---|
| α-Tocopherol | Tocopherol | Both positions (5 & 7) methylated | Saturated phytyl | 1.0 (reference standard) |
| β-Tocopherol | Tocopherol | Position 5 only | Saturated phytyl | 0.5 |
| γ-Tocopherol | Tocopherol | Position 7 only | Saturated phytyl | 0.1 |
| δ-Tocopherol | Tocopherol | Neither position methylated | Saturated phytyl | ~0.03 |
| α-Tocotrienol | Tocotrienol | Both positions methylated | Unsaturated (3 double bonds at 3', 7', 11') | 0.3 |
| β-Tocotrienol | Tocotrienol | Position 5 only | Unsaturated | ~0.05 |
| γ-Tocotrienol | Tocotrienol | Position 7 only | Unsaturated | ~0.01 |
| δ-Tocotrienol | Tocotrienol | Neither position methylated | Unsaturated | ~0.01 |
α-Tocopherol equivalent (α-TE) = α-tocopherol + (β-tocopherol × 0.5) + (γ-tocopherol × 0.1) + (α-tocotrienol × 0.3) (Tietz Textbook of Laboratory Medicine, 7th Ed.)
Part 2: Natural vs. Synthetic α-Tocopherol (Key Clinical Distinction)
| Property | Natural RRR-α-Tocopherol (d-α-tocopherol) | Synthetic all-rac-α-Tocopherol (dl-α-tocopherol) |
|---|---|---|
| Stereoisomers | Single isomer: RRR only | 8 racemic forms: RRR, RSR, RRS, RSS, SRR, SSR, SRS, SSS |
| Biological activity | 100% (reference) | ~50% of natural form (only 1 in 8 isomers is RRR) |
| Recognition by α-TTP | High affinity - preferentially incorporated into VLDL | Poor recognition by α-tocopherol transfer protein |
| Plasma retention | Longer half-life; efficiently recycled (<60 hr half-life in circulation) | Rapidly cleared and excreted |
| IU equivalence | 1 mg = 1.49 IU | 1 mg = 1.10 IU |
| Source | Vegetable oils, wheat germ, sunflower, nuts | Synthetic supplements, fortified foods |
| Regulatory note (US RDA) | RDA of 15 mg/d must be met by RRR form only - other forms not counted | Not counted toward meeting the RDA |
Part 3: Absorption and Bioavailability by Form
| Step | α-Tocopherol | Other Tocopherols (β, γ, δ) | Tocotrienols |
|---|---|---|---|
| Intestinal absorption | Passive diffusion + cholesterol transporters; requires bile salts, pancreatic esterases, intact mucosa | Same mechanism; absorbed non-selectively in intestine | Same mechanism; absorbed non-selectively |
| Chylomicron packaging | Packed into chylomicrons with dietary fat; absorption depends on fat content of meal | Packed non-selectively | Packed non-selectively |
| Hepatic processing | Preferentially selected by α-TTP for incorporation into VLDL; distributed to all tissues | Degraded and excreted after hepatic uptake; NOT incorporated into VLDL by α-TTP | Degraded and excreted; not preferentially retained |
| Plasma level | Predominant form; 5.5-18.0 µg/mL (reference range) | γ-tocopherol: 0.5-3.5 µg/mL (much lower despite being the major US dietary form) | Very low plasma levels |
| Tissue storage | Stored in adipose tissue; high in adrenal glands, testes, platelets | Minimal storage | Minimal storage |
| Metabolism | CYP450 side-chain oxidation; excreted as tocopherolonic acid in urine and as β-glucuronide in bile | Faster CYP450 side-chain degradation; γ-carboxyethyl-hydroxychroman (γ-CEHC) is urinary metabolite | Faster degradation via CYP450 |
| Half-life | <60 hours; rapidly recycled between liver and systemic circulation | Shorter | Shorter |
| Overall bioavailability | Highest | Low (γ-tocopherol is the major dietary form in US but is ~1/4 to 1/10 of plasma α-tocopherol) | Lowest among the forms |
Part 4: Dietary Sources by Form
| Form | Primary Food Sources |
|---|---|
| α-Tocopherol | Sunflower oil, safflower oil, wheat germ oil, almonds, spinach, broccoli |
| γ-Tocopherol | Soybean oil, corn oil, peanut oil, most plant seeds - major form in US diet |
