Tb full exam notes of pathology in given topic :
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Robbins Pathologic Basis of Disease and Basic Pathology. I have enough material to write detailed, exam-quality notes. Let me now compose the full notes.
Tuberculosis (TB) — Full Pathology Exam Notes (MBBS Level)
Primary sources: Robbins, Cotran & Kumar — Pathologic Basis of Disease; Robbins & Kumar — Basic Pathology
1. DEFINITION
Tuberculosis is a communicable, chronic granulomatous disease caused by Mycobacterium tuberculosis. It primarily involves the lungs but may affect virtually any organ or tissue in the body.
2. ETIOLOGY AND BACTERIOLOGY
- Causative organism: Mycobacterium tuberculosis (human type); rarely M. bovis (from unpasteurized milk — bovine TB, now rare in developed countries).
- Characteristics: Slender, slightly curved, aerobic, acid-fast bacilli (AFB); rod-shaped with a waxy lipid-rich cell wall containing mycolic acids.
- Acid-fastness: Due to mycolic acids in the cell wall — the organism retains carbol-fuchsin dye after acid-alcohol decolorization (Ziehl-Neelsen stain).
- Growth: Slow-growing; culture on solid agar (Löwenstein-Jensen medium) shows visible colonies in 3–6 weeks; liquid media (BACTEC) gives results within 2 weeks.
- Virulence factors:
- Cord factor (trehalose dimycolate) — inhibits leukocyte migration, mitochondrial damage.
- Wax-D (cell wall component) — adjuvant-like effect, promotes granuloma formation.
- Sulfatides — inhibit phagolysosome fusion.
- Lipoarabinomannan (LAM) — inhibits macrophage activation, suppresses IFN-γ.
3. EPIDEMIOLOGY
- WHO (2022): ~10.6 million new cases worldwide; 1.3 million deaths (167,000 in HIV-infected persons).
- Leading infectious cause of death by a single pathogen globally.
- In the US: ~8,300 cases reported; 73% in foreign-born individuals.
- Risk factors for TB:
- HIV/AIDS (dominant risk factor — loss of CD4⁺ Th1 cells)
- Silicosis, diabetes mellitus, Hodgkin lymphoma
- Chronic renal failure, malnutrition, alcohol use disorder
- Glucocorticoids, TNF inhibitors, immunosuppression (transplants)
- Poverty, crowding, homelessness, incarceration
- Rare: inherited mutations in IL-12 receptor β1 → severe TB + atypical mycobacteria
4. PATHOGENESIS
Step 1 — Entry and Ingestion
- Organisms inhaled as droplet nuclei (1–5 μm particles) — settle in alveoli of lower lobe (better ventilated middle and lower zones).
- Alveolar macrophages phagocytose bacilli via mannose-binding lectin and complement receptor 3 (CR3).
- Dendritic cells also engulf and carry bacilli to draining lymph nodes.
Step 2 — Replication in Macrophages
- M. tuberculosis blocks phagolysosome formation by recruiting host protein coronin to the phagosome membrane → coronin activates calcineurin → inhibits phagosome-lysosome fusion.
- Bacteria replicate freely inside macrophages.
- During the first <3 weeks (pre-immune phase): unchecked proliferation → bacteremia and seeding of multiple sites (most people are asymptomatic or mildly flu-like at this stage).
Step 3 — Innate Immunity
- PAMPs on M. tuberculosis activate toll-like receptors:
- Lipoarabinomannan → TLR2
- Unmethylated CpG nucleotides → TLR9
- Enhance innate and adaptive immune responses.
- M. tuberculosis also infects neutrophils, resists killing, and after replicating induces death of infected cells.
Step 4 — Th1 Adaptive Immune Response (~3 weeks post-infection)
- Dendritic cells migrate to draining lymph nodes and present mycobacterial antigens to T cells.
- IL-12 and IL-18 (from APCs) drive differentiation of Th1 cells.
- Th1 cells produce IFN-γ, the critical cytokine that:
- Stimulates production of nitric oxide and reactive oxygen species (ROS) in phagolysosome → bactericidal.
