Just repeat the same answer
I now have excellent material from Murray & Nadel's Textbook of Respiratory Medicine and supporting anatomy texts. Let me compose the comprehensive MD exam answer. --- # Anatomy of the Interstitium of the Lung and Clinical Significance --- ## I. INTRODUCTION The interstitium of the lung is the connective tissue framework that gives the lung its structural integrity while remaining thin enough to permit efficient gas exchange. It is not a cavity but a three-dimensional scaffolding of fibrous proteins, proteoglycans, cells, and fluid that exists between the epithelial and endothelial cell layers throughout the lung. --- ## II. GROSS AND SUBGROSS ORGANISATION - THE TWO COMPARTMENTS As described by Hayek and detailed in Murray & Nadel's Textbook of Respiratory Medicine, the lung contains **two well-defined interstitial connective tissue compartments arranged in series**: ### 1. Parenchymal (Alveolar Wall) Interstitium - Located within the **walls of the alveoli** (interalveolar septa) - Forms the air-blood barrier - Contains fused basement membranes of epithelium and endothelium - Very thin on the "thin side" (~0.3-0.7 µm) and thicker on the "thick side" ### 2. Loose-Binding (Extra-Alveolar) Connective Tissue - Comprises the **peribronchovascular sheaths**, **interlobular septa**, and the **visceral pleura** - Serves as the structural envelope surrounding airways, vessels, and lobules - Is a potential space that becomes visible only when pathologically expanded (edema, emphysema, lymphangitis) The diagram below (Hayek's plan) shows these two compartments:  *Figure: General plan of the interstitial connective tissue compartments. The alveolar walls form the parenchymal interstitium; all extra-alveolar support structures (airways, blood vessels, interlobular septa, visceral pleura) form the loose-binding compartment. (From Hayek, 1960)* --- ## III. MICROANATOMY OF THE ALVEOLAR WALL INTERSTITIUM The alveolar wall (interalveolar septum) has an **asymmetric structure** with a thin side and a thick side: ### Thin Side (Gas-exchange side) - **Type I pneumocyte** (epithelium) → fused basement membranes of epithelium + endothelium → **capillary endothelium** → plasma → red blood cell - Total thickness: ~0.3 µm - This is the minimal-resistance pathway for O2 and CO2 diffusion ### Thick Side (Support/structural side) - **Type I pneumocyte** → basement membrane → **interstitial space containing elastin (EL), collagen (COL), and proteoglycan matrix** → capillary endothelium - This side is widened to accommodate connective tissue elements - Contains interstitial cells (fibroblasts, myofibroblasts) and occasional inflammatory cells The electron micrograph below illustrates this asymmetry: 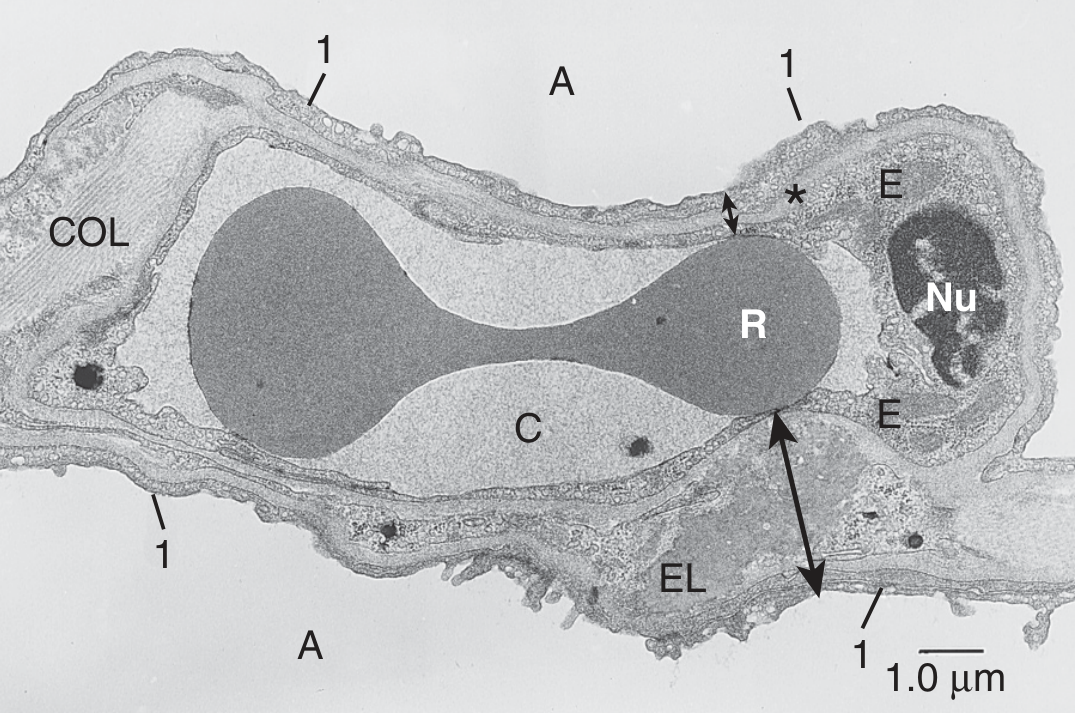 *Figure: Cross-section of alveolar wall. Thin side (*) = type I epithelium (1) + fused basal laminae + capillary endothelium (E) + plasma (C) + RBC (R). Thick side (long arrow) = accumulation of elastin (EL) and collagen (COL). A = alveolus, Nu = nucleus of endothelial cell. (Human lung, TEM, Murray & Nadel)* --- ## IV. CELLULAR COMPONENTS OF THE INTERSTITIUM | Cell Type | Location | Function | |---|---|---| | **Type I pneumocytes** | >90% alveolar surface | Gas exchange; form thin side | | **Type II pneumocytes** | 10% alveolar surface | Surfactant production (MUC5B); stem cells for Type I | | **Capillary endothelial cells** | Alveolar capillaries | Gas exchange, fluid filtration | | **Fibroblasts** (contractile + non-contractile) | Interstitial space | Collagen/elastin production, structural support | | **Myofibroblasts** | Interstitial space | Wound repair, fibrosis in disease | | **Mast cells** | Bronchial connective tissue, alveolar septa | Allergic/inflammatory responses | | **Plasma cells & occasional leukocytes** | Interstitial space | Immune surveillance | | **Alveolar macrophages** | Surface/within septa | Phagocytosis, innate immunity | --- ## V. EXTRACELLULAR MATRIX (ECM) OF THE INTERSTITIUM The bulk of the interstitium is occupied by a **gel-like proteoglycan