| δ-Tocopherol | Soybean oil, palm oil |
| β-Tocopherol | Wheat germ, some vegetable oils (minor) |
| Tocotrienols (all) | Palm oil, rice bran oil, barley, oats, rye |
Part 5: Special Pharmaceutical Forms
| Form | Key Feature | Clinical Use |
|---|---|---|
| Water-miscible α-tocopherol esters (TPGS) | Soluble in water; forms micelles | Vitamin E supplementation in cholestasis/fat malabsorption; children with deficiency (400 mg/d orally) |
| α-Tocopherol acetate | Ester form; stable; hydrolyzed to active tocopherol after absorption | Most common supplement form |
| α-Tocopherol succinate | Ester form; more stable than acetate | Used in some fortified foods and supplements |
| IV α-tocopherol | Complete bioavailability via bloodstream | 9.1 mg/d (10 IU/d) recommended for IV nutrition; lower dose than oral due to 100% delivery |
ABFlo vs Deriphyillin
ABFlo acebrophylline vs Deriphyllin theophylline etofylline comparison bronchodilator India
https://pmc.ncbi.nlm.nih.gov/articles/PMC4225926
ABFlo vs Deriphyllin - Full Comparison
Brand Identity
| Feature | ABFlo | Deriphyllin / Deriphyllin Retard |
|---|---|---|
| Active ingredient(s) | Acebrophylline 100 mg | Theophylline 23 mg + Etofylline 77 mg (standard) OR Theophylline 69 mg + Etofylline 231 mg (Retard 300 mg) |
| Drug class | Xanthine derivative + mucoactive hybrid | Methylxanthine combination |
| Chemical nature | Ambroxol + Theophylline-7-Acetate (hybrid molecule) | Theophylline (1,3-dimethylxanthine) + Etofylline (7-(2-hydroxyethyl)theophylline) |
| Formulation | Capsule (oral) | Tablet / Retard (slow-release) tablet |
| Typical dose | 100 mg twice daily | Standard: 1 tab TDS; Retard: 300 mg once daily |
Mechanism of Action
| Mechanism | ABFlo (Acebrophylline) | Deriphyllin (Theophylline + Etofylline) |
|---|---|---|
| PDE inhibition | Inhibits intracellular PDE → ↑ cAMP → bronchial smooth muscle relaxation | Non-selective PDE inhibitor (PDE3, PDE4, PDE5) → ↑ cAMP → bronchodilation |
| Adenosine antagonism | Minimal/absent - key advantage | YES - antagonizes adenosine A1 receptors (responsible for arrhythmias and seizures) |
| Anti-inflammatory | Selectively inhibits phosphatidylcholine, phospholipase A2, TNF-α, and leukotrienes | ↑ IL-10 release; inhibits NF-κB nuclear translocation; promotes eosinophil/neutrophil apoptosis |
| Mucolytic/mucokinetic | YES - ambroxol component: lowers mucus gel viscosity, ↑ sol phase, augments ciliary motility → ↑ mucociliary clearance | None |
| Surfactant stimulation | YES (ambroxol component stimulates surfactant synthesis) | None |
| Catecholamine release | No | ↑ Epinephrine release |
Efficacy
| Parameter | ABFlo (Acebrophylline) | Deriphyllin (Theophylline + Etofylline) |
|---|---|---|
| Bronchodilation | Comparable to SR theophylline | Established bronchodilator |
| FEV1 improvement in COPD | Comparable improvement at Day 21 and Day 42 | Comparable improvement |
| Symptom relief (dyspnea, cough) | Comparable | Comparable |
| Mucociliary benefit | Additional benefit - reduces sputum viscosity and improves clearance | None |
| Add-on to LAMA (Tiotropium) | Used as add-on in moderate COPD | Used as add-on |
| Asthma | Yes | Yes |
| COPD | Yes (preferred due to mucolytic action + better safety) | Yes (widely used, very low cost) |
Safety / Adverse Effects
| Side Effect | ABFlo (Acebrophylline) | Deriphyllin (Theophylline + Etofylline) |
|---|---|---|
| Palpitations / tachycardia | Less frequent (no adenosine antagonism) | More frequent (adenosine A1 antagonism → arrhythmia risk) |
| Tremor | Rare | Common (CNS stimulation) |