- Mobilizes antimicrobial peptides (defensins, cathelicidin).
- Stimulates autophagy → destroys intracellular bacilli.
Step 5 — Granuloma Formation and Tissue Damage
- IFN-γ-activated macrophages differentiate into epithelioid histiocytes → aggregate into granulomas.
- Some epithelioid cells fuse → Langhans giant cells (nuclei arranged in horseshoe/peripheral pattern).
- TNF (from activated macrophages) is essential for granuloma maintenance → patients on TNF inhibitors have significantly increased risk of TB reactivation.
- In most individuals: granulomas contain infection with caseous necrosis (cheese-like centre).
- In advanced/immunosuppressed disease: ongoing inflammation → caseous necrosis ± cavitation — without granuloma formation.
Key concept — Infection vs. Disease
| Feature | Latent Infection | Active Disease |
|---|---|---|
| Organisms | Dormant, contained in granulomas | Proliferating, uncontrolled |
| Symptoms | None | Cough, fever, weight loss |
| Transmission | Not infectious | Infectious |
| Immune status | Intact Th1 response | Impaired (HIV, steroids, etc.) |
5. TUBERCULIN TEST (PPD / MANTOUX) AND IGRAs
Tuberculin Skin Test (TST / Mantoux)
- Intradermal injection of purified protein derivative (PPD) of M. tuberculosis.
- Read at 48–72 hours — measures visible, palpable induration.
- Positive = Type IV delayed hypersensitivity (DTH) reaction.
- Significance: Indicates T-cell sensitisation to mycobacterial antigens; does NOT differentiate infection from active disease.
IGRA (Interferon-Gamma Release Assay)
- In vitro test: patient's lymphocytes stimulated with M. tuberculosis antigens → IFN-γ production measured.
- More specific than TST (not affected by BCG vaccination).
False Negatives (Anergy) in both tests:
- Viral infections (measles, HIV)
- Sarcoidosis, Hodgkin lymphoma
- Malnutrition, immunosuppression
- Overwhelming active TB itself (anergy from excessive T-cell depletion)
False Positives:
- Atypical mycobacteria (TST only)
- Prior BCG vaccination (TST only; IGRAs less affected)
6. PRIMARY TUBERCULOSIS
Definition
- Disease occurring in a previously unexposed, unsensitised individual.
- Source of infection: exogenous (inhaled airborne droplet nuclei from an active case).
Sequence of Events
- Droplet nuclei inhaled → lodge in subpleural zone, lower part of upper lobe or upper part of lower lobe (most aerated regions).
- Initial exudative reaction (non-specific pneumonic patch) within days.
- After ~3 weeks, immune response develops → lesion organises into a granuloma with caseous necrosis.
- A 1–1.5 cm area of grey-white consolidation with caseous necrosis forms = Ghon focus (Ghon lesion).
- Bacilli drain via lymphatics to regional hilar/mediastinal lymph nodes → caseating lymphadenopathy.
- Ghon focus + regional caseating lymph node = Ghon complex.
- Ghon complex undergoes progressive fibrosis and calcification → Ranke complex (visible on CXR as calcified parenchymal nodule + calcified hilar node).
Outcomes of Primary TB
In ~95% of immunocompetent individuals:
- Infection is contained; Ghon complex calcifies.
- Organisms remain latent (dormant) for decades.
- No clinical disease; patient becomes tuberculin positive.
In ~5% (especially immunocompromised):
- Progressive primary TB: lesion enlarges, caseates, spreads → pneumonia, pleural effusion, hematogenous dissemination.
- Particularly in infants, elderly, HIV-positive individuals.
Morphology of Primary TB (Microscopy)
- Granulomas (tubercles): central caseous necrosis surrounded by epithelioid macrophages, Langhans giant cells, lymphocytes, fibroblasts.
- Caseating granulomas = hallmark of TB.
- Sites of hematogenous seeding may show granulomas in liver, spleen, kidneys, bone marrow, meninges, adrenals, bone — but in most immunocompetent people these remain dormant.