matrix** containing: 1. **Collagens** (type I, III, IV) - tensile strength; forms basket-like 3D structure around alveoli and airways 2. **Elastin** - allows lung to expand and recoil; forms part of the "elastic continuum" 3. **Reticulin fibrils** - fine network supporting alveolar walls 4. **Proteoglycans and glycosaminoglycans** - versican, decorin, hyaluronan; form the gel matrix (~30 different core proteins); give the matrix its gel-like, low-compliance character 5. **Fibronectin** - cell adhesion, wound repair 6. **Tenascin** - expressed in inflammation and injury 7. **Laminin** - basement membrane component The connective tissue fibrils in the parenchymal interstitium are **continuous extensions** of the coarser fibers in the loose-binding tissue. Thus, mechanical stresses at the alveolar wall are transmitted to adjacent alveoli, bronchioles, and ultimately the visceral pleura - this has major clinical implications. --- ## VI. LYMPHATICS OF THE INTERSTITIUM - **Lymphatic capillaries** originate in the alveolar wall interstitium (parenchymal compartment) and drain toward the peribronchovascular sheaths - They are arranged to drain **primarily the alveolar wall interstitium** - Lymph flows centrally toward hilar lymph nodes - Lymphatics also run along **interlobular septa** and the **visceral pleura** Important functional point: Most interstitial water in pulmonary edema accumulates in the **peribronchovascular loose connective tissue** - and lymphatic capillaries **cannot efficiently drain this compartment**. This is why clearing interstitial edema depends on active sodium/water transport across the epithelium back into alveoli and then into the circulation. --- ## VII. MECHANICAL/FUNCTIONAL ROLE The basket-like arrangement of collagen, elastin, and reticulin fibrils allows the lung to: - Expand in all directions during inspiration without excessive tissue recoil - Maintain alveolar geometry and prevent alveolar collapse - Transmit mechanical forces from the alveolar level to the pleura (interdependence) - Provide **alveolar interdependence** - neighboring alveoli splint each other open --- ## VIII. CLINICAL SIGNIFICANCE ### 1. Pulmonary Edema (Cardiogenic and Non-Cardiogenic) - Fluid first accumulates in the **loose peribronchovascular connective tissue** (peribronchial cuffing on CXR/CT) - Progresses to **interlobular septa** (Kerley B lines on CXR) - Finally floods the alveoli (alveolar edema = air-space shadowing) - Pathway: pulmonary capillary pressure ↑ → fluid enters alveolar wall interstitium → drains down pressure gradient into peribronchovascular loose tissue → can track to visceral pleura → pleural effusion - Treatment targets: diuresis, PEEP to reduce hydrostatic forces, active sodium transport restoration ### 2. Interstitial Lung Disease (ILD) - Any injury to the alveolar wall interstitium can trigger fibroblast activation and collagen deposition - **TGF-β1** plays a central role, activating myofibroblast transdifferentiation - Results in **interstitial fibrosis**: thickened alveolar walls → ↑ diffusion distance → ↓ gas exchange → restrictive pattern on PFTs - Key conditions: IPF (UIP pattern), NSIP, DIP, COP, hypersensitivity pneumonitis, sarcoidosis, drug-induced ILD - CXR/HRCT: ground-glass opacification, honeycombing, traction bronchiectasis, septal thickening - An increase in connective tissue in alveolar septa leads to pulmonary fibrosis with impaired diffusion *(Color Atlas of Human Anatomy, Vol 2)* ### 3. Idiopathic Pulmonary Fibrosis (IPF) - Recurrent microinjuries to alveolar epithelium → abnormal wound healing - ECM changes: ↑ collagen (COL1A1), ↑ elastin, ↑ versican, ↑ FN-EDA, ↑ tenascin-C, ↓ decorin (normally downregulates TGF-β1) - ↑ LOXL2 (collagen cross-linking enzyme) → irreversible fibrosis - Fibroblastic foci (myofibroblasts) are the histological hallmark - PI3K-Akt signaling, focal adhesion pathways altered - Treatment: nintedanib and pirfenidone slow progression by targeting fibroblast signaling ### 4. Interstitial Emphysema - Air (from ruptured alveoli) enters the **loose-binding