Adult ddh etiology pathology and signs and symptoms and investigations and evaluation treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
adult developmental dysplasia hip DDH etiology pathology signs symptoms investigations treatment 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
I now have all the material needed for a comprehensive, illustrated answer. Let me compile the full detailed response:
Adult Developmental Dysplasia of the Hip (DDH)
1. DEFINITION & OVERVIEW
Developmental dysplasia of the hip (DDH) describes a spectrum of hip abnormalities ranging from mild acetabular undercoverage of the femoral head to complete dislocation. In adults, DDH is the end result of undiagnosed or undertreated childhood DDH - either because it was never detected, or because a mild/moderate form was missed. Adult DDH is one of the most important causes of premature hip osteoarthritis, accounting for up to 20-40% of all hip replacement procedures in young adults.
- Campbell's Operative Orthopaedics 15th Ed 2026
- Miller's Review of Orthopaedics 9th Ed
2. ETIOLOGY & RISK FACTORS
The etiology of adult DDH is multifactorial. It is the persistence or late presentation of dysplasia originating perinatally or in early childhood.
2A. Primary Etiological Factors
| Category | Details |
|---|---|
| Genetic / Familial | Family history of DDH raises risk to ~10%. Polygenetic - candidate genes include COL1A1 (connective tissue), GDF5 (osteogenesis), UQCC1/ASPN (chondrogenesis), TGFB1 (cell growth) |
| Hormonal | Maternal relaxin crosses the placenta and causes fetal ligamentous laxity; more pronounced in girls |
| Mechanical / Intrauterine | Breech presentation, oligohydramnios, firstborn status (tight uterine wall), extended-leg position |
| Cultural / Postnatal | Swaddling with hips in extension dramatically increases risk (Navajo); carrying babies with hips abducted is protective |
| Sex | Female:Male = 5:1 (hormonal + ligamentous laxity) |
| Racial | Higher in white/Caucasian and Navajo populations; lower in Chinese and African populations |
2B. Associated Conditions
- Congenital muscular torticollis (8% co-occurrence)
- Metatarsus adductus
- Talipes calcaneovalgus
- Ligamentous hyperlaxity syndromes
2C. Why DDH Persists into Adulthood
Mild forms (borderline or low-grade dysplasia) produce no symptoms in childhood. The hip is loaded increasingly through adolescence and adulthood; at some point the reduced articular contact area can no longer sustain normal joint reactive forces, and symptoms begin - typically in the second to fifth decade of life.