7. SECONDARY (POST-PRIMARY / REACTIVATION) TUBERCULOSIS
Definition
- TB occurring in a previously sensitised host.
- May follow shortly after primary TB or, more commonly, months to years later (reactivation of dormant organisms — latent TB reactivation).
- May also result from exogenous reinfection with a new strain.
Characteristics distinguishing it from Primary TB
| Feature | Primary TB | Secondary TB |
|---|---|---|
| Host immunity | Absent/naïve | Previously sensitised |
| Site of initial lesion | Mid/lower zone subpleural | Apex of upper lobe |
| Lymph node involvement | Prominent | Less prominent (due to prior immunity) |
| Cavitation | Rare | Common |
| Ghon complex | Forms | Already present (healed) |
| Progression | Often self-limited | Progressive if untreated |
Location
- Apex of one or both upper lobes (Simon foci — small apical seedlings from primary hematogenous spread that later reactivate).
- Reason: high O₂ tension, poor lymphatic drainage, less surfactant activity.
Morphology — Sequence
- Fibrocaseous nodule at lung apex: 1–2 cm focus, central caseous necrosis, surrounded by fibrosis.
- Cavity formation: caseous material liquefies and drains into airways → erosion into bronchus → tuberculous cavity (irregular, ragged walls lined by grey-white caseous material).
- Erosion of cavities into bronchi → aerogenous spread to other lung areas → tuberculous bronchopneumonia.
- Erosion into blood vessels → haemoptysis (and potentially dissemination).
Gross Pathology — Secondary TB
- Fibrocaseous lesions — soft caseous centre + surrounding fibrosis.
- Apical cavities with caseous grey walls; may be up to several cm.
- Satellite nodules around main cavity.
- Old healed lesions: dense fibrous scars ± calcification at apex.
Microscopy
- Caseating granulomas (as above) but more numerous and destructive.
- Areas of coagulative necrosis (caseous) — acellular, granular, eosinophilic.
- Langhans giant cells — multinucleated, peripheral arrangement of nuclei.
- Epithelioid macrophages (elongated, eosinophilic cytoplasm, "footprint" nuclei).
- Surrounding lymphocytes and peripheral fibrosis.
- In cavities: AFB may be numerous in caseous material.
8. DISSEMINATION AND COMPLICATIONS OF TB
A. Miliary Tuberculosis
- Definition: Haematogenous dissemination of M. tuberculosis → seeding of multiple organs with tiny (1–2 mm) granulomas resembling millet seeds.
- Occurs when: primary TB in immunocompromised, erosion of caseous focus into a vessel (pulmonary vein → systemic), or during secondary TB.
- Organs involved: Lungs, liver, spleen, bone marrow, kidneys, adrenals, meninges, eyes.
- Gross: Innumerable small yellow-white nodules throughout parenchyma.
- Micro: Non-caseating or caseating granulomas at multiple sites.
- CXR: Diffuse bilateral 1–3 mm nodules in a "snow-storm/millet seed" pattern.
B. Tuberculous Pleuritis / Pleural Effusion
- Extension of subpleural Ghon focus into pleural space.
- Exudative effusion (lymphocyte-predominant, high protein, low glucose, positive ADA).
- Parietal pleural biopsy shows caseating granulomas.
C. Tuberculous Lymphadenitis (Scrofula)
- Most common extrapulmonary TB manifestation.
- Cervical lymph nodes most commonly involved (especially posterior triangle).
- Nodes: caseous necrosis → matting → collar-stud abscess → sinus tract to skin.
- Histology: Caseating granulomas in lymph node parenchyma.
D. Tuberculous Meningitis
- Haematogenous seeding of leptomeninges.
- Exudate at base of brain (basal exudative meningitis) → obstructs CSF flow → hydrocephalus.
- Endarteritis → infarcts.
- CSF: Clear/turbid; lymphocytosis; elevated protein; very low glucose; acid-fast smear often negative (culture positive).
- Histology: Tubercles on meninges; endarteritis of small vessels.
