What is Hodgkin lymphoma
Reading File
Finding Sources
Searching PubMed
"Hodgkin lymphoma"[MeSH Terms] AND treatment
Reading File
Reading File
Searching Images
Hodgkin lymphoma Reed-Sternberg cell histology
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to give a thorough answer. Let me compile everything.
Hodgkin Lymphoma
Hodgkin lymphoma (HL) is a B-cell malignancy defined by the presence of distinctive neoplastic Reed-Sternberg (RS) cells set within a reactive inflammatory background. It is one of the most curable cancers in oncology.
Histology — The Reed-Sternberg Cell
The sine qua non of HL is the Reed-Sternberg cell — a giant cell (15–45 µm) with a multilobate nucleus, exceptionally prominent nucleoli, and abundant slightly eosinophilic cytoplasm. The classic form is binucleate, with two mirror-image nuclear lobes each containing a large acidophilic nucleolus surrounded by a clear halo, giving the characteristic "owl-eye" appearance.
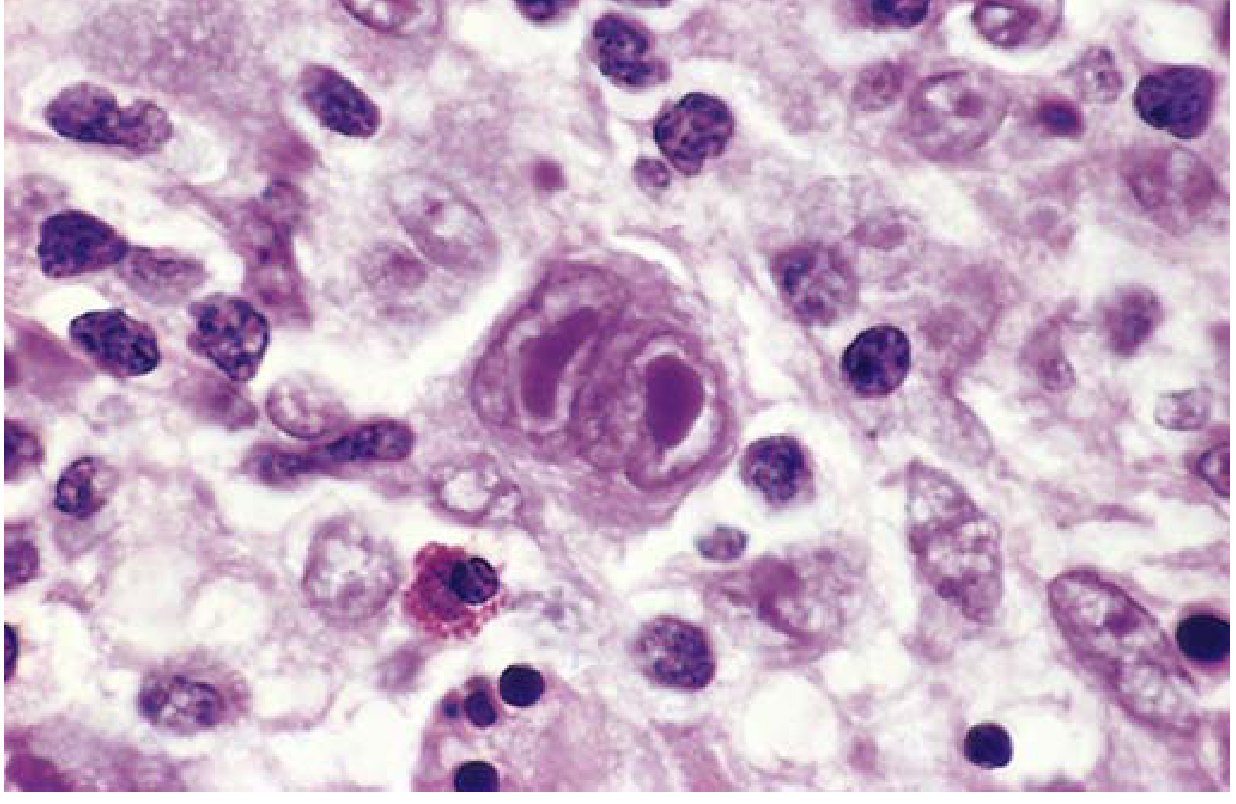
Immunophenotype: RS cells express CD15 and CD30, but do NOT express CD45 (leukocyte common antigen) or typical B-cell/T-cell markers. Despite this unusual phenotype, elegant single-cell microdissection studies confirmed that RS cells arise from germinal center B cells — their rearranged immunoglobulin genes show somatic hypermutation.
