Scotopic vision
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Scotopic Vision
Scotopic vision is vision under low-light (dim or night) conditions. It is mediated almost exclusively by rod photoreceptors in the retina, in contrast to photopic (daylight) vision, which relies on cones.
1. The Duplex Retina
The human retina contains two complementary photoreceptor systems - an arrangement called the duplex retina (Neuroscience: Exploring the Brain):
| Feature | Rods (Scotopic) | Cones (Photopic) |
|---|---|---|
| Light condition | Dim / night | Bright / daylight |
| Number | ~120 million | ~5 million |
| Photopigment | Rhodopsin (1 type) | 3 types (S, M, L) |
| Peak sensitivity | 500 nm (blue-green) | ~560 nm (yellow-green) |
| Color vision | None | Yes |
| Visual acuity | Low | High |
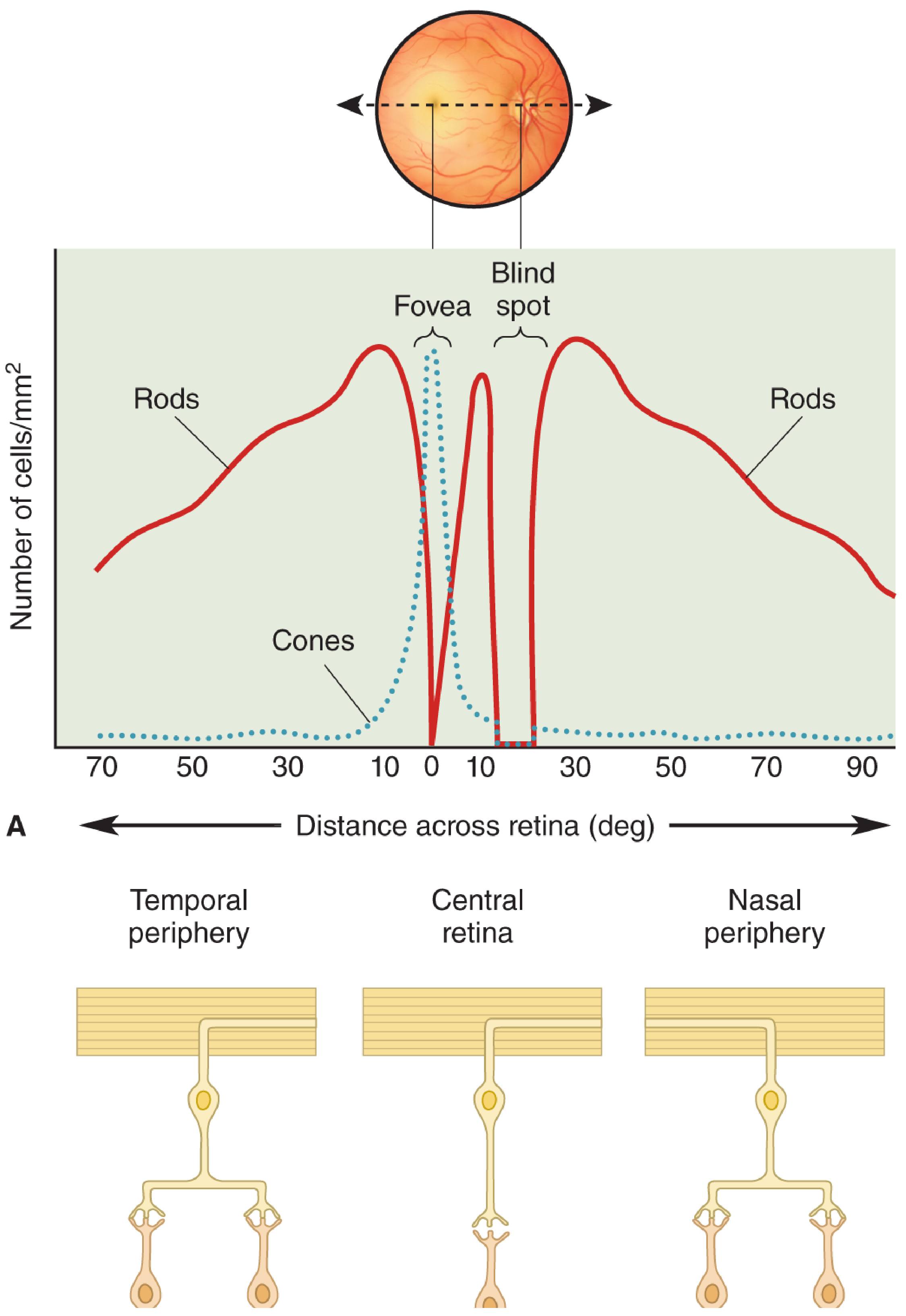
| Location | Peripheral retina | Fovea / central retina |
At intermediate light levels (indoor lighting, nighttime traffic), both rods and cones contribute - this is called mesopic vision.