E. Pott's Disease (Tuberculous Spondylitis)
- Haematogenous spread to vertebral bodies (lower thoracic / lumbar most common).
- Caseous necrosis destroys disc space → vertebral collapse → kyphosis/gibbus deformity.
- Psoas abscess: Cold abscess tracking along psoas sheath → inguinal region.
- Spinal cord compression → paraplegia (Pott's paraplegia).
F. Renal Tuberculosis
- Haematogenous seeding of renal cortex (high O₂) → caseating granulomas → papillary necrosis → cavitation → "putty kidney" (dystrophic calcification throughout).
- Bacteria shed in urine → ureteric stricture → sterile pyuria (WBCs in urine, no ordinary bacteria on culture).
- "Sterile pyuria" is a classic clue for renal TB.
G. Adrenal Tuberculosis
- Historically a cause of Addison's disease (adrenal insufficiency).
- Bilateral caseating granulomas → adrenal destruction.
H. GI / Peritoneal Tuberculosis
- Primary: ingestion of M. bovis (rare).
- Secondary: swallowed infected sputum.
- Ileocaecal region most commonly involved.
- Macroscopy: Transverse ulcers (perpendicular to long axis of bowel — vs. Crohn's longitudinal fissuring ulcers).
- Peritoneal TB: Ascites (lymphocyte-exudate, high ADA) + "dough-belly" (omentum matted, caseous).
9. SPECIAL PATTERNS
TB in HIV/AIDS
- Most common AIDS-defining infection worldwide.
- CD4⁺ count determines pattern:
- CD4 >350/μL: typical secondary TB (upper lobe cavitary disease).
- CD4 200–350/μL: atypical pattern, lower lobe involvement, less cavitation.
- CD4 <200/μL: Miliary TB, diffuse infiltrates, extrapulmonary TB dominant; non-caseating granulomas (poor granuloma formation due to lack of T cells).
- Co-infection with HIV dramatically worsens prognosis.
- Paradoxical reactions (Immune Reconstitution Inflammatory Syndrome — IRIS) occur when ART is started and immune function is restored.
Drug-Resistant TB
- MDR-TB: Resistant to isoniazid + rifampicin (two key first-line drugs).
- XDR-TB: MDR-TB + resistance to any fluoroquinolone AND at least one injectable second-line drug (amikacin, kanamycin, capreomycin).
- New WHO definitions (2021): Pre-XDR-TB = MDR-TB + fluoroquinolone resistance.
- Rising globally, particularly in Eastern Europe and South/Southeast Asia.
10. DIAGNOSIS
| Test | Details |
|---|---|
| Sputum AFB smear (Ziehl-Neelsen stain) | Rapid, cheap; detects >10,000 bacilli/mL; low sensitivity |
| Culture (gold standard) | Löwenstein-Jensen (3–6 wks); BACTEC liquid (2 wks); antibiotic susceptibility testing |
| PCR (GeneXpert MTB/RIF) | FDA-approved; detects M. tuberculosis + rifampicin resistance in hours |
| TST / Mantoux | Induration ≥10 mm (≥5 mm in HIV/immunosuppressed) at 48–72 hrs |
| IGRA (QuantiFERON-TB Gold) | In vitro; more specific than TST; not affected by BCG |
| Whole-genome sequencing | Predicts susceptibility >90% accuracy; not yet widely available |
| Histology (biopsy) | Caseating granulomas + AFB (Ziehl-Neelsen, auramine-rhodamine fluorescence) |
11. HISTOLOGICAL HALLMARKS — SUMMARY TABLE
| Feature | Description |
|---|---|
| Caseating granuloma | Central caseous necrosis + epithelioid macrophages + Langhans giant cells + lymphocytes + peripheral fibrosis |
| Caseous necrosis | Acellular, cheese-like, eosinophilic, granular; structureless on H&E |
| Epithelioid histiocytes | Elongated, pink cytoplasm, oblong "footprint" nucleus; arise from IFN-γ-activated macrophages |
| Langhans giant cells | Multinucleated; nuclei arranged in peripheral/horseshoe pattern (vs. foreign-body giant cells: random nuclei) |
| AFB on special stain | Slender red rods (Ziehl-Neelsen); bright fluorescent rods (auramine-rhodamine) |
| Fibrous capsule | Outer rim of fibrosis around granuloma |
12. CLINICAL FEATURES — PULMONARY TB
- Systemic: Fever (low-grade, afternoon), night sweats, malaise, anorexia, weight loss ("consumption").