Classification
Five subtypes are recognized. The first four are grouped as Classic Hodgkin Lymphoma (cHL):
| Subtype | Key Features | Notes |
|---|---|---|
| Nodular sclerosis | Lacunar RS cell variants; collagen bands dividing lymphoid tissue into nodules | Most common; equally M:F; adolescents/young adults; excellent prognosis |
| Mixed cellularity | Classic RS cells amid eosinophils, plasma cells, macrophages | ~25% of cases; most common in >50 years; male predominance; EBV in ~70% |
| Lymphocyte-rich | Few RS cells, predominant small lymphocytes | Uncommon |
| Lymphocyte depletion | Abundant RS cells, sparse lymphocytes | Rarest; older/immunocompromised patients; poorer prognosis |
| Nodular lymphocyte-predominant (NLPHL) | ~10% of cases; RS variants express germinal center B-cell markers (CD20+, CD15−, CD30−) | Distinct natural history from cHL |
Pathogenesis
- Cell of origin: Germinal center B cells (proven by clonal immunoglobulin gene rearrangements with somatic hypermutation in RS cells)
- EBV association: EBV is found in RS cells in ~50% of HL cases overall, and up to ~70% of the mixed-cellularity subtype. The identical viral integration site in all RS cells of a given case indicates EBV infection precedes clonal expansion
- Immune evasion: RS cells express high levels of PD-L1 and PD-L2 (often due to amplification of chromosome 9p24.1), and frequently lose β2-microglobulin/MHC class I expression — allowing them to evade T-cell killing. This is why anti-PD-1 checkpoint inhibitors are highly effective even in refractory disease
- Cytokine milieu: RS cells secrete IL-5 (eosinophil chemoattractant), TGF-β (fibrogenic), and IL-13 (autocrine growth) — explaining the reactive inflammatory background that paradoxically supports RS cell survival
Epidemiology
- Incidence: ~2.7 per 100,000 per year in North America/Europe; ~30,000 new cases annually in North America and Europe
- Bimodal age distribution: Early peak at 25–30 years; late peak >50 years
- Slightly more common in males; higher incidence in White and higher socioeconomic groups
- History of infectious mononucleosis increases risk ~3-fold
Clinical Features
- Painless lymphadenopathy — usually cervical, supraclavicular, or mediastinal (nodular sclerosis has a striking propensity for the lower cervical/supraclavicular/mediastinal nodes)
- B symptoms (fever >38°C, drenching night sweats, unexplained weight loss >10% body weight in 6 months) — indicate more advanced disease
- Contiguous spread — unlike non-Hodgkin lymphoma, HL typically spreads in a stepwise fashion to anatomically adjacent lymph node groups, which has important therapeutic implications
- Mediastinal mass may cause cough, dyspnea, or superior vena cava syndrome
Staging — Modified Ann Arbor System
| Stage | Involvement |
|---|---|
| I | Single lymph node region (or one extralymphatic site) |
| II | ≥2 lymph node regions, same side of diaphragm |
| III | Lymph node regions on both sides of diaphragm |
| IV | Diffuse or disseminated involvement of extralymphatic organs |
Suffix "B" = B symptoms present; "A" = absent. Bulky disease = any mass ≥10 cm.