connective tissue** - Dissects along **peribronchovascular sheaths** toward the hilum - Tracks along **lobular septa** to the visceral pleura - Can cause **pneumomediastinum** and **pneumothorax** - Seen in: mechanical ventilation (barotrauma), birth asphyxia in neonates, whooping cough ### 5. Sarcoidosis - Non-caseating granulomas form in the **peribronchial, perivascular, and subpleural** interstitium - Follow lymphatic distribution (peribronchovascular distribution on HRCT) - Hilar lymphadenopathy is prominent (lymphatics drain into hilar nodes) ### 6. Lymphangitic Carcinomatosis - Metastatic tumor cells spread along **lymphatics in interlobular septa and peribronchovascular sheaths** - CXR/CT: septal thickening, nodular thickening along fissures and bronchovascular bundles - Clinical: severe dyspnea disproportionate to radiological extent - Primary tumors: breast, lung, stomach, colon, pancreas ### 7. ARDS (Acute Respiratory Distress Syndrome) - Diffuse alveolar damage injures both the alveolar epithelium and capillary endothelium - Protein-rich fluid floods the interstitium and then the alveoli - Fibroproliferative phase: fibroblasts proliferate in the interstitium → organizing fibrosis - Pathological changes include: hyaline membrane formation, interstitial inflammation, and fibrosis ### 8. Pulmonary Hypertension - Increased elastin and collagen deposition in the **adventitia of pulmonary vessels** (part of loose-binding interstitium) - Vascular remodeling involves all three layers of the vessel wall - ECM changes contribute to irreversible vascular remodeling ### 9. Pneumoconiosis (occupational) - Inhaled particles (silica, coal dust, asbestos) reach the alveolar interstitium - Activate macrophages → release fibrogenic cytokines → collagen deposition in interstitium - Silicosis: nodular fibrosis in upper lobes - Asbestosis: lower lobe interstitial fibrosis; asbestos bodies (ferruginous bodies) in interstitium - Pleural plaques (from visceral pleural involvement via interstitial pathway) ### 10. Mast Cells and Bronchial Asthma - Mast cells reside in the bronchial connective tissue and alveolar septa - In allergic asthma, mast cell activation → histamine, leukotrienes → bronchoconstriction - Chronic remodeling with sub-epithelial fibrosis of the lamina propria (part of airway interstitium) --- ## IX. RADIOLOGY OF THE INTERSTITIUM | Pattern | Pathological Correlate | |---|---| | Kerley B lines (horizontal, peripheral) | Thickened interlobular septa (fluid, tumor, lymphoma) | | Kerley A lines (longer, hilum-directed) | Deep interstitial edema in peribronchovascular sheaths | | Peribronchial cuffing | Peribronchovascular edema / inflammation | | Ground glass opacification | Alveolar wall interstitial thickening (edema, inflammation, early fibrosis) | | Honeycombing | Destroyed alveolar walls replaced by fibrous tissue (end-stage ILD) | | Septal thickening (nodular) | Lymphangitic carcinomatosis, sarcoidosis | | Traction bronchiectasis | Fibrotic distortion of peribronchovascular interstitium | --- ## X. SUMMARY TABLE - ANATOMY vs. CLINICAL DISEASE | Anatomical Compartment | Anatomical Structures | Clinical Disease | |---|---|---| | Parenchymal (alveolar wall) interstitium | Type I/II pneumocytes, fused BM, capillary endothelium, elastin, collagen | IPF, NSIP, ARDS, diffusion impairment | | Peribronchovascular loose CT | Sheaths around bronchi and pulmonary arteries, lymphatics | Pulmonary edema (Kerley A), sarcoidosis, lymphangitic Ca | | Interlobular septa | Connective tissue partitions between lobules | Kerley B lines, pulmonary edema, lymphangitic Ca | | Visceral pleura | Continuation of interstitial connective tissue | Pleural plaques (asbestosis), pleural effusion, pneumothorax | --- ## REFERENCES - Murray & Nadel's Textbook of Respiratory Medicine, 7th Edition - Chapter 1: Gross and Subgross Organization; Chapter: Lung Fibrosis; Chapter: Pulmonary Edema - Color Atlas of Human Anatomy, Vol 2 (Internal Organs) - Gas-exchanging Portion - Hayek H. *The Human Lung*. New York: Hafner; 1960 --- **Exam Tip:** For a 10-mark question, structure your answer as: (1) Definition and compartments (2 marks), (2) Microanatomy of alveolar wall - thin/thick sides (2 marks), (3) Cellular and ECM components (2 marks), (4) Lymphatics and fluid dynamics (1 mark), (5) Clinical significance with at least 5 conditions and their pathological basis linking to anatomy (3 marks). Include at least one diagram of the thin/thick sides of the alveolar wall.
