Childhood schizophrenia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"childhood schizophrenia" OR "early-onset schizophrenia"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content to write a thorough response. Let me compile everything.
Childhood-Onset Schizophrenia (COS)
Definition and Epidemiology
Childhood-onset schizophrenia (COS) is defined as schizophrenia with onset before age 13 (some texts use before 17); onset before 5 is virtually nonexistent. It is a rare condition - incidence is less than 1 in 10,000 - making it far less common than adult schizophrenia. There is a slight male predominance (M:F ratio approximately 1.67:1). COS is considered a more severe form of the disease, with higher rates of premorbid abnormalities and a generally worse prognosis than adult-onset schizophrenia.
- Kaplan and Sadock's Synopsis of Psychiatry, p. 669
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 10891
Etiology and Risk Factors
Genetic factors dominate. A family history of schizophrenia is markedly increased in COS. Healthy siblings of COS patients show gray matter deficits in left prefrontal and bilateral temporal cortices, suggesting familial/trait markers.
Neurodevelopmental factors:
- Premorbid delays in motor milestones and language acquisition (resembling autism spectrum disorder features) are common
- Prenatal and perinatal complications are not specifically increased (unlike ASD)
- Exaggerated neuronal pruning is implicated in pathogenesis
- COMT gene polymorphism may modulate frontal deficits
Environmental risk factors: Psychosocial/family stressors (high expressed emotion - "high EE" families) are known to influence relapse rate.
Pathophysiology and Neuroimaging
COS shows more severe neurobiological changes than adult schizophrenia, making it a valuable model for studying schizophrenia neurobiology:
Gray and white matter:
- Smaller total brain volume (even more dramatic than in adults)
- Progressive loss of gray and white matter in periventricular regions: posterior cingulate, caudate, thalamus
- Slower growth of parietal white matter
- Reduced fractional anisotropy in the cuneus (also seen in healthy siblings)
Prefrontal cortex / insula / temporal lobe:
- Lower NAA (neuronal marker) and reduced gray matter in frontal and anterior cingulate cortices
- Smaller right and left insula volumes; right insula inversely correlates with positive symptoms
- Smaller superior temporal gyrus volumes - correlate with symptom severity; normalize somewhat after pharmacotherapy
- Siblings show reduced activation of frontal and striatal regions (cortical-striatal dysfunction as a liability marker)
Hippocampus and amygdala:
- Significant bilateral hippocampal volume deficit (~9-10%), persisting from age 9-26
- Anterior hippocampal inward deformation correlates with positive symptoms
- Amygdala-hippocampal volume reduction found in patients AND unaffected relatives
Subcortical structures:
- Increased caudate volume (partly due to typical neuroleptic exposure - normalizes with clozapine)
- Decreased thalamic volume - one of the most consistent findings in psychotropic-naïve patients
The figure below from the NIMH longitudinal study demonstrates progressive gray matter loss in COS compared to healthy controls:
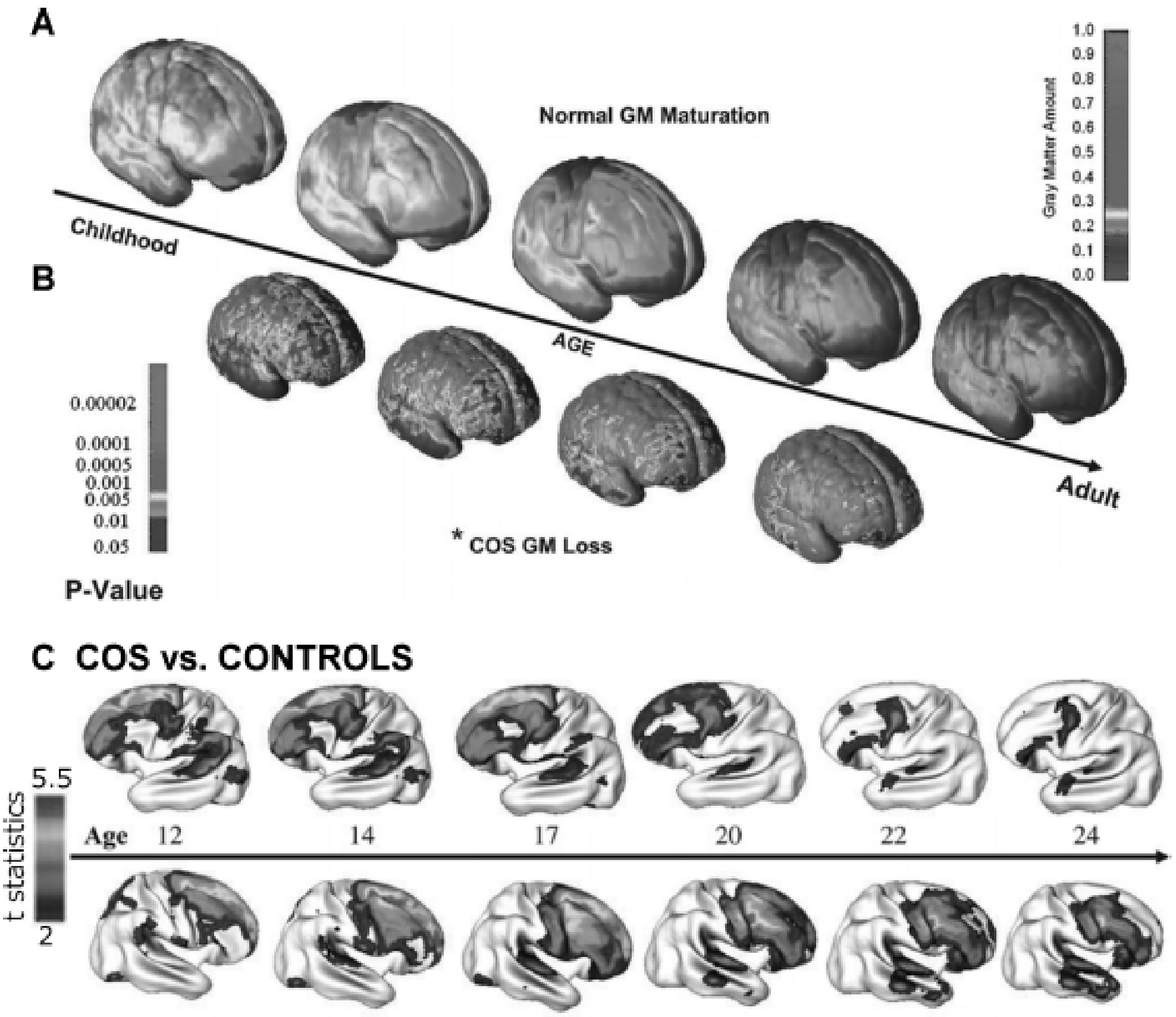