Staging workup: CBC, metabolic panel, ESR, serum albumin, HIV/hepatitis serology; contrast CT (neck, thorax, abdomen, pelvis); and crucially FDG-PET/CT, which has replaced bone marrow biopsy for staging.
Treatment
| Group | Stage | Regimen |
|---|---|---|
| Limited-stage | IA or IIA, non-bulky | ABVD ×2 + involved-region radiotherapy (IRRT); or ABVD ×3 alone if complete metabolic response on PET; checkpoint inhibitor + AVD ×4 if partial response |
| Advanced-stage | IB, IIB, any III/IV, or bulky | ABVD ×6; or A+AVD (brentuximab vedotin + AVD) ×6; or escalated BEACOPP ×4–6 |
| Relapsed/Refractory | All | Salvage chemotherapy → high-dose chemoradiation → autologous hematopoietic cell transplantation |
ABVD = doxorubicin (Adriamycin), bleomycin, vinblastine, dacarbazine
BEACOPP = bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone
A+AVD = brentuximab vedotin + doxorubicin, vinblastine, dacarbazine
BEACOPP = bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone
A+AVD = brentuximab vedotin + doxorubicin, vinblastine, dacarbazine
Checkpoint inhibitors (nivolumab, pembrolizumab) — highly active given PD-L1/L2 overexpression by RS cells; used in relapsed/refractory disease and increasingly in frontline unfavorable-stage disease with progression-free survival >98% in recent trials.
Prognosis
HL is among the most curable malignancies:
- Limited-stage: >95% cure rate
- Advanced-stage: ~70–80% cure with modern regimens
- The major clinical challenge is minimizing long-term treatment toxicity (secondary malignancies, cardiopulmonary complications, infertility) while maintaining high cure rates
Sources: Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine, Chapter 172 (Connors & Savage)
What is different between Hodgkin and non Hodgkin lymphoma
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material from both sides. Here is a thorough side-by-side comparison:
Hodgkin Lymphoma vs. Non-Hodgkin Lymphoma
These are two broad categories of lymphoid malignancy that share the same tissue of origin (lymphoid cells) but differ substantially in almost every clinically meaningful way.
1. Defining Histology
| Feature | Hodgkin Lymphoma (HL) | Non-Hodgkin Lymphoma (NHL) |
|---|---|---|
| Hallmark cell | Reed-Sternberg (RS) cell — giant binucleate cell with "owl-eye" nucleoli (CD15+, CD30+, CD45−) | No RS cells; tumor composed of a monomorphic proliferation of neoplastic lymphoid cells |
| Tumor cell fraction | RS cells make up only a tiny fraction (<1–5%) of the tumor mass; background is reactive inflammatory cells | Neoplastic cells constitute the bulk of the tumor |
| Cell of origin | Almost always germinal center B cells (despite aberrant phenotype) | B cells (~85% of cases), T cells, or NK cells |
2. Classification Complexity
| HL | NHL | |
|---|---|---|
| Subtypes | 5 well-defined subtypes (nodular sclerosis, mixed cellularity, lymphocyte-rich, lymphocyte depletion, nodular lymphocyte-predominant) | Dozens of distinct entities in the WHO classification — organized by cell lineage (B-cell vs. T/NK-cell) and maturation stage |
| Common B-cell NHL types | — | Diffuse large B-cell lymphoma (DLBCL, ~30%), follicular lymphoma (~20%), marginal zone lymphoma, mantle cell lymphoma, Burkitt lymphoma, CLL/SLL |
| Common T-cell NHL types | — | Peripheral T-cell lymphoma NOS, anaplastic large cell lymphoma (ALCL), mycosis fungoides, angioimmunoblastic T-cell lymphoma |
| Behavior spectrum | Mostly predictable; excellent curability | Ranges from indolent (follicular lymphoma — slow, may never need treatment) to highly aggressive (Burkitt lymphoma — doubles in hours) |
3. Pattern of Spread
| HL | NHL | |
|---|---|---|