- Respiratory: Persistent productive cough (>3 weeks), purulent sputum, haemoptysis (~50% of cases), pleuritic chest pain.
- Examination: Dullness at apex, bronchial breathing, amphoric breath sounds (over cavity), post-tussive suction sounds.
- CXR: Upper lobe infiltrates, cavitation, fibrosis, calcification, hilar lymphadenopathy (primary TB), miliary pattern.
13. TREATMENT (Overview — for context)
- First-line regimen (RIPE/DOTS): Rifampicin (R), Isoniazid (I), Pyrazinamide (P), Ethambutol (E).
- Phases: 2 months intensive (RIPE) + 4 months continuation (RI).
- BCG vaccine: Attenuated M. bovis; protects against severe childhood forms (miliary, meningeal TB); less effective against pulmonary TB in adults.
14. KEY HIGH-YIELD EXAM POINTS
- Ghon focus = primary parenchymal lesion (subpleural, lower upper lobe).
- Ghon complex = Ghon focus + ipsilateral caseating hilar lymph node.
- Ranke complex = calcified Ghon complex (healed, visible on CXR).
- Secondary TB site = apex of upper lobe (Simon foci).
- Caseous necrosis = cheese-like, acellular, eosinophilic — pathognomonic of TB.
- Langhans giant cells = peripheral/horseshoe nuclei (different from foreign-body type).
- IFN-γ = critical cytokine for granuloma formation and macrophage activation.
- TNF = essential for granuloma maintenance; TNF inhibitors → TB reactivation risk.
- Sterile pyuria = classic sign of renal TB.
- Pott's disease = vertebral TB → gibbus deformity + cold psoas abscess.
- Miliary TB = haematogenous dissemination; 1–2 mm nodules; resembles millet seeds.
- Scrofula = TB cervical lymphadenitis; collar-stud abscess.
- MDR-TB = resistant to rifampicin + isoniazid.
- In HIV with very low CD4: non-caseating granulomas (poor T-cell function).
- Tuberculin test positivity = delayed hypersensitivity (Type IV); does NOT mean active disease.
Sources: Robbins, Cotran & Kumar — Pathologic Basis of Disease (10th ed.), pp. 351–360; Robbins & Kumar — Basic Pathology (11th ed.), pp. 428–432.
Make it perfect of MBBS long answer in university exam.
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
tuberculosis granuloma caseating necrosis Langhans giant cell histology
Reading File
Reading File
Searching Images
primary tuberculosis Ghon complex Ghon focus lung pathology
Reading File
Searching Images
secondary tuberculosis cavitary upper lobe lung gross pathology
Searching Images
miliary tuberculosis millet seed nodules lung histology
I now have everything needed. Let me compose the perfect MBBS long-answer exam response — structured exactly as a university examiner expects.
TUBERCULOSIS — PATHOLOGY
Long Answer | MBBS University Examination Standard
Source: Robbins, Cotran & Kumar — Pathologic Basis of Disease; Robbins & Kumar — Basic Pathology
DEFINITION
Tuberculosis (TB) is a communicable, chronic granulomatous disease caused by Mycobacterium tuberculosis. It primarily affects the lungs but may involve virtually any organ or tissue in the body. It is the leading infectious cause of death from a single pathogen worldwide.
ETIOLOGY AND BACTERIOLOGY
The causative organism is Mycobacterium tuberculosis (human type). Rarely, Mycobacterium bovis causes TB via ingestion of unpasteurized contaminated milk (bovine TB), now rare in pasteurizing countries.