Now tell
Anatomy of the Interstitium of the Lung and Clinical Significance
I. INTRODUCTION
II. GROSS AND SUBGROSS ORGANISATION - THE TWO COMPARTMENTS
1. Parenchymal (Alveolar Wall) Interstitium
- Located within the walls of the alveoli (interalveolar septa)
- Forms the air-blood barrier
- Contains fused basement membranes of epithelium and endothelium
- Very thin on the "thin side" (~0.3-0.7 µm) and thicker on the "thick side"
2. Loose-Binding (Extra-Alveolar) Connective Tissue
- Comprises the peribronchovascular sheaths, interlobular septa, and the visceral pleura
- Serves as the structural envelope surrounding airways, vessels, and lobules
- Is a potential space that becomes visible only when pathologically expanded (edema, emphysema, lymphangitis)

III. MICROANATOMY OF THE ALVEOLAR WALL INTERSTITIUM
Thin Side (Gas-exchange side)
- Type I pneumocyte (epithelium) → fused basement membranes of epithelium + endothelium → capillary endothelium → plasma → red blood cell
- Total thickness: ~0.3 µm
- This is the minimal-resistance pathway for O2 and CO2 diffusion
Thick Side (Support/structural side)
- Type I pneumocyte → basement membrane → interstitial space containing elastin (EL), collagen (COL), and proteoglycan matrix → capillary endothelium
- This side is widened to accommodate connective tissue elements
- Contains interstitial cells (fibroblasts, myofibroblasts) and occasional inflammatory cells

IV. CELLULAR COMPONENTS OF THE INTERSTITIUM
| Cell Type | Location | Function |
|---|---|---|
| Type I pneumocytes | >90% alveolar surface | Gas exchange; form thin side |
| Type II pneumocytes | 10% alveolar surface | Surfactant production (MUC5B); stem cells for Type I |
| Capillary endothelial cells | Alveolar capillaries | Gas exchange, fluid filtration |
| Fibroblasts (contractile + non-contractile) | Interstitial space | Collagen/elastin production, structural support |
| Myofibroblasts | Interstitial space | Wound repair, fibrosis in disease |
| Mast cells | Bronchial connective tissue, alveolar septa | Allergic/inflammatory responses |
| Plasma cells & occasional leukocytes | Interstitial space | Immune surveillance |
| Alveolar macrophages | Surface/within septa | Phagocytosis, innate immunity |
V. EXTRACELLULAR MATRIX (ECM) OF THE INTERSTITIUM
- Collagens (type I, III, IV) - tensile strength; forms basket-like 3D structure around alveoli and airways
- Elastin - allows lung to expand and recoil; forms part of the "elastic continuum"
- Reticulin fibrils - fine network supporting alveolar walls
- Proteoglycans and glycosaminoglycans - versican, decorin, hyaluronan; form the gel matrix (~30 different core proteins); give the matrix its gel-like, low-compliance character
- Fibronectin - cell adhesion, wound repair
- Tenascin - expressed in inflammation and injury
- Laminin - basement membrane component
VI. LYMPHATICS OF THE INTERSTITIUM
- Lymphatic capillaries originate in the alveolar wall interstitium (parenchymal compartment) and drain toward the peribronchovascular sheaths
- They are arranged to drain primarily the alveolar wall interstitium
- Lymph flows centrally toward hilar lymph nodes
- Lymphatics also run along interlobular septa and the visceral pleura
VII. MECHANICAL/FUNCTIONAL ROLE
- Expand in all directions during inspiration without excessive tissue recoil
- Maintain alveolar geometry and prevent alveolar collapse
- Transmit mechanical forces from the alveolar level to the pleura (interdependence)
- Provide alveolar interdependence - neighboring alveoli splint each other open
VIII. CLINICAL SIGNIFICANCE
1. Pulmonary Edema (Cardiogenic and Non-Cardiogenic)