| Insomnia | Rare | Common |
| Seizures | Very rare | Risk at toxic levels (adenosine A1 antagonism) |
| Nausea / dyspepsia | Mild GI effects | Nausea, dyspepsia common |
| Headache | Rare | Reported |
| Therapeutic window | Wider - safer profile | Narrow therapeutic index (theophylline: 10-20 mg/L) - toxicity risk if slightly overdosed |
| Cardiac risk patients | Safer option | Caution - arrhythmogenic |
| Overall | Safer (fewer CVS and CNS effects) | More adverse effects, especially at 300 mg dose |
Pharmacokinetics & Monitoring
| Parameter | ABFlo (Acebrophylline) | Deriphyllin (Theophylline + Etofylline) |
|---|---|---|
| TDM (therapeutic drug monitoring) | Not required | Required for chronic use - serum theophylline levels must be monitored |
| Drug interactions | Fewer | Multiple (CYP1A2 substrate - affected by ciprofloxacin, erythromycin, cimetidine, smoking, phenytoin) |
| Liver metabolism | Yes | CYP1A2 and OAA substrate - hepatic metabolism; dose adjustment in liver disease |
Practical / Cost Comparison
| Factor | ABFlo | Deriphyllin Retard |
|---|---|---|
| Cost (India) | ~₹1/tablet (very cheap) | |
| Availability | Widely available | Widely available |
| Patient population | Preferred in patients with productive cough/mucus, cardiac comorbidities, or those intolerant to theophylline | Preferred when cost is the primary concern; still widely used in primary care across India |
| Monitoring needed | No | Yes (TDM) |
| Pregnancy / caution | Use with caution | Use with caution |
Summary: When to Choose Which?
| Clinical Scenario | Preferred Drug |
|---|---|
| COPD with productive cough / excessive mucus | ABFlo (added mucolytic benefit) |
| Patient with cardiac arrhythmia / palpitations | ABFlo (no adenosine antagonism) |
| Need for TDM-free management | ABFlo |
| Cost-sensitive patient, primary care setting | Deriphyllin |
| Stable COPD, low cardiac risk, well-monitored | Either (comparable efficacy) |
| Acute exacerbation | Neither (methylxanthines not recommended in acute exacerbations per GOLD guidelines) |
Vs Erdomac AB
Erdomac AB tablet composition ingredients erdosteine acebrophylline India
erdosteine mechanism action mucolytic antioxidant COPD exacerbations clinical evidence
erdosteine COPD chronic bronchitis mucolytic
ABFlo vs Deriphyllin vs Erdomac AB - Three-Way Comparison
Brand Identity
| Feature | ABFlo | Deriphyllin Retard | Erdomac AB |
|---|---|---|---|
| Active ingredients | Acebrophylline 100 mg | Theophylline 69 mg + Etofylline 231 mg | Acebrophylline 100 mg + Erdosteine 300 mg |
| Drug class | Xanthine derivative + mucoregulator (hybrid) | Methylxanthine combination | Bronchodilator-mucoregulator + mucolytic/antioxidant (dual action) |
| Chemical nature | Ambroxol + Theophylline-7-acetate | 1,3-dimethylxanthine + 7-(2-hydroxyethyl)theophylline | Acebrophylline (hybrid) + Erdosteine (thiol prodrug) |
| Formulation | Capsule | Sustained-release tablet | Bi-layered film-coated tablet (patented) |
| Typical dose | 100 mg BD | 300 mg OD | 1 tablet BD |
| Manufacturer | Multiple (generic) | Multiple (generic) | Theon Pharmaceuticals (first DCGI-licensed in India) |
| Primary indication | Asthma, COPD, chronic bronchitis | COPD, asthma (long-term management) | Chronic bronchitis in COPD |
Mechanism of Action
| Mechanism | ABFlo | Deriphyllin | Erdomac AB |
|---|---|---|---|
| Bronchodilation | PDE inhibition → ↑ cAMP → smooth muscle relaxation | Non-selective PDE inhibition (PDE3/4/5) → ↑ cAMP | Same as ABFlo (via acebrophylline component) |
| Adenosine antagonism | Minimal | YES (arrhythmia/seizure risk) | Minimal (acebrophylline component only) |