| Spread pattern | Contiguous/stepwise — starts in one node or chain and spreads to anatomically adjacent nodes in an orderly fashion | Non-contiguous — spreads unpredictably, skipping node groups |
| Extranodal involvement | Uncommon (except advanced disease) | Common — NHL frequently involves extranodal sites (bone marrow, GI tract, CNS, skin, liver, Waldeyer's ring) |
| Mediastinal involvement | Very common (especially nodular sclerosis HL) | Less prominent except in primary mediastinal large B-cell lymphoma or T-lymphoblastic lymphoma |
| Bone marrow involvement at diagnosis | Uncommon | Common in indolent NHLs (follicular lymphoma often involves marrow at diagnosis) |
4. Epidemiology
| HL | NHL | |
|---|---|---|
| Incidence | ~2.7 per 100,000/year | ~10× more common than HL; ~80,000+ new cases/year in the US |
| Age distribution | Bimodal — young adults (25–30 yrs) and older adults (>50 yrs) | Rising steadily with age; incidence increases sharply after age 40 |
| Gender | Slight male predominance | Slight male predominance |
| Immunodeficiency link | Less strongly linked | Strongly linked — HIV, organ transplant recipients, inherited immunodeficiencies greatly increase NHL risk |
| Trend | Stable | Incidence rising ~1.5–2% per year over past decades |
5. EBV Association
| HL | NHL | |
|---|---|---|
| EBV | Present in RS cells in ~50% of all HL cases (up to 70% of mixed-cellularity subtype); strongly implicated in pathogenesis | Present in specific NHL subtypes: Burkitt lymphoma (~25–40% in HIV), primary CNS lymphoma (nearly all in AIDS), plasmablastic lymphoma (most), PTLD |
6. Staging
Both use the Modified Ann Arbor staging system (Stages I–IV ± B symptoms). However:
- In HL, stage matters enormously for treatment decisions — limited vs. advanced stage drives the entire treatment algorithm
- In NHL, histologic subtype (indolent vs. aggressive) often matters more than stage for prognosis and treatment selection
7. Treatment
| HL | NHL | |
|---|---|---|
| Backbone | ABVD chemotherapy ± involved-region radiotherapy | Varies by subtype: R-CHOP (rituximab + cyclophosphamide, doxorubicin, vincristine, prednisone) is standard for aggressive B-cell NHL; watchful waiting for indolent disease |
| Anti-CD20 (rituximab) | Not applicable (RS cells are CD20−) | Cornerstone of B-cell NHL therapy (CD20+ in ~85%) |
| Anti-CD30 (brentuximab vedotin) | Used in HL (RS cells are CD30+) | Used only in specific CD30+ NHLs (e.g., ALCL) |
| Checkpoint inhibitors | Highly effective (PD-L1/L2 amplified on RS cells) | Used in select subtypes |
| CAR-T cell therapy | Limited role | Established in relapsed/refractory DLBCL |
| Overall curability | Excellent — >95% for limited stage; ~70–80% for advanced stage | Highly variable: aggressive NHLs often curable; indolent NHLs rarely curable but long survival possible |
8. Prognosis Summary
| HL | NHL | |
|---|---|---|
| 5-year survival | ~87% overall (one of the most curable cancers) | ~74% overall (highly variable by subtype) |
| Indolent disease | Uncommon concept | Key concept in NHL — follicular lymphoma may follow a waxing/waning course for decades |
| Major concern in survivors | Long-term toxicity of treatment (secondary malignancies, cardiac disease, pulmonary fibrosis, infertility) | Relapse; secondary transformation (e.g., follicular → DLBCL = "Richter transformation" analog) |
In one sentence: HL is a single, well-defined disease defined by the RS cell, with predictable nodal spread and high curability; NHL is a heterogeneous group of 30+ distinct lymphoid malignancies with variable behavior, frequent extranodal spread, and treatment tailored to each subtype.
Sources: Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine Ch. 171–172; Harrison's Principles of Internal Medicine 22E
WBCs and it's types
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.