Characteristics of the organism:
- Slender, slightly curved, aerobic, non-spore-forming bacillus
- Acid-fast — owing to high mycolic acid content in the cell wall; retains carbol-fuchsin dye after acid-alcohol decolorization (Ziehl-Neelsen stain)
- Obligate aerobe — explains predilection for well-oxygenated areas (lung apex, renal cortex)
- Slow-growing: colonies appear in 3–6 weeks on Löwenstein-Jensen solid medium; 2 weeks in BACTEC liquid medium
Important virulence factors:
| Factor | Role |
|---|---|
| Cord factor (trehalose dimycolate) | Inhibits leukocyte migration; toxic to mitochondria |
| Sulfatides | Inhibit phagolysosome fusion |
| Lipoarabinomannan (LAM) | Binds TLR2; inhibits macrophage activation and IFN-γ action |
| Mycolic acids / wax-D | Adjuvant-like; promotes granuloma induction |
EPIDEMIOLOGY
- WHO (2022): ~10.6 million new cases; 1.3 million deaths worldwide.
- Called the "White Plague" or "consumption" historically.
- TB flourishes in settings of poverty, overcrowding, and chronic debilitating illness.
- In the US: 73% of cases are foreign-born; predominantly affects older adults, immigrants, the homeless, prisoners, and HIV-positive individuals.
Risk factors for developing active TB:
| Immunological Risk Factors | Other Risk Factors |
|---|---|
| HIV/AIDS (dominant risk — CD4⁺ loss) | Poverty, crowding, malnutrition |
| Glucocorticoids, TNF inhibitors | Silicosis (strongest occupational risk) |
| Post-transplant immunosuppression | Diabetes mellitus |
| Malignancy (Hodgkin lymphoma) | Alcohol use disorder |
| Inherited IL-12Rβ1 mutations | Chronic renal failure |
PATHOGENESIS
Concept: Infection vs. Disease
Infection = organisms present in the body (may be latent — no symptoms, not infectious). Active Disease = organisms proliferating with tissue destruction and clinical symptoms (infectious).
Only ~5–10% of infected immunocompetent individuals ever develop active disease. The rest harbour latent infection with dormant organisms in granulomas for decades.
Step-by-Step Mechanism
STEP 1 — Inhalation and Initial Infection (Days 1–21)
- TB is transmitted by airborne droplet nuclei (1–5 μm) — produced by coughing, sneezing, or speaking by a patient with active pulmonary TB.
- Droplet nuclei reach the alveoli (lower lobe or middle lobe — better ventilated).
- Alveolar macrophages phagocytose the bacilli via:
- Mannose-binding lectin receptors
- Complement receptor 3 (CR3 / CD11b/CD18)
- M. tuberculosis blocks phagolysosome formation: it recruits the host protein coronin to the phagosomal membrane → coronin activates calcineurin → inhibits phagosome-lysosome fusion.
- Bacteria replicate freely within macrophages. Infected macrophages migrate to the lung interstitium.
- Bacteraemia occurs within the first 3 weeks → haematogenous seeding of multiple organs (liver, spleen, kidney, meninges, bone, adrenals).
- At this stage: most patients are asymptomatic or have a mild flu-like illness.
STEP 2 — Innate Immune Response
- PAMPs on M. tuberculosis activate pattern recognition receptors:
- Lipoarabinomannan → TLR2
- Unmethylated CpG DNA → TLR9
- These interactions prime the innate and adaptive immune responses.
- M. tuberculosis also infects neutrophils → resists killing → replicates → induces neutrophil death.
STEP 3 — Adaptive Th1 Immune Response (~3 weeks post-infection)
- Dendritic cells process mycobacterial antigens and migrate to regional draining lymph nodes → present antigens to naïve CD4⁺ T cells.
- IL-12 and IL-18 (from antigen-presenting cells) drive Th1 cell differentiation.
- Th1 cells produce IFN-γ — the central cytokine of TB immunity.