3. PATHOLOGY & PATHOANATOMY
Adult DDH involves a characteristic set of structural abnormalities across three compartments:
3A. Acetabulum
- Shallow socket: acetabulum less than a hemisphere; the "dish" is too flat
- Reduced anterior and lateral coverage of the femoral head
- Increased acetabular index (Tönnis angle) above normal (>10°)
- Reduced lateral center-edge (LCE) angle (<20°)
- Superolateral subluxation of the femoral head with high articular contact stresses concentrated at the superolateral rim
- Broadened radiographic teardrop: the hip center is lateralized
3B. Proximal Femur
- Coxa valga: increased neck-shaft angle
- Increased femoral anteversion: the femoral neck points abnormally forward
- Small, flattened femoral head with a lateral contour deficiency
- Cam morphology (increased alpha angle) co-exists in 10-40% of dysplastic hips and can cause FAI after surgical correction if not addressed
3C. Soft Tissue Changes
- Labral hypertrophy / tear: the labrum compensatorily enlarges to increase functional coverage; it is then subjected to high tensile stress and tears
- Capsular laxity: chronic instability stresses the capsule
- Shortened abductor musculature (gluteus medius/minimus) with altered lever arm
- Psoas tendon contracture
3D. Consequences: Pathological Cascade
The reduced contact area at the superolateral rim concentrates joint reactive forces. This leads to:
- Labral tear and degeneration
- Cartilage delamination at the superolateral acetabulum
- Progressive subchondral damage
- Osteoarthritis (commonly by age 45-65 if LCE angle <16°)
4. CLASSIFICATION: CROWE SYSTEM
The Crowe classification is the standard system for grading adult DDH severity based on the degree of femoral head subluxation on AP pelvis X-ray:
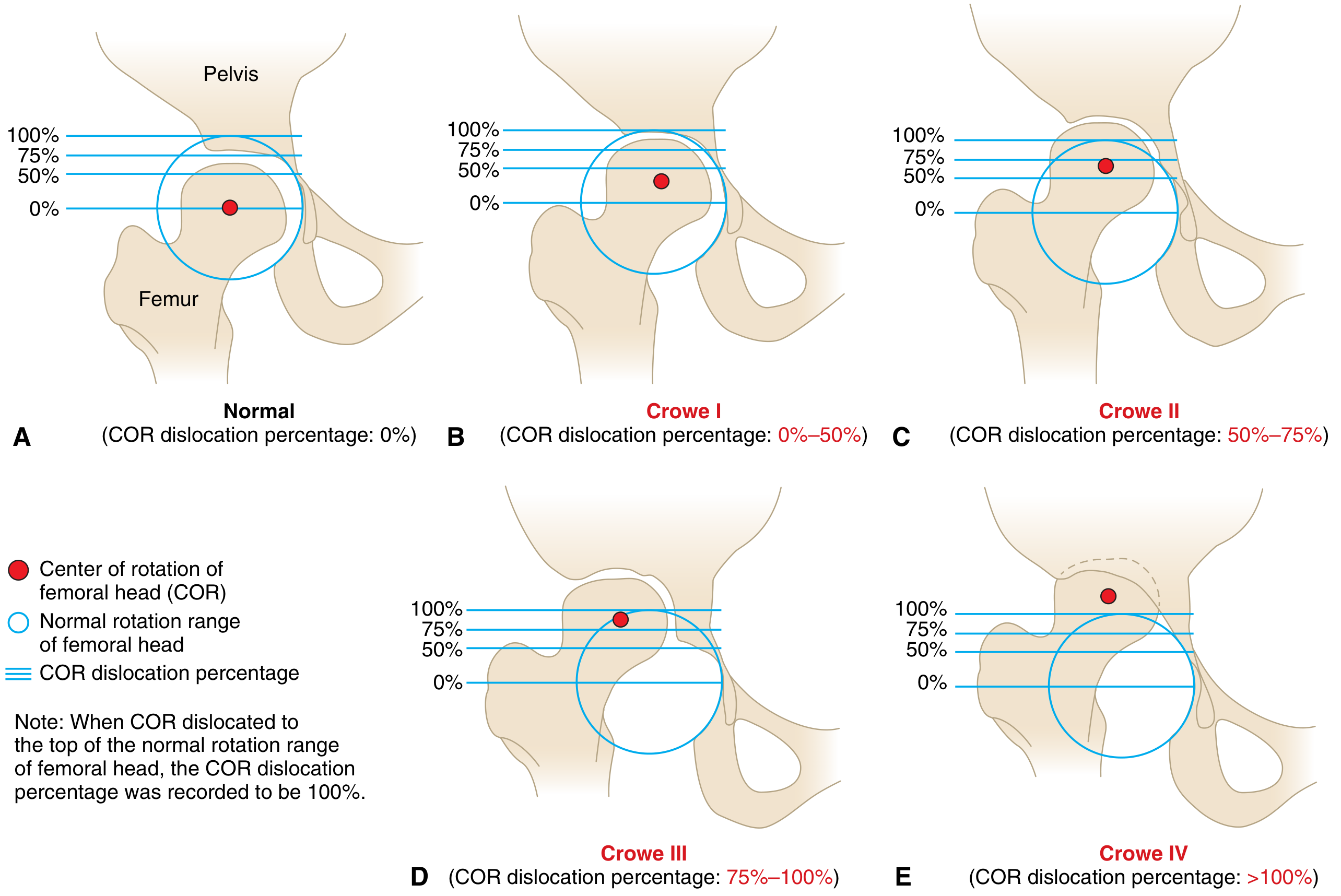
Crowe Classification for Adult DDH - Miller's Review of Orthopaedics 9th Ed, Fig. 5.2
| Grade | Femoral Head Subluxation | Proximal Displacement |
|---|---|---|
| Crowe I (mild) | <50% | <10% |
| Crowe II | 50-75% | 10-15% |
| Crowe III | 75-100% | 15-20% |
| Crowe IV (severe) | >100% | >20%; true acetabulum deficient |
The percentage is measured as displacement of the center of rotation (COR) relative to the femoral head diameter.
5. SIGNS & SYMPTOMS
5A. Clinical Presentation
Patients with adult DDH become symptomatic between their second and fifth decades. Symptoms correlate with the degree of dysplasia and labral/chondral damage.