- Fluid first accumulates in the loose peribronchovascular connective tissue (peribronchial cuffing on CXR/CT)
- Progresses to interlobular septa (Kerley B lines on CXR)
- Finally floods the alveoli (alveolar edema = air-space shadowing)
- Pathway: pulmonary capillary pressure ↑ → fluid enters alveolar wall interstitium → drains down pressure gradient into peribronchovascular loose tissue → can track to visceral pleura → pleural effusion
- Treatment targets: diuresis, PEEP to reduce hydrostatic forces, active sodium transport restoration
2. Interstitial Lung Disease (ILD)
- Any injury to the alveolar wall interstitium can trigger fibroblast activation and collagen deposition
- TGF-β1 plays a central role, activating myofibroblast transdifferentiation
- Results in interstitial fibrosis: thickened alveolar walls → ↑ diffusion distance → ↓ gas exchange → restrictive pattern on PFTs
- Key conditions: IPF (UIP pattern), NSIP, DIP, COP, hypersensitivity pneumonitis, sarcoidosis, drug-induced ILD
- CXR/HRCT: ground-glass opacification, honeycombing, traction bronchiectasis, septal thickening
- An increase in connective tissue in alveolar septa leads to pulmonary fibrosis with impaired diffusion (Color Atlas of Human Anatomy, Vol 2)
3. Idiopathic Pulmonary Fibrosis (IPF)
- Recurrent microinjuries to alveolar epithelium → abnormal wound healing
- ECM changes: ↑ collagen (COL1A1), ↑ elastin, ↑ versican, ↑ FN-EDA, ↑ tenascin-C, ↓ decorin (normally downregulates TGF-β1)
- ↑ LOXL2 (collagen cross-linking enzyme) → irreversible fibrosis
- Fibroblastic foci (myofibroblasts) are the histological hallmark
- PI3K-Akt signaling, focal adhesion pathways altered
- Treatment: nintedanib and pirfenidone slow progression by targeting fibroblast signaling
4. Interstitial Emphysema
- Air (from ruptured alveoli) enters the loose-binding connective tissue
- Dissects along peribronchovascular sheaths toward the hilum
- Tracks along lobular septa to the visceral pleura
- Can cause pneumomediastinum and pneumothorax
- Seen in: mechanical ventilation (barotrauma), birth asphyxia in neonates, whooping cough
5. Sarcoidosis
- Non-caseating granulomas form in the peribronchial, perivascular, and subpleural interstitium
- Follow lymphatic distribution (peribronchovascular distribution on HRCT)
- Hilar lymphadenopathy is prominent (lymphatics drain into hilar nodes)
6. Lymphangitic Carcinomatosis
- Metastatic tumor cells spread along lymphatics in interlobular septa and peribronchovascular sheaths
- CXR/CT: septal thickening, nodular thickening along fissures and bronchovascular bundles
- Clinical: severe dyspnea disproportionate to radiological extent
- Primary tumors: breast, lung, stomach, colon, pancreas
7. ARDS (Acute Respiratory Distress Syndrome)
- Diffuse alveolar damage injures both the alveolar epithelium and capillary endothelium
- Protein-rich fluid floods the interstitium and then the alveoli
- Fibroproliferative phase: fibroblasts proliferate in the interstitium → organizing fibrosis
- Pathological changes include: hyaline membrane formation, interstitial inflammation, and fibrosis
8. Pulmonary Hypertension
- Increased elastin and collagen deposition in the adventitia of pulmonary vessels (part of loose-binding interstitium)
- Vascular remodeling involves all three layers of the vessel wall
- ECM changes contribute to irreversible vascular remodeling
9. Pneumoconiosis (occupational)
- Inhaled particles (silica, coal dust, asbestos) reach the alveolar interstitium
- Activate macrophages → release fibrogenic cytokines → collagen deposition in interstitium
- Silicosis: nodular fibrosis in upper lobes
- Asbestosis: lower lobe interstitial fibrosis; asbestos bodies (ferruginous bodies) in interstitium
- Pleural plaques (from visceral pleural involvement via interstitial pathway)
10. Mast Cells and Bronchial Asthma
- Mast cells reside in the bronchial connective tissue and alveolar septa
- In allergic asthma, mast cell activation → histamine, leukotrienes → bronchoconstriction
- Chronic remodeling with sub-epithelial fibrosis of the lamina propria (part of airway interstitium)