FIGURE: Right lateral views of (A) normal gray matter maturation in healthy youth ages 4-22, (B) global gray matter loss in COS vs. controls, and (C) progressive GM deficits in COS from ages 12 to 24 - showing that COS follows an exaggerated form of normal cortical maturation. - Kaplan & Sadock's Comprehensive Textbook, p. 10892
Clinical Features
All symptoms seen in adult schizophrenia can occur in children, but presentation differs based on developmental level:
Positive Symptoms
Hallucinations are the most common feature:
- Auditory hallucinations predominate - voices may offer running commentary, command the child to harm themselves or others, or sound like "a computer in my head," "Martians," or familiar relatives
- The NIMH COS project found unexpectedly high rates of tactile, olfactory, and visual hallucinations - visual ones (seeing devils, skeletons, scary faces) are associated with lower IQ and earlier onset
- Visual, tactile, and olfactory hallucinations are markers of more severe psychosis
Delusions occur in up to 50% of children and adolescents:
- Types: persecutory, grandiose, religious
- Content is developmentally influenced - young children have simpler delusions featuring age-appropriate fears (monsters, animals); older children develop more complex ones
- Frequency increases with age
Thought disorder:
- Loosening of associations, thought blocking, illogical thinking, poverty of thought
- Unlike adults, children do NOT show poverty of speech content but speak less and communicate more ambiguously
- Failure to self-correct (no self-initiated repair) is a distinctive communication deficit
Negative Symptoms
- Blunted or inappropriate affect (near universal) - giggling for no reason, crying inexplicably
- Avolition, apathy, social withdrawal
- Academic and social decline
Premorbid Features
- Social rejection, poor peer relationships, clingy/withdrawn behavior
- Academic difficulties
- Some children show delayed motor milestones and language acquisition similar to ASD
- Comorbid ADHD and conduct disorder are common
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Autism Spectrum Disorder (ASD) | Early developmental onset; poor social relatedness; stereotypies; no hallucinations/delusions as core features; seizures in 4-32%; no family history of schizophrenia |
| Bipolar I Disorder | 1/3 of children initially diagnosed COS are later rediagnosed with bipolar disorder in adolescence; better long-term prognosis |
| Substance-induced psychosis | Amphetamines, LSD, PCP can cause paranoid psychosis; sudden flagrant onset is a clue |
| Medical causes | Thyroid disease, SLE, temporal lobe epilepsy |
| Anxiety/PTSD | Anxious children can have quasi-delusional thinking; PTSD flashbacks can mimic hallucinations |
| Depression/mania | Mood disorders can include nihilistic/grandiose delusions |
| Intellectual disability | Global impairments in verbal and nonverbal; relates socially per mental age |
- Kaplan and Sadock's Synopsis of Psychiatry, p. 404 (Table 2-13)
Course and Prognosis
COS generally carries a guarded prognosis - worse than adult-onset schizophrenia. Key predictors:
Poor prognostic factors:
- Early age of onset and insidious onset
- Family history of schizophrenia
- Premorbid developmental delays, lower IQ, lower functioning
- Comorbid ADHD or conduct disorder
- Long or chronic first psychotic episode
- High expressed emotion (high EE) in the family
Moderating factors: Response to pharmacological and psychosocial interventions, degree of remission after first episode, degree of family support.