Early / Mild DDH:
- Groin pain with activity - initially only with high-stress activities (running, prolonged standing), later with activities of daily living
- Mechanical symptoms: clicking, catching, giving-way of the hip
- Anterior groin ache - from labral tear and capsular stress
Moderate / Advanced DDH:
- Constant groin and lateral hip pain
- Limping / Trendelenburg gait: abductor weakness from altered lever arm leads to a positive Trendelenburg sign; in bilateral DDH, a waddling gait
- Leg length discrepancy (affected side shorter in subluxated/dislocated hips)
- Fatigue easily with walking
- Reduced hip range of motion, especially internal rotation and abduction
- Lumbar spine pain: compensatory hyperlordosis and spinal overload
5B. Special Clinical Tests
| Test | Method | Positive if |
|---|---|---|
| FADIR test (Flexion-Adduction-Internal Rotation) | Supine; flex hip 90°, adduct, internally rotate | Groin pain = labral tear / intra-articular pathology |
| Anterior Apprehension Test | Patient supine at edge of table; hip extended and externally rotated | Apprehension/pain = anterior capsule deficiency, dysplasia |
| Trendelenburg Sign | Single-leg stance on affected side | Pelvis drops contralaterally = abductor insufficiency |
| Thomas Test | Supine, flex one knee to chest; watch contralateral hip | Flexion contracture of ipsilateral hip |
| Log Roll Test | Supine, passive internal/external rotation | Pain with internal rotation = intra-articular pathology |