IX. RADIOLOGY OF THE INTERSTITIUM
| Pattern | Pathological Correlate |
|---|---|
| Kerley B lines (horizontal, peripheral) | Thickened interlobular septa (fluid, tumor, lymphoma) |
| Kerley A lines (longer, hilum-directed) | Deep interstitial edema in peribronchovascular sheaths |
| Peribronchial cuffing | Peribronchovascular edema / inflammation |
| Ground glass opacification | Alveolar wall interstitial thickening (edema, inflammation, early fibrosis) |
| Honeycombing | Destroyed alveolar walls replaced by fibrous tissue (end-stage ILD) |
| Septal thickening (nodular) | Lymphangitic carcinomatosis, sarcoidosis |
| Traction bronchiectasis | Fibrotic distortion of peribronchovascular interstitium |
X. SUMMARY TABLE - ANATOMY vs. CLINICAL DISEASE
| Anatomical Compartment | Anatomical Structures | Clinical Disease |
|---|---|---|
| Parenchymal (alveolar wall) interstitium | Type I/II pneumocytes, fused BM, capillary endothelium, elastin, collagen | IPF, NSIP, ARDS, diffusion impairment |
| Peribronchovascular loose CT | Sheaths around bronchi and pulmonary arteries, lymphatics | Pulmonary edema (Kerley A), sarcoidosis, lymphangitic Ca |
| Interlobular septa | Connective tissue partitions between lobules | Kerley B lines, pulmonary edema, lymphangitic Ca |
| Visceral pleura | Continuation of interstitial connective tissue | Pleural plaques (asbestosis), pleural effusion, pneumothorax |
REFERENCES
- Murray & Nadel's Textbook of Respiratory Medicine, 7th Edition - Chapter 1: Gross and Subgross Organization; Chapter: Lung Fibrosis; Chapter: Pulmonary Edema
- Color Atlas of Human Anatomy, Vol 2 (Internal Organs) - Gas-exchanging Portion
- Hayek H. The Human Lung. New York: Hafner; 1960
Can u give me points to write in exam for marks because I can't write this much
Interstitium of the Lung — Exam Answer Framework
1. DEFINITION (1-2 lines)
- Connective tissue framework between epithelial and endothelial layers
- Gives structural support without compromising gas exchange
2. TWO COMPARTMENTS (draw a small box diagram)
- Within alveolar walls (interalveolar septa)
- Forms the air-blood barrier
- Peribronchovascular sheaths
- Interlobular septa
- Visceral pleura
3. ALVEOLAR WALL — THIN vs THICK SIDE ⭐ (examiners love this)
| Thin Side | Thick Side | |
|---|---|---|
| Thickness | ~0.3 µm | Wider |
| Contents | Fused BM only | Elastin + Collagen + Fibroblasts |
| Function | Gas exchange | Structural support |
4. ECM COMPONENTS (list 4-5)
- Collagen (type I, III, IV) — tensile strength
- Elastin — recoil
- Proteoglycans (decorin, versican, hyaluronan)
- Fibronectin — cell adhesion
- Laminin — basement membrane
5. CELLS (list 5)
- Type I pneumocytes (gas exchange)
- Type II pneumocytes (surfactant)
- Fibroblasts/myofibroblasts (collagen synthesis)
- Alveolar macrophages (immunity)
- Mast cells (allergy)
6. CLINICAL SIGNIFICANCE — 5 KEY CONDITIONS ⭐
| Condition | Compartment Affected | Key Point |
|---|---|---|
| Pulmonary edema | Peribronchovascular first → septa → alveoli | Kerley B lines, peribronchial cuffing |
| IPF | Alveolar wall | Fibroblastic foci, TGF-β1, restrictive PFTs |
| Sarcoidosis | Peribronchovascular + subpleural | Non-caseating granulomas, hilar LN |
| Lymphangitic carcinomatosis | Interlobular septa + lymphatics | Nodular septal thickening on HRCT |
| Interstitial emphysema | Loose-binding CT | Air tracks to mediastinum → pneumomediastinum |
7. RADIOLOGY (3 lines max)
- Kerley B lines = thickened interlobular septa
- Ground glass = alveolar wall thickening
- Honeycombing = end-stage fibrosis
EXAM WRITING TIPS
- 5-mark Q: Definition + 2 compartments + thin/thick side + 2 clinical conditions
- 10-mark Q: All 7 sections above + one small diagram of thin/thick alveolar wall
- Always link anatomy to disease (e.g. "loose-binding tissue expands first in edema because it is a potential space")
- Draw the thin/thick side table - it takes 30 seconds and gets you marks every time
I think it is less
Interstitium of the Lung — Complete Exam Answer (Bullet Format)
1. DEFINITION