2. Distribution of Rods and the "No Fovea" Effect
Rods are absent from the central fovea and are concentrated in the peripheral retina. This has a key consequence under scotopic conditions: visual acuity at night is greatest in the peripheral retina, not the center. Staring directly at a dim star makes it disappear (foveal fixation = no rods), while looking slightly to the side reveals it (peripheral rod stimulation). - Neuroscience: Exploring the Brain, p. 864
3. Rhodopsin - The Scotopic Photopigment
Rods contain rhodopsin (visual purple), a G-protein-coupled receptor composed of:
- Retinal - an aldehyde of vitamin A (11-cis configuration in the dark)
- Opsin - a 41 kDa protein making up 90% of total rod disk membrane protein
How light triggers a signal:
- Light converts retinal from 11-cis to all-trans isomer
- This conformational change activates opsin
- Opsin activates transducin (a heterotrimeric G-protein: Tα, Gβγ)
- Tα activates phosphodiesterase (PDE)
- PDE degrades cGMP in the outer segment
- cGMP-gated cation channels close - shutting off the "dark current"
- The photoreceptor hyperpolarizes (membrane potential goes more negative)
- Reduced glutamate release at the synaptic terminal signals downstream bipolar cells
In the dark, cGMP-gated channels are open, Na⁺ flows in, and the photoreceptor is relatively depolarized (continuously releasing glutamate). - Ganong's Review of Medical Physiology, p. 203-204
4. Spectral Sensitivity and the Purkinje Shift
Scotopic vision has peak spectral sensitivity at ~500 nm (blue-green), compared to ~560 nm for photopic (cone-based) vision. The shift in peak sensitivity from 560 nm to 500 nm as light levels fall is called the Purkinje shift.
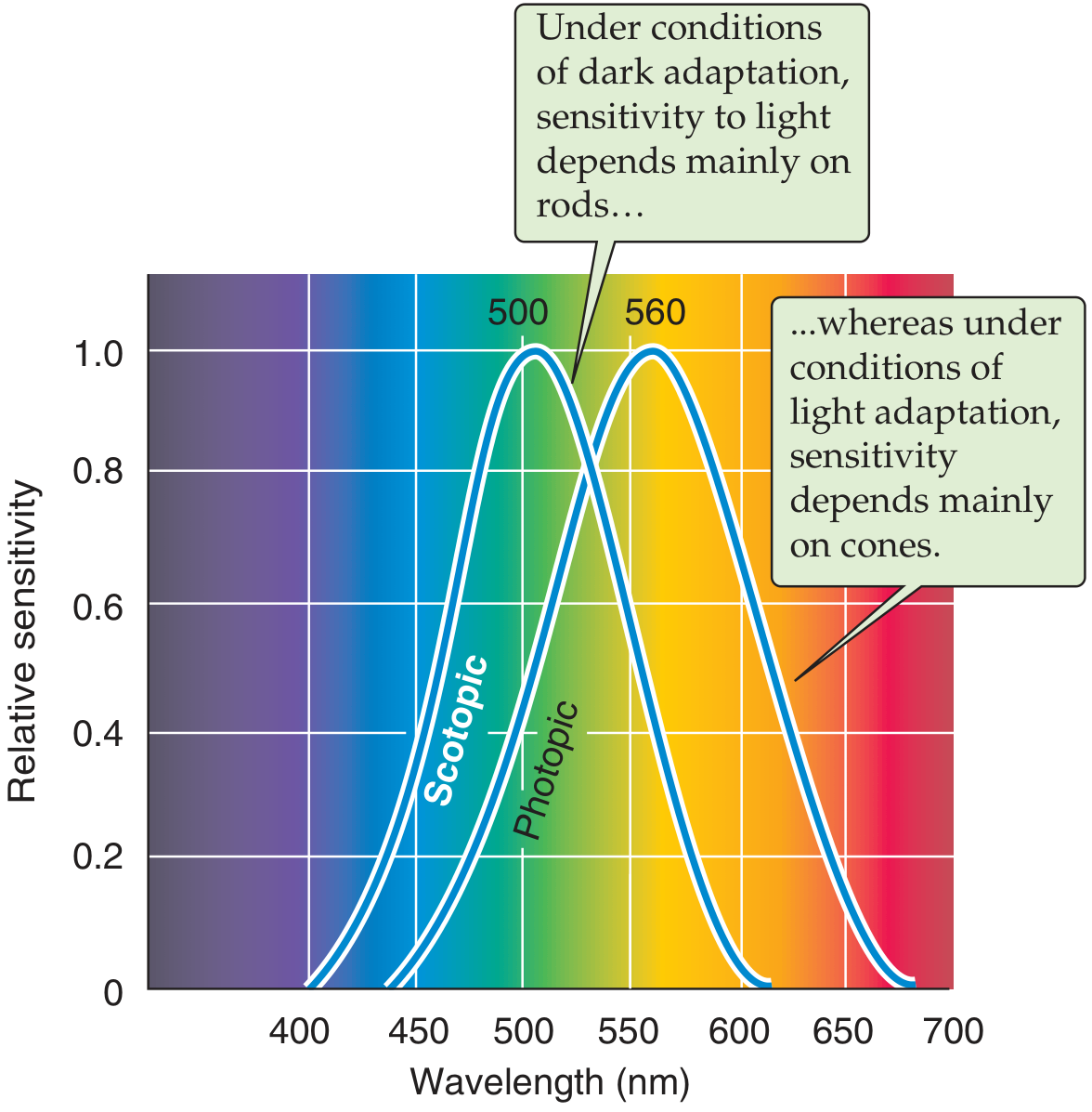
This means under scotopic conditions, blue and green objects appear relatively brighter than red objects compared to daytime. - Medical Physiology (Boron & Boulpaep), p. 549
5. Loss of Color in Scotopic Conditions
Objects lose their color under scotopic conditions - appearing as drab blue-green shades regardless of their daytime color, because cone activation is required for normal color perception. This is a profound perceptual effect that most people do not consciously notice due to familiarity. In modern urban environments, streetlights and neon signs can provide enough illumination to partially activate cones even at night. - Neuroscience: Exploring the Brain, p. 865
6. Dark Adaptation
Dark adaptation is the progressive increase in retinal sensitivity when moving from bright to dim light. It is nearly complete in ~20 minutes but may continue further.