6. RADIOGRAPHIC MEASUREMENTS (KEY PARAMETERS)
The following AP pelvis radiograph demonstrates the key measurements used in DDH evaluation:
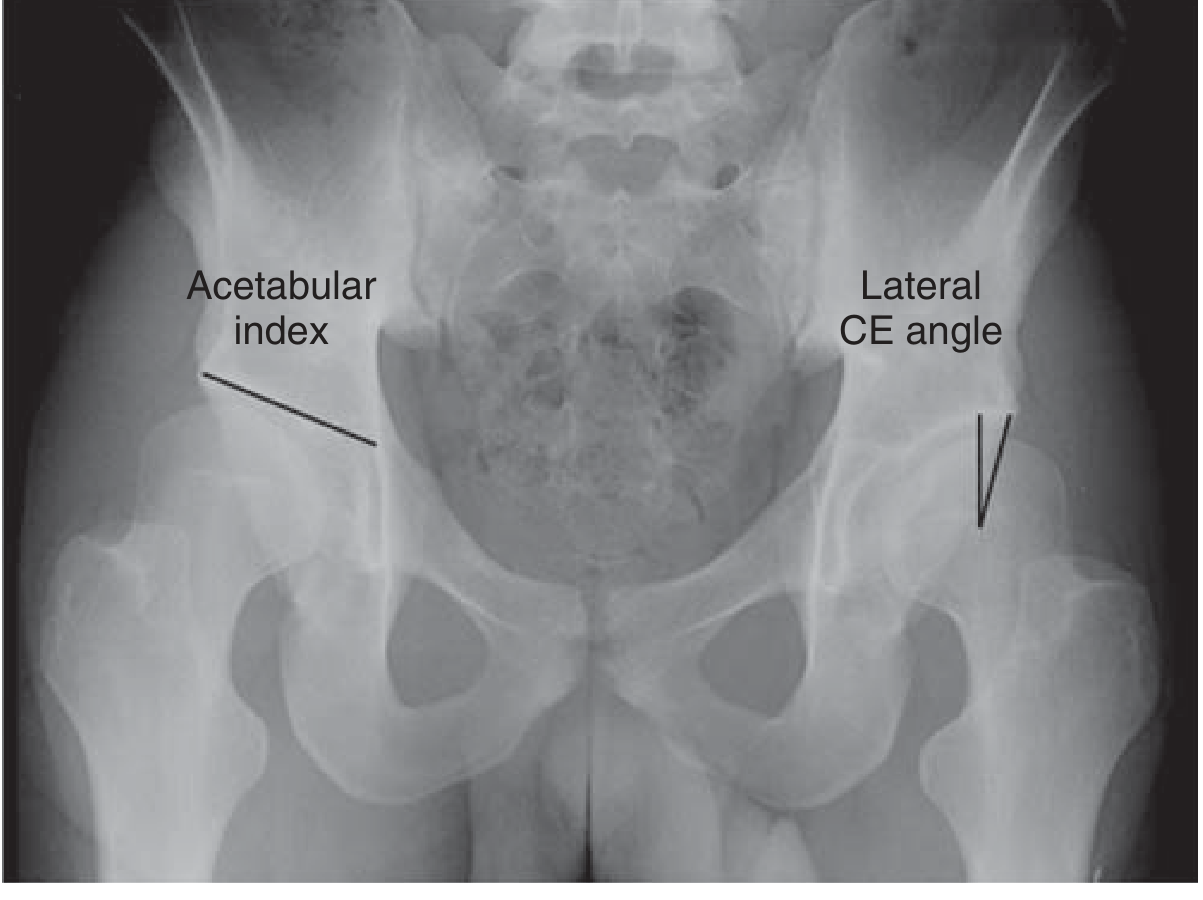
AP pelvis showing acetabular index and lateral CE angle - both hips dysplastic (Miller's Review of Orthopaedics 9th Ed, Fig. 5.1)
Key Radiographic Parameters for DDH Diagnosis
| Parameter | Normal | Dysplastic |
|---|---|---|
| Lateral Center-Edge (CE) Angle | 25-35° | <20° (borderline 20-25°) |
| Anterior CE Angle (false profile view) | >25° | <20° |
| Acetabular Index (Tönnis angle) | ~0° | >10° |
| Shenton's Line | Continuous arc | Disrupted in subluxation |
| Neck-shaft angle | 125-135° | Increased (coxa valga) |
The X-ray below shows disrupted Shenton line indicating superior subluxation - a hallmark of significant dysplasia:
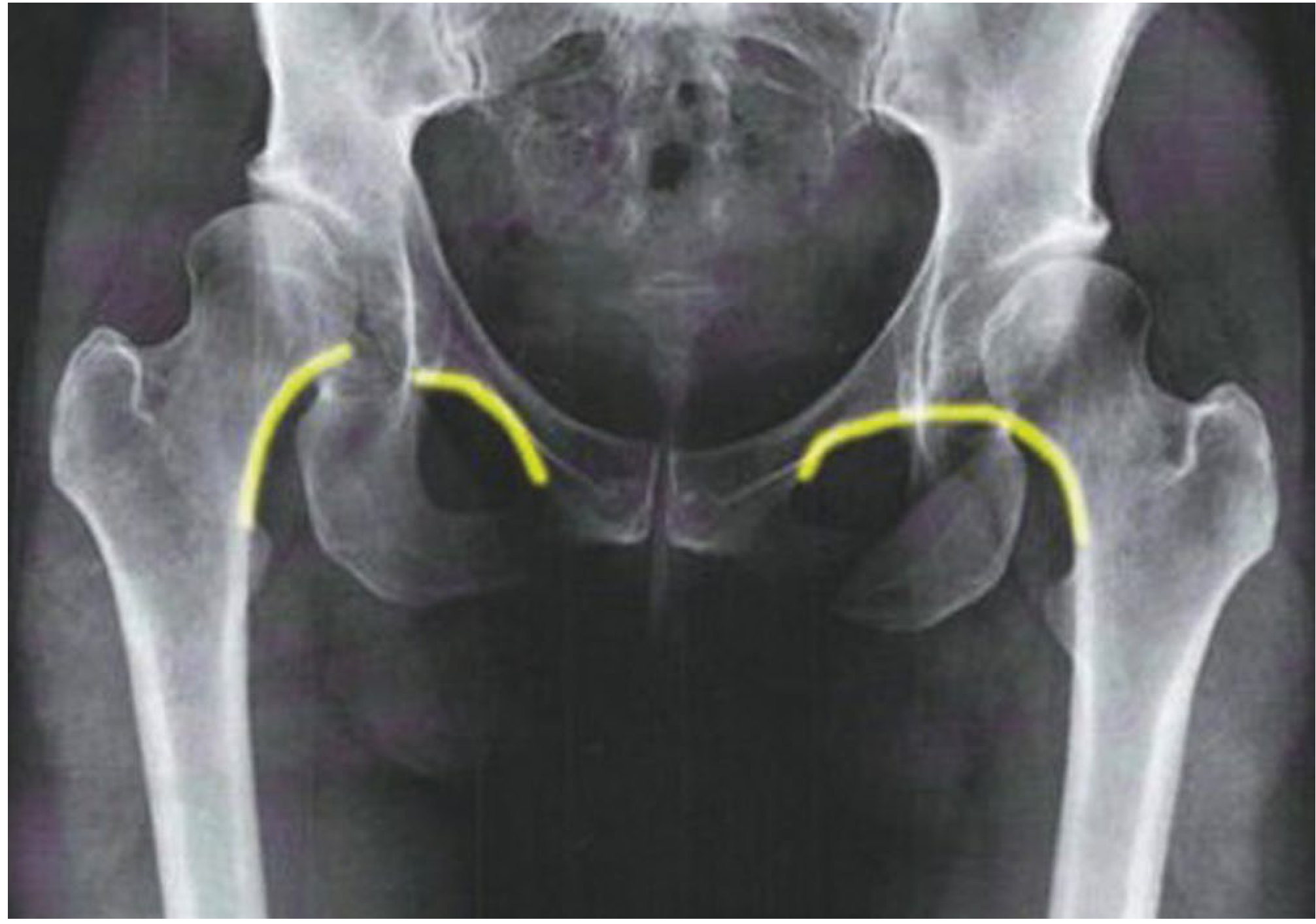
Disrupted Shenton line - indicating subluxation of femoral head - Campbell's Operative Orthopaedics, Fig. 7.36
7. INVESTIGATIONS & EVALUATION
7A. Plain Radiography (First Line)
Views required:
- Standing AP pelvis - assess CE angle, acetabular index, Shenton line, Tönnis OA grade, lateralization
- False profile view (Lequesne) - assess anterior CE angle and anterior coverage
- AP pelvis with hip in abduction and slight flexion - simulates correction achievable with PAO; tests congruence
Radiographic features of adult DDH:
- LCE angle <20°
- Tönnis angle >10°
- Lateralized hip center with broadened teardrop
- Disrupted Shenton line
- Elevated Tönnis OA grade