| Mucolytic | Partial - ambroxol lowers gel-phase viscosity, ↑ sol phase | None | Dual mucolysis: acebrophylline (ambroxol) + erdosteine cleaves disulfide bonds in mucoproteins via free thiol groups |
| Mucociliary clearance | ↑ Ciliary motility (ambroxol) | None | ↑↑ Enhanced (both components act synergistically) |
| Anti-inflammatory | Inhibits phospholipase A2, TNF-α, leukotrienes | ↑ IL-10; inhibits NF-κB | Acebrophylline (leukotrienes, TNF-α) + Erdosteine (reduces oxidative stress-driven inflammation) |
| Antioxidant | None | None | YES - Erdosteine's free thiol metabolites neutralize reactive oxygen species (ROS); protects α1-antitrypsin from oxidative inactivation |
| Anti-bacterial adhesion | None | None | YES - Erdosteine reduces bacterial adhesion to airway epithelium; ↑ IgA antibodies |
| Surfactant production | ↑ (ambroxol component) | None | ↑ (acebrophylline/ambroxol component) |
| Reduction of bronchial hyperresponsiveness | Yes | Partial | Yes |
Efficacy Evidence
| Parameter | ABFlo | Deriphyllin | Erdomac AB |
|---|---|---|---|
| FEV1 improvement in COPD | Comparable to SR theophylline | Established | Same as ABFlo + additional mucolytic benefit |
| COPD exacerbation reduction | Moderate | Moderate | Superior - Erdosteine reduces rate, duration, and hospitalization risk from AECOPD (EQUALIFE, RESTORE studies) |
| Exacerbation reduction vs NAC | - | - | Erdosteine ranked #1 among thiol mucolytics (erdosteine > carbocysteine > NAC) in network meta-analysis (RR 0.74, 95% CI 0.68-0.80) |
| Risk of ≥1 exacerbation | Moderate | Moderate | Significantly reduced (P<0.01) |
| Hospitalization risk | - | - | Significantly reduced (P<0.05) by erdosteine component |
| Sputum clearance | Good | None | Excellent (dual mechanism) |
| Duration of exacerbations | - | - | Shortened |
| Quality of life | Moderate | Moderate | Improved (RESTORE study) |
| Effect with ICS use | - | - | Effective regardless of concomitant ICS treatment |
| Clinical trial vs ABFlo + NAC | Reference | - | Phase 3 RCT: Erdomac AB (erdosteine + acebrophylline) vs acebrophylline + acetylcysteine 600 mg - comparable efficacy with better tolerability for Erdomac AB |
Safety / Adverse Effects
| Side Effect | ABFlo | Deriphyllin | Erdomac AB |
|---|---|---|---|
| Cardiac arrhythmias | Rare | More frequent (adenosine A1 antagonism) | Rare |
| Tremor / Insomnia | Rare | Common (CNS stimulation) | Rare |
| Seizures at toxicity | Very rare | Risk present | Very rare |
| GI effects | Mild (nausea, abdominal discomfort) | Nausea, dyspepsia | Mild and well-tolerated |
| Therapeutic drug monitoring | Not required | Required (serum theophylline 10-20 mg/L) | Not required |
| Long-term safety | Good | Concern at higher doses | Best - suitable for long-term chronic therapy |
| Drug interactions | Minimal | Multiple (CYP1A2 - erythromycin, ciprofloxacin, cimetidine, smoking) | Minimal |
| Overall safety rank | Good | Least safe | Best |
Pharmacokinetics
| Parameter | ABFlo | Deriphyllin | Erdomac AB |
|---|---|---|---|
| Erdosteine metabolism | - | - | Prodrug - hydrolyzed in body to active thiol metabolites |
| Monitoring | None needed | TDM mandatory | None needed |
| Hepatic metabolism | Yes | CYP1A2/OAA | Yes (both components) |
Cost & Practical Profile
| Factor | ABFlo | Deriphyllin | Erdomac AB |
|---|---|---|---|
| Cost (India) | ~₹8-10/capsule | ~₹1/tablet (cheapest) | Higher (newer branded combination) |
| Regulatory status | Widely available | Widely available | DCGI-licensed; first-of-kind in India |