Two-component response:
- Rapid, small drop in threshold - due to cone dark adaptation (seen when only fovea is tested)
- Slower, larger drop - due to rod dark adaptation, involving regeneration of rhodopsin bleached by bright light
Mechanisms:
- Pupil dilation (contributes ~10-fold increase in sensitivity - only a minor factor)
- Rhodopsin regeneration - the dominant mechanism (~1 million-fold overall increase)
- Retinal circuit reorganization - more rods converge onto each ganglion cell, increasing sensitivity
- Ca²⁺-mediated feedback: when cGMP-gated channels close (in bright light), Ca²⁺ entry stops, relieving inhibition of guanylyl cyclase → cGMP synthesized → channels reopen (prevents saturation)
Light adaptation (readjusting from dark to bright) takes only 5-10 minutes and is essentially the reversal of dark adaptation.
Practical note: Wearing red goggles in bright light allows cones to function while letting rods dark-adapt - used by radiologists and pilots who need immediate scotopic sensitivity. - Ganong's Review of Medical Physiology, p. 205
7. Clinical Relevance
| Condition | Mechanism | Effect on Scotopic Vision |
|---|---|---|
| Vitamin A deficiency | Retinal synthesis impaired | Night blindness (nyctalopia) - earliest sign |
| Retinitis pigmentosa | Rod degeneration | Progressive nyctalopia, then tunnel vision |
| Rod monochromatism (complete achromatopsia) | No functioning cones | Photopic ERG absent; only scotopic vision remains |
| Enhanced S-cone / Goldmann-Favre syndrome | Rod degeneration + abnormal cones | Nyctalopia in childhood |
Night blindness from vitamin A deficiency occurs because retinal (vitamin A aldehyde) is essential for rhodopsin synthesis. Treatment with vitamin A restores rod function if given before receptor destruction. - Ganong's Review of Medical Physiology, p. 204 (Clinical Box 10-3)
Sources:
- Ganong's Review of Medical Physiology, 26th ed., pp. 202-206
- Neuroscience: Exploring the Brain, 5th ed., pp. 858-883
- Medical Physiology (Boron & Boulpaep), pp. 549-550
- Kanski's Clinical Ophthalmology, 10th ed., relevant chapters on retinal dystrophies
What is macular sparing
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have all the information needed for a thorough answer. Here it is:
Macular Sparing
Macular sparing is a visual field phenomenon in which a homonymous hemianopia (loss of the same half of the visual field in both eyes) is present, but the central macular (fixation) vision remains intact. It is the hallmark of occipital lobe (visual cortex) lesions, particularly those caused by posterior cerebral artery (PCA) infarction.