Actions of IFN-γ:
- Activates macrophages → produce nitric oxide (NO) and reactive oxygen species (ROS) within phagolysosome → bactericidal
- Mobilises antimicrobial peptides (defensins, cathelicidin)
- Stimulates autophagy → destroys intracellular bacteria
STEP 4 — Granuloma Formation and Tissue Damage
- IFN-γ-activated macrophages transform into epithelioid histiocytes (elongated, abundant pale-pink cytoplasm, oblong "footprint" nucleus).
- Epithelioid cells aggregate → granuloma (the hallmark of TB).
- Some epithelioid cells fuse → Langhans giant cells (nuclei arranged in a horseshoe/peripheral pattern — distinguishing them from foreign-body giant cells with random nuclei).
- TNF (from activated macrophages) is essential for granuloma maintenance and integrity.
- Granuloma centre undergoes caseous necrosis: the bacteria and macrophages die → cheese-like (acellular, granular, eosinophilic) necrotic material.
- In most people: granulomas contain the infection. In immunocompromised: ongoing inflammation → tissue destruction without granuloma formation.
⚠️ Patients on TNF inhibitors (e.g., anti-rheumatic drugs) have a markedly elevated risk of TB reactivation because TNF is required to maintain granuloma integrity.
Tuberculin Test Basis
The Mantoux/PPD test and Interferon-Gamma Release Assays (IGRAs) detect this T-cell mediated delayed hypersensitivity (Type IV). A positive test indicates sensitisation to M. tuberculosis, but does NOT distinguish active disease from latent infection.
PRIMARY TUBERCULOSIS
Definition
Disease occurring in a previously unexposed, immunologically naïve host. Source: exogenous inhalation.
Sequence of Events and Morphology
- Inhaled bacilli → settle in subpleural zone, lower lobe or lower part of upper lobe (zones of maximal ventilation).
- Initial non-specific pneumonic patch (exudative reaction) develops within days.
- After ~3 weeks, cell-mediated immunity activates → exudative lesion organises into granuloma.
- A 1–1.5 cm area of grey-white pulmonary consolidation with central caseous necrosis = GHON FOCUS (also called Ghon lesion).
- Bacilli drain via lymphatics to regional hilar/paratracheal lymph nodes → caseating lymphadenopathy (prominent in children).
- GHON COMPLEX = Ghon focus + ipsilateral caseating hilar lymph nodes.
- In most cases (~95%), cell-mediated immunity contains the infection → both components undergo progressive fibrosis and dystrophic calcification → RANKE COMPLEX (visible on CXR as calcified peripheral nodule + calcified hilar node).
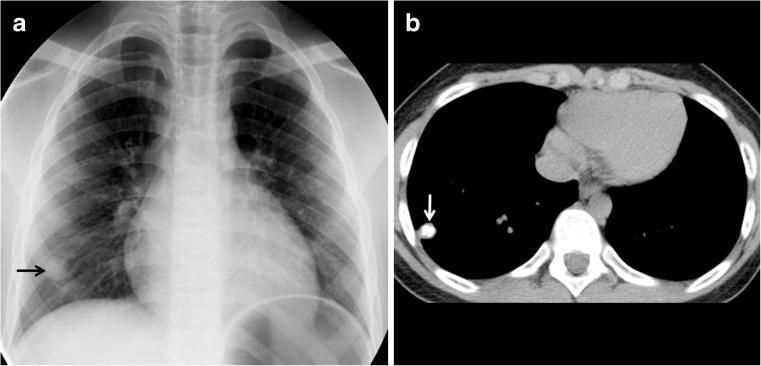
Calcified Ghon focus in primary TB (right lower lobe, arrow) — a healed primary lesion.
Microscopy of Primary TB Granuloma
- Central caseous necrosis: acellular, eosinophilic, granular — structureless (unlike coagulative necrosis which preserves outlines)
- Epithelioid histiocytes: surrounding the necrotic core; elongated pink cytoplasm, oblong nucleus
- Langhans giant cells: horseshoe/peripheral arrangement of nuclei; multinucleated
- Lymphocytic cuff: surrounding the epithelioid cells
- Outer fibrous rim: encircling the entire granuloma
Outcomes of Primary TB
| Outcome | Frequency | Details |
|---|---|---|
| Latent infection | ~95% | Contained; Ghon complex calcifies; organisms dormant for decades |
| Progressive primary TB | ~5% | Especially in infants, elderly, HIV+ persons |
| Haematogenous dissemination | Variable | Seeding of liver, spleen, kidney, meninges, bones during early bacteraemia |
SECONDARY (POST-PRIMARY / REACTIVATION) TUBERCULOSIS
Definition
TB arising in a previously sensitised host — either by reactivation of dormant organisms (latent TB reactivation) or by exogenous reinfection. It occurs months to years after primary infection.