- Coxa valga (increased neck-shaft angle)
- Excessive femoral anteversion (visible on AP)
7B. MR Arthrography (Gold Standard for Cartilage/Labrum)
- Gadolinium intra-articular contrast injection followed by MRI
- Best modality to assess labral tears and cartilage delamination
- Identifies which patients still have adequate joint space for hip-preservation surgery vs. those requiring THA
- Typical findings in adult DDH: posterosuperior labral hypertrophy with tear at the superolateral acetabulum, chondral delamination
7C. Low-Dose CT Scan
- Assess acetabular and femoral version (combined anteversion is key surgical planning data)
- Identify femoral neck morphology and neck-shaft angle
- Plan osteotomy level for shortening procedures (Crowe III/IV)
- A few dedicated slices through the femoral epicondyles allow measurement of femoral anteversion
7D. Ultrasound
- Primary role in neonatal screening (Graf classification), not typically used for adult evaluation
- Can image the labrum and iliopsoas tendon in adults but MR arthrogram is superior
7E. Tönnis Grading of OA (Treatment Guide)
| Grade | Findings | Implication |
|---|---|---|
| 0 | Normal | Hip preservation candidate |
| 1 | Mild sclerosis, slight joint space narrowing, no cysts | Hip preservation candidate |
| 2 | Moderate cysts, moderate narrowing | Borderline - assess carefully |
| 3 | Severe narrowing, large cysts, head deformity | THA (not PAO) |
PAO is generally indicated for Tönnis grade 0-1; outcomes decline significantly at grade 2+.