Anatomy Background
The macula (central 5-10° of visual field) is disproportionately represented in the primary visual cortex (V1). Its cortical representation lies at the occipital pole - the most posterior tip of the occipital lobe. The peripheral visual fields are represented more anteriorly within the calcarine fissure.
Critically, the two regions have different blood supplies:
| Cortical Region | Blood Supply |
|---|---|
| Peripheral visual field cortex (anterior calcarine) | Posterior cerebral artery (PCA) |
| Macular cortex (occipital pole) | Middle cerebral artery (MCA) (or collaterals from MCA) |
This dual supply is the anatomical basis for macular sparing. - Kanski's Clinical Ophthalmology, p. 820
Why Macular Sparing Occurs
When the posterior cerebral artery is occluded, the anterior calcarine cortex (representing the peripheral visual field) is infarcted, but the occipital pole (representing the macula) survives because it is also supplied by the MCA. The result is:
Left or right homonymous hemianopia with preservation of central (macular) vision
A second reason is purely anatomical: the macular representation in V1 is disproportionately large relative to peripheral fields. An occipital lesion therefore needs to extend a considerable distance to destroy both peripheral and macular cortical representations. - Ganong's Review of Medical Physiology, p. 211
As stated in Costanzo Physiology: "Macular sparing occurs because lesions of the visual cortex do not destroy all neurons that represent the macula." - p. 97
Visual Field Pattern
- The patient has a congruous homonymous hemianopia (same-sided field loss in both eyes, with sharp vertical midline cut)
- But a central island of vision (typically ~5°) is preserved around fixation
- The defect respects the vertical meridian but does NOT encroach on the foveal center
Examples of macular sparing patterns (Neuroanatomy through Clinical Cases, p. 501):
- (A) Monocular concentric visual loss with central sparing - e.g., retinitis pigmentosa, raised ICP
- (B) Left homonymous hemianopia with macular sparing - e.g., right PCA infarct preserving the occipital pole
- (C) Left superior quadrantanopia with macular sparing - e.g., lesion of inferior bank of right calcarine fissure sparing the occipital pole
Classic Cause
Posterior cerebral artery (PCA) infarction is responsible for >90% of homonymous hemianopia without other neurological deficits. PCA occlusion produces:
- Contralateral congruous homonymous hemianopia
- With macular sparing (because the occipital pole retains MCA supply)
Kanski's Clinical Ophthalmology summarizes: "Occlusion of the posterior cerebral artery will therefore tend to produce a macular-sparing congruous homonymous hemianopia." - p. 820
Macular Sparing vs. Macular Splitting
| Feature | Macular Sparing | Macular Splitting |
|---|---|---|
| Central vision | Preserved | Lost (defect cuts through fixation) |
| Typical cause | PCA infarct (occipital pole survives) | Direct damage to occipital pole (e.g., head trauma, MCA infarct) |
| Blood supply reason | MCA protects occipital pole | MCA territory involved |
Damage to the tip of the occipital cortex - as in a direct head injury - tends to give rise to congruous homonymous macular defects (macular splitting). - Kanski's, p. 820
Bilateral Occipital Lesions
Bilateral PCA territory infarcts can cause bilateral homonymous hemianopia with macular sparing ("keyhole vision" or "tunnel vision from the back") - a small central island is all that remains. This is distinct from anterior pathway tunnel vision (e.g., glaucoma, retinitis pigmentosa). - Localization in Clinical Neurology, 8th ed.
Clinical Significance
- Localizing value: Macular sparing points to the occipital lobe, not more anterior visual pathway lesions (optic tract or radiation lesions typically cause macular splitting)
- Pupillary reflex is preserved: Because fibers to the pretectal pupillary reflex area leave the optic tract before the geniculate - so even with cortical blindness, pupils react normally to light
- Reading and daily function: Patients with macular sparing may retain enough central vision for reading and face recognition despite a large field defect
- Driving: Even with macular sparing, hemianopia typically disqualifies patients from driving
Sources:
- Ganong's Review of Medical Physiology, 26th ed., p. 211
- Costanzo Physiology, 7th ed., p. 97
- Kanski's Clinical Ophthalmology, 10th ed., p. 820
- Neuroanatomy through Clinical Cases, 3rd ed., p. 501
This is a shared conversation. Sign in to Orris to start your own chat.