| Formulation advantage | Standard capsule | SR tablet | Patented bi-layer - optimized release kinetics for both molecules |
| TDM needed | No | Yes | No |
| Suitable for long-term use | Yes | With monitoring | Yes (best suited) |
Clinical Scenario Guide
| Scenario | Best Choice |
|---|---|
| COPD + productive cough + frequent exacerbations | Erdomac AB (dual mucolysis + antioxidant + exacerbation reduction) |
| COPD + cardiac comorbidity / arrhythmia risk | ABFlo or Erdomac AB (avoid Deriphyllin) |
| COPD with oxidative stress / smoking history | Erdomac AB (erdosteine provides antioxidant protection) |
| Cost-sensitive patient, primary care | Deriphyllin (with TDM) |
| Simple bronchodilation, asthma, no mucus issue | ABFlo |
| COPD needing long-term maintenance therapy | Erdomac AB (best tolerability for chronic use) |
| Acute exacerbation | None of the above (methylxanthines not recommended in acute AECOPD per GOLD guidelines) |
Summary
In CKD PATIENT
ABFlo acebrophylline Deriphyllin theophylline Erdomac erdosteine dose adjustment CKD chronic kidney disease renal impairment
theophylline CKD renal failure dose adjustment protein binding uremia pharmacokinetics
erdosteine renal impairment CKD dose contraindication eGFR prescribing information
https://pmc.ncbi.nlm.nih.gov/articles/PMC3614285
ABFlo vs Deriphyllin vs Erdomac AB in CKD Patients
Quick CKD Safety Summary
| Drug | CKD Stage 1-2 (eGFR >60) | CKD Stage 3 (eGFR 30-60) | CKD Stage 4 (eGFR 15-30) | CKD Stage 5 / ESRD (eGFR <15 / Dialysis) |
|---|---|---|---|---|
| ABFlo (Acebrophylline) | Use normally | Use with caution, no specific dose adjustment | Use with caution | Limited data; avoid if possible |
| Deriphyllin (Theophylline + Etofylline) | Use with TDM | Use with TDM; monitor closely - ↑ free drug due to ↓ protein binding | Use at reduced dose with TDM; risk ↑↑ | Avoid / use only with strict TDM - dialyzable but requires replacement dosing |
| Erdomac AB (Acebrophylline + Erdosteine) | Use normally | Use with monitoring | Reduce erdosteine dose / use cautiously | Contraindicated (erdosteine: CrCl <25 mL/min is a contraindication) |
Drug-by-Drug Analysis in CKD
1. Deriphyllin (Theophylline + Etofylline) - MOST PROBLEMATIC in CKD
- In adults, only 10-15% of theophylline is renally excreted unchanged; the rest is hepatically metabolized (CYP1A2)
- Formal dose adjustment is NOT required for renal dysfunction alone based on excretion
- However, CKD causes major pharmacokinetic disruptions that make theophylline dangerous:
| CKD Effect | Impact on Theophylline |
|---|---|
| ↓ Protein binding (uremic toxins displace drug from albumin) | ↑ Free (active) theophylline fraction → toxicity at "normal" total serum levels |
| ↓ CYP1A2 activity (uremic toxins inhibit hepatic enzymes) | ↓ Hepatic clearance → drug accumulation |
| Metabolite accumulation | Active metabolites (e.g., 1-methylxanthine) accumulate in renal failure (especially with allopurinol co-use) |
| Hypoalbuminemia in CKD/nephrotic syndrome | Further ↑ free drug fraction |
| Adenosine A1 antagonism | CKD patients are prone to arrhythmias; theophylline's cardiac risk is amplified |
| Narrow therapeutic index (10-20 mg/L) | Standard TDM targets may be falsely reassuring since free drug is elevated |
- Arrhythmias (particularly dangerous in CKD patients with cardiovascular comorbidity)
- Seizures
- Severe nausea/vomiting
- Hypercalcemia (theophylline/aminophylline is listed as a cause of hypercalcemia in CKD)
Verdict: Use only if essential, with mandatory TDM, targeting lower end of therapeutic range. Monitor free drug levels if possible. Avoid in ESRD/dialysis patients unless no alternative.