8. TREATMENT
Treatment depends on:
- Patient's skeletal maturity and age
- Degree of dysplasia (Crowe grade)
- Degree of OA (Tönnis grade)
- Femoral head sphericity and joint congruence
- Specific anatomic deformity (acetabular vs. femoral vs. combined)
8A. Conservative (Non-Surgical) Management
Indicated for:
- Mild dysplasia without significant symptoms
- Patients with severe OA not yet ready for surgery
- Temporary symptom management
Options:
- Activity modification: avoid impact activities (running, jumping)
- Physical therapy: hip abductor strengthening, gait training, core stabilization
- NSAIDs for pain
- Intra-articular corticosteroid or hyaluronic acid injections: short-term symptomatic relief; also useful as a diagnostic tool to confirm intra-articular source of pain
8B. Hip Preservation: Periacetabular Osteotomy (PAO) - Bernese PAO
The Bernese PAO (Ganz osteotomy) is the gold-standard hip-preserving procedure for adult DDH in patients with:
- Tönnis grade 0-1 (or mild grade 2)
- Spherical femoral head with good joint congruence
- Skeletal maturity (typically age 15-45)
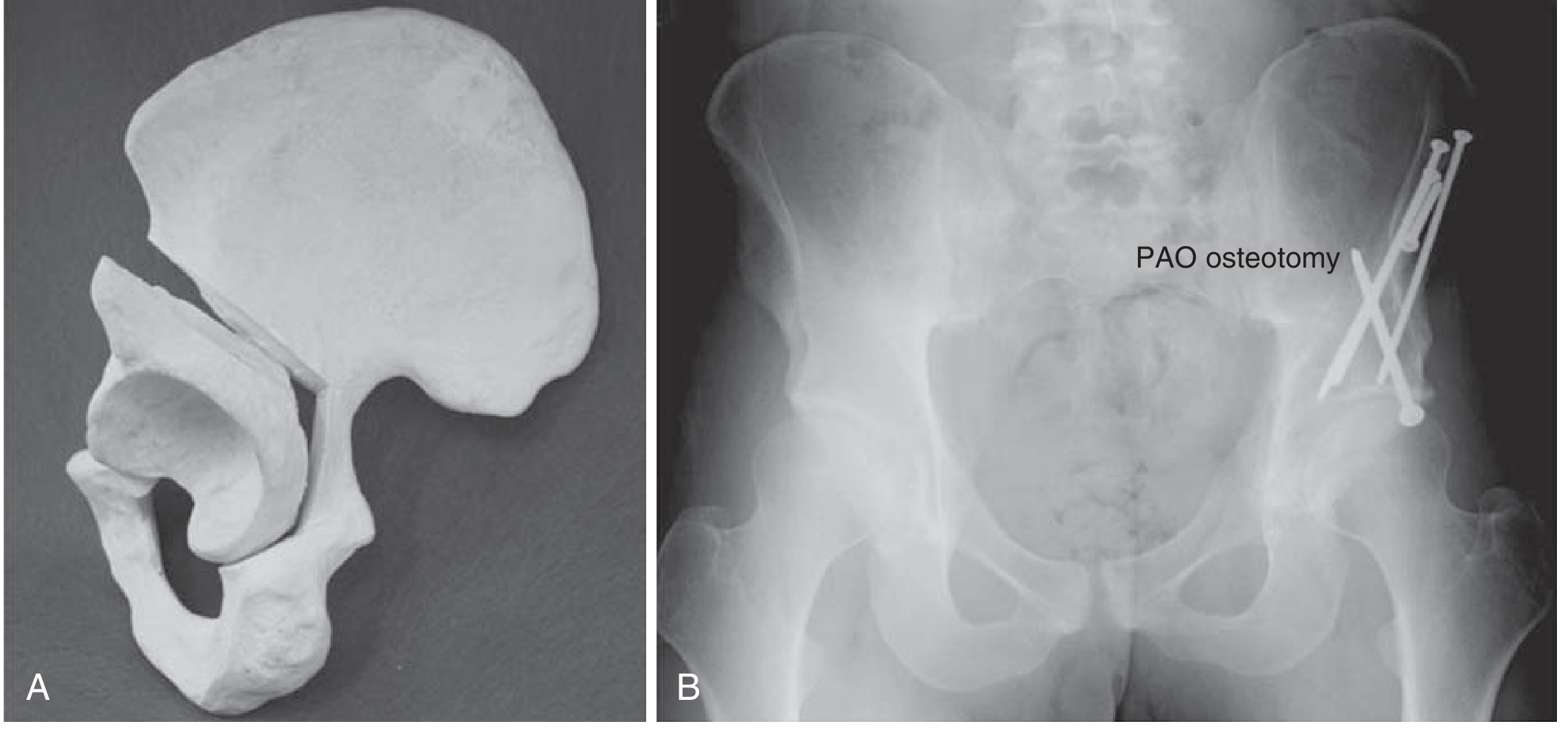
Periacetabular Osteotomy (PAO) - (A) model, (B) postoperative X-ray - Miller's Review of Orthopaedics 9th Ed, Fig. 5.3
Principle of PAO:
Four bony cuts are made around the acetabulum (ischium, pubis, ilium, quadrilateral plate) while preserving the posterior column - this maintains pelvic stability and allows early weight bearing. The freed acetabular fragment is then rotated to:
- Increase lateral coverage (normalize CE angle)
- Normalize the acetabular index to 0°
- Restore appropriate socket anteversion
- Medialize the center of rotation (reduces joint reactive forces)
Surgical Goals:
- Acetabular index → 0°
- Lateral CE angle → 25-35° (normalize, do NOT overcorrect)
- Avoid retroversion (overcorrection causes secondary FAI)
- Address concomitant cam morphology with femoral osteochondroplasty if needed
Outcomes:
- Good-to-excellent long-term results in appropriately selected patients
- Hip joint preservation: 73-76% at >9 years, 60% at 20 years, 29% at 30 years
- Survival is best in Tönnis grade 0 with a spherical, congruent head
Combined procedures sometimes needed:
- Intertrochanteric varus osteotomy for coxa valga (to address femoral side deformity)
- Femoral osteochondroplasty (for cam FAI)
- Hip arthroscopy (labral repair, chondral debridement)
8C. Hip Arthroscopy
Used for:
- Isolated labral tears in mild dysplasia without significant structural undercoverage
- Caution: arthroscopy alone in significant dysplasia without addressing the underlying instability can worsen outcomes; it must be carefully selected
8D. Total Hip Arthroplasty (THA)
Indicated when:
- Tönnis grade 2-3 (advanced OA)
- Severe dysplasia (Crowe III/IV) with no viable joint preservation