The NIMH Treatment of Early-Onset Schizophrenia study (comparing molindone, olanzapine, and risperidone) found modest but significant improvement in neurocognitive functioning with antipsychotic treatment over 1 year, with no significant differences among the three agents.
Treatment
Treatment requires a multimodal approach.
Psychosocial Interventions
- Psychoeducation for families - ongoing family therapeutic interventions are critical; high EE predicts relapse
- CBT - effective component of integrated psychological intervention (IPI)
- Group skills training and cognitive remediation therapy
- Multifamily psychoeducation
- Appropriate educational placement - addressing frequent social skills deficits, attention deficits, and academic difficulties
- An RCT of integrated psychological interventions (IPI) in early prodromal youth was more effective than standard treatment in delaying psychosis onset over 2 years
Pharmacotherapy
Second-generation antipsychotics (SGAs) are the first-line treatment. Six RCTs support their efficacy in early-onset schizophrenia, with limited evidence favoring one agent over another.
| Agent | Notes |
|---|---|
| Risperidone | FDA-approved for schizophrenia in adolescents; increases frontal activation (unlike typicals) |
| Olanzapine | Compared to clozapine in a double-blind RCT; significant weight gain concern |
| Aripiprazole | FDA-approved for adolescents |
| Quetiapine | Used in practice; sedation profile can be limiting |
| Lurasidone | FDA-approved for adolescents (2017) |
| Paliperidone | FDA-approved for adolescents (2017) |
| Clozapine | Most effective for positive AND negative symptoms, but last resort due to side effects (agranulocytosis, seizures, metabolic effects); normalizes caudate volume after switching from typicals |
Important caveats in children:
- Children have less robust responses to antipsychotics than adolescents and adults
- Use the lowest effective dosage - children are more vulnerable to side effects
- Greater vulnerability to extrapyramidal symptoms (EPS) with D2 antagonists
- Greater risk of weight gain and metabolic abnormalities with SGAs
- Antipsychotic drugs may impair learning in this population
- Typical neuroleptics decrease frontal cortical activation; atypicals (e.g., risperidone) increase frontal activation
Key Comparison: COS vs. ASD
| Feature | ASD | COS (before puberty) |
|---|---|---|
| Age of onset | Early developmental | Rarely under age 5 |
| Incidence | ~1% | <1 in 10,000 |
| M:F ratio | 4:1 | 1.67:1 |
| Family Hx of schizophrenia | Not increased | Increased |
| Perinatal complications | Increased | Not increased |
| Core symptoms | Poor social relatedness, stereotypies, language abnormalities | Hallucinations, delusions, thought disorder |
| Adaptive functioning | Impaired | Deterioration from baseline |
| IQ | Wide range; 30% intellectually disabled | Usually normal/low average |
| Seizures | 4-32% | Low incidence |
- Kaplan and Sadock's Synopsis of Psychiatry, p. 404
Sources:
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (10th ed.), Chapter 37, pp. 10891-10894
- Kaplan and Sadock's Synopsis of Psychiatry, pp. 669-676
This is a shared conversation. Sign in to Orris to start your own chat.