- Interstitium = connective tissue space between the alveolar epithelium and capillary endothelium
- Not a cavity — it is a 3D scaffolding of fibers, cells, and fluid
- Extends from alveolar walls to peribronchovascular sheaths, interlobular septa, and visceral pleura
- Maintains structural integrity while allowing efficient gas exchange
2. TWO COMPARTMENTS
A. Parenchymal (Alveolar Wall) Interstitium
- Located within the interalveolar septa
- Contains fused basement membranes of epithelium + endothelium
- Houses elastin, collagen, fibroblasts
- Forms the air-blood barrier
- Site of gas exchange and earliest fluid accumulation in edema
B. Loose-Binding (Extra-Alveolar) Connective Tissue
- Surrounds airways, pulmonary vessels → peribronchovascular sheaths
- Forms interlobular septa (partitions between secondary lobules)
- Extends to visceral pleura
- Is a potential space — expands in edema, emphysema, lymphangitis
- Contains lymphatics, nerves, bronchial vessels
3. MICROANATOMY — THIN vs THICK SIDE OF ALVEOLAR WALL ⭐
Thin Side
- Type I pneumocyte → fused basement membranes → capillary endothelium
- Thickness ~0.3 µm
- Minimal resistance to gas diffusion
- Primary site of O2 and CO2 exchange
Thick Side
- Type I pneumocyte → separate BM → interstitial space → capillary endothelium
- Interstitial space contains: elastin (EL), collagen (COL), proteoglycans, fibroblasts
- Provides structural support to the alveolar wall
- This side widens first in interstitial edema and fibrosis
4. EXTRACELLULAR MATRIX (ECM) COMPONENTS
- Collagen (Type I, III, IV) — tensile strength; basket-like 3D arrangement around alveoli
- Elastin — allows expansion and elastic recoil; part of the "elastic continuum" of the lung
- Reticulin fibrils — fine supporting network of alveolar walls
- Proteoglycans — versican, decorin, hyaluronan; form gel-like matrix; decorin downregulates TGF-β1
- Fibronectin — cell adhesion and wound repair
- Tenascin — upregulated in injury and inflammation
- Laminin — key component of basement membranes
- Fibrils are continuous from alveolar wall → visceral pleura → mechanical forces transmitted throughout lung
5. CELLULAR COMPONENTS
- Type I pneumocytes — cover >90% alveolar surface; gas exchange
- Type II pneumocytes — produce surfactant; act as stem cells for Type I after injury
- Capillary endothelial cells — gas exchange; regulate fluid filtration (Starling forces)
- Fibroblasts — synthesize collagen, elastin, proteoglycans; maintain ECM
- Myofibroblasts — activated in injury; drive fibrosis; express α-SMA
- Alveolar macrophages — phagocytosis; innate immunity; release fibrogenic cytokines
- Mast cells — in bronchial CT and alveolar septa; role in allergy and asthma
- Plasma cells and lymphocytes — immune surveillance
6. LYMPHATICS
- Lymphatic capillaries begin in alveolar wall interstitium
- Drain toward peribronchovascular sheaths → hilar lymph nodes
- Also run in interlobular septa and visceral pleura
- In edema: fluid accumulates in peribronchovascular loose CT which lymphatics cannot efficiently drain
- Clearance depends on active Na+/water transport across epithelium
7. MECHANICAL FUNCTIONS
- Basket-like collagen/elastin framework maintains alveolar shape
- Prevents alveolar collapse between breaths
- Alveolar interdependence — neighboring alveoli splint each other open via shared interstitial fibers
- Mechanical forces at alveolar level transmitted to pleura via continuous fiber network
- Loss of elastin (emphysema) → loss of recoil → air trapping
8. CLINICAL SIGNIFICANCE ⭐⭐⭐
A. Pulmonary Edema
- Fluid first enters alveolar wall interstitium (thin side widens)
- Then accumulates in peribronchovascular loose CT → peribronchial cuffing on CXR
- Then fills interlobular septa → Kerley B lines on CXR
- Finally floods alveoli → air-space shadowing
- Treatment: diuretics, PEEP, restore Na+ transport
B. Interstitial Lung Disease (ILD)
- Injury to alveolar wall → fibroblast/myofibroblast activation → collagen deposition
- TGF-β1 is the key mediator
- Thickened alveolar wall → ↑ diffusion distance → hypoxia
- PFTs: restrictive pattern (↓ FVC, ↓ TLC, ↓ DLCO)