- Older age (typically >50 years, but depends on functional demands)
- Failed previous preservation surgery
Challenges specific to DDH in THA:
| Issue | Solution |
|---|---|
| Small, shallow true acetabulum | Small-diameter cementless cups; anatomic cup placement at true acetabulum |
| High-riding femoral head | Subtrochanteric shortening osteotomy (Crowe III/IV) to bring femur down to true acetabulum without stretching neurovascular structures |
| Increased femoral anteversion | Custom or modular stems; adjust combined anteversion |
| Coxa valga | Calcar-restoring stem; femoral osteotomy if needed |
| Soft tissue contracture | Careful release; sciatic nerve monitoring |
Subtrochanteric shortening osteotomy is standard practice for Crowe III and IV DDH during THA - femoral head resection, cup placed at true acetabulum, then the femur is shortened and an intramedullary nail or stem is passed across the osteotomy site.
9. SURGICAL DECISION ALGORITHM
Adult hip pain with suspected DDH
↓
AP pelvis + false profile X-rays
↓
CE angle <20°, Tönnis angle >10°?
↓
Yes → MR arthrogram + CT (version/anatomy)
↓
┌─────────────────────────────────────────────────────┐
│ Tönnis 0-1 + Spherical head + Age <45-50 │
│ → Bernese PAO (+ femoral osteotomy if coxa valga) │
└─────────────────────────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────┐
│ Tönnis 2-3 OR severe OA OR failed PAO OR Age >50 │
│ → Total Hip Arthroplasty (± shortening osteotomy) │
└─────────────────────────────────────────────────────┘
10. NATURAL HISTORY (UNTREATED)
- Hips with LCE angle <16° routinely develop significant osteoarthritis by age 65
- Progressive labral tear → chondral delamination → joint space loss
- Eventual severe OA requiring THA
- Bilateral DDH leads to characteristic waddle, early disability, and profound quality-of-life impact
11. SUMMARY TABLE
| Feature | Details |
|---|---|
| Definition | Spectrum: acetabular undercoverage → subluxation → dislocation |
| Peak symptom onset | 2nd to 5th decade |
| Gold standard investigation | MR arthrogram (labrum/cartilage) + AP pelvis X-ray (CE angle) |
| Key radiographic parameter | Lateral CE angle <20° = dysplasia |
| Classification | Crowe I-IV (degree of femoral head subluxation) |
| Hip preservation surgery | Bernese PAO (gold standard for Tönnis 0-1) |
| Arthroplasty | THA ± subtrochanteric shortening osteotomy (Crowe III/IV) |
| Primary complication if untreated | Premature osteoarthritis |
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapters 7 & 32
- Miller's Review of Orthopaedics 9th Ed, Chapter 5
- Bailey and Love's Short Practice of Surgery 28th Ed, Chapter 39
- StatPearls - DDH (2024)
- MDPI - DDH Etiopathogenesis Review
This is a shared conversation. Sign in to Orris to start your own chat.