2. ABFlo (Acebrophylline) - RELATIVELY SAFER in CKD
| CKD consideration | Details |
|---|---|
| Renal excretion | Primarily hepatically metabolized; renal excretion is minor |
| Dose adjustment | No specific formal dose adjustment guideline; use with general caution as GFR declines |
| Protein binding changes | Less impacted than theophylline since it lacks the narrow therapeutic window issue |
| Adenosine antagonism | Minimal - lower cardiac risk in CKD patients |
| TDM required | No |
| Mucolytic benefit | Retained in CKD patients who have COPD with productive cough |
| GI risk | Mild GI effects possible; caution in CKD patients who may have gastroparesis |
| Dialysis | No specific supplemental dosing required |
Verdict: Preferred over Deriphyllin in CKD. No TDM burden. Lower cardiac and CNS risk. Usable across CKD stages 1-4 with general monitoring.
3. Erdomac AB (Acebrophylline + Erdosteine) - DUAL CONSIDERATION in CKD
| Feature | Details |
|---|---|
| Excretion | Excreted in urine as active thiol metabolites; renal clearance is the primary elimination route |
| Protein binding | 64.5% |
| Half-life | ~1.46 hr (erdosteine), ~1.62 hr (active metabolite) |
| Accumulation in renal failure | Active metabolites accumulate as GFR drops |
| Formal contraindication | CrCl <25 mL/min (severe renal impairment) - CONTRAINDICATED |
| Moderate CKD (CrCl 25-50) | Use with caution; consider dose reduction to once daily |
| CKD Stage 3 (eGFR 30-60) | Use cautiously; monitor |
| ESRD / Dialysis | Contraindicated |
- Shown to reduce CsA (cyclosporine)-induced nephrotoxicity
- Protects against gentamicin nephrotoxicity
- Improves oxidative stress markers (glutathione peroxidase, catalase, MDA, nitric oxide)
- Improves renal functional markers (BUN, serum creatinine, uric acid) in animal models
Verdict: Acceptable in mild-moderate CKD (CrCl >50 mL/min) with standard dosing. Reduce to OD dosing in CrCl 25-50 mL/min. Contraindicated below CrCl 25 mL/min.
Practical Prescribing Guide for CKD
| CKD Stage | eGFR | Best Choice | Cautions |
|---|---|---|---|
| Stage 1-2 (mild) | >60 | Any of the three; Erdomac AB preferred for added antioxidant benefit | TDM for Deriphyllin |
| Stage 3a | 45-60 | ABFlo or Erdomac AB (standard dose) | Avoid Deriphyllin unless no alternative + strict TDM |
| Stage 3b | 30-45 | ABFlo preferred; Erdomac AB with reduced erdosteine dose (OD) | Deriphyllin - avoid or use at low dose with TDM; monitor free drug |
| Stage 4 | 15-30 | ABFlo (use with caution) | Erdomac AB - use only if CrCl >25; Deriphyllin - avoid |
| Stage 5 / ESRD | <15 | ABFlo (with caution, limited data) | Erdomac AB - contraindicated; Deriphyllin - avoid; if used, strict TDM + replacement dose post-HD |
Additional CKD-Specific Considerations
| Issue | Deriphyllin | ABFlo | Erdomac AB |
|---|---|---|---|
| Hyperkalemia risk | Theophylline can cause hypokalemia (shifts K+ intracellularly) - may temporarily mask CKD hyperkalemia, then rebound | Minimal | Minimal |
| Cardiovascular risk | HIGH - arrhythmias in CKD patients with CVD | Low | Low (acebrophylline component only) |
| Drug interactions in CKD | Many - allopurinol (common in CKD/gout) ↑ theophylline levels; fluoroquinolones (common in CKD infections) ↑ theophylline toxicity | Minimal | Minimal |
| Monitoring burden | High (TDM mandatory) | Low | Low |