- HRCT: ground glass, honeycombing, traction bronchiectasis
C. Idiopathic Pulmonary Fibrosis (IPF)
- Recurrent microinjury to alveolar epithelium → abnormal repair
- ↑ collagen (COL1A1), ↑ tenascin, ↓ decorin → unchecked TGF-β1 → fibrosis
- Histology: UIP pattern — fibroblastic foci + honeycombing + temporal heterogeneity
- Treatment: nintedanib, pirfenidone (slow progression)
D. Interstitial Emphysema
- Ruptured alveoli → air enters loose-binding CT
- Dissects along peribronchovascular sheaths toward hilum
- Can cause pneumomediastinum and pneumothorax
- Causes: barotrauma (ventilated patients), neonatal birth asphyxia, whooping cough
E. Sarcoidosis
- Non-caseating granulomas in peribronchial, perivascular, subpleural interstitium
- Follows lymphatic distribution → peribronchovascular pattern on HRCT
- Prominent bilateral hilar lymphadenopathy
F. Lymphangitic Carcinomatosis
- Tumor cells spread along lymphatics in interlobular septa and peribronchovascular sheaths
- HRCT: nodular septal thickening, beaded bronchovascular bundles
- Severe dyspnea disproportionate to radiology
- Common primaries: breast, lung, stomach, colon, pancreas
G. ARDS
- Diffuse alveolar damage → injury to both epithelium and endothelium
- Protein-rich fluid floods interstitium then alveoli
- Fibroproliferative phase → fibroblast proliferation → organizing fibrosis
- Hyaline membrane formation on histology
H. Pneumoconiosis
- Inhaled particles (silica, asbestos, coal) → macrophage activation → fibrogenic cytokines → collagen deposition
- Silicosis: nodular fibrosis, upper lobes
- Asbestosis: lower lobe interstitial fibrosis, asbestos bodies, pleural plaques
I. Pulmonary Hypertension
- ↑ elastin + collagen in vessel adventitia (loose-binding interstitium)
- ECM remodeling contributes to irreversible vascular changes
J. Bronchial Asthma
- Mast cells in bronchial CT → activation → histamine, leukotrienes
- Chronic: sub-epithelial fibrosis of airway interstitium (remodeling)
9. RADIOLOGY SUMMARY
| Sign | Meaning |
|---|---|
| Kerley B lines | Thickened interlobular septa |
| Kerley A lines | Deep peribronchovascular edema |
| Peribronchial cuffing | Peribronchovascular edema |
| Ground glass | Alveolar wall thickening |
| Honeycombing | End-stage fibrosis |
| Nodular septal thickening | Lymphangitic Ca / sarcoidosis |
| Traction bronchiectasis | Fibrotic distortion of interstitium |
EXAM STRATEGY
- 5 marks — Definition + 2 compartments + thin/thick table + 3 clinical conditions
- 10 marks — All sections above + radiology table + one thin/thick diagram
- Always say: "loose-binding compartment is a potential space that expands first in edema"
- Always say: "thin side = fused BM, thick side = elastin + collagen + fibroblasts"
- Mention TGF-β1 for any fibrosis question — it is the single most important mediator
From next time what I should tell u so that I get the same answer . I think this is good format to fetch marks
"Give me exam answer for [topic] in bullet point format for [X] marks — include definition, classification/types, components, functions, and clinical significance with all conditions explained in points. Use tables where needed."
| What you say | What it gives you |
|---|---|
| "exam answer" | Focused, no unnecessary fluff |
| "bullet point format" | Easy to write in exam |
| "for 10 marks" | I calibrate how much to write |
| "definition, classification, components, functions" | Covers all anatomy/physiology basics |
| "clinical significance with all conditions" | Gets you the disease section with full points |
| "use tables where needed" | Thin/thick table, radiology table, summary table |
-
"Give me exam answer for blood-brain barrier in bullet format for 10 marks — include definition, structure, cells, functions, clinical significance"
-
"Give me exam answer for surfactant in bullet format for 5 marks — include definition, composition, synthesis, functions, clinical conditions"
-
"Give me exam answer for glomerular filtration barrier in bullet format for 10 marks — include layers, components, functions, diseases"