Comparison with Primary TB
| Feature | Primary TB | Secondary TB |
|---|---|---|
| Host immunity | Naïve/absent | Previously sensitised |
| Site of initial lesion | Lower/middle zone (subpleural) | Apex of upper lobe (Simon foci) |
| Lymph node involvement | Prominent | Less prominent |
| Cavitation | Rare | Common and early |
| Ghon complex | Forms | Already calcified |
| Progression | Usually self-limited | Progressive if untreated |
Why the Apex?
Secondary TB localises to the apex of the upper lobe because:
- Simon foci — tiny apical seedlings deposited during initial primary bacteraemia
- High oxygen tension (M. tuberculosis is an obligate aerobe)
- Poor lymphatic drainage
- Reduced lymphatic clearance at the apex
Morphological Progression in Secondary TB
Stage 1 — Fibrocaseous Nodule
- Small (1–2 cm) focus at apex with caseating granuloma + surrounding fibrosis.
- Central caseous material may remain solid for a time.
Stage 2 — Cavity Formation
- Caseous material liquefies → drains into an adjacent bronchus → tuberculous cavity forms.
- Cavity walls: ragged, grey-white caseous lining; poorly vascularised.
- Positive AFB sputum smear (bacteria shed into sputum from cavity).
Stage 3 — Spread
- Erosion of cavity into bronchi → aerogenous (bronchogenic) spread → cough-spreads infection to other lung segments → tuberculous bronchopneumonia (patchy consolidation throughout lung).
- Spread via:
- Airways → same/opposite lung
- Lymphatics → hilar nodes, pleura
- Blood vessels → haematogenous miliary spread

CXR showing bilateral upper lobe cavitation — classic appearance of secondary TB.
Gross Pathology — Secondary TB Lung
- Fibrocaseous lesions with soft grey-yellow caseous centres and grey-white fibrotic walls
- Apical cavities — variable size, ragged walls
- Satellite nodules around main cavity
- Old healed lesions: dense apical scars, calcification, pleural adhesions
- In progressive disease: entire lobe can be replaced by caseous material
Microscopy — Secondary TB
- Caseating granulomas — more numerous and destructive than primary
- Caseous necrosis: acellular, granular, eosinophilic — no cellular detail
- Epithelioid macrophages — classical "footprint" nucleus
- Langhans giant cells — horseshoe/peripheral nuclei
- Lymphocytic infiltrate peripheral
- AFB on ZN stain — slender red rods in caseous material (may be scanty)
- Progressive disease: large areas of coagulative-caseous necrosis replacing normal architecture
COMPLICATIONS AND SPREAD — DISSEMINATION
A. Miliary Tuberculosis
Definition: Haematogenous dissemination of M. tuberculosis → seeding of multiple organs with innumerable tiny nodules resembling millet seeds (1–2 mm, yellow-white).
Mechanism:
- Erosion of a caseous focus into a pulmonary vein or lymphovascular channel → bacteraemia → systemic spread.
- May occur during primary (especially in immunocompromised) or secondary TB.
Organs affected: Lungs, liver, spleen, bone marrow, kidneys, adrenals, meninges, choroid of eye.
Gross: Innumerable 1–2 mm yellow-white nodules scattered uniformly throughout the parenchyma.
Microscopy: Non-caseating or caseating granulomas at multiple sites (in severely immunocompromised: granulomas may be absent — collections of phagocytes with organisms only).

Classic miliary TB pattern on CXR — diffuse bilateral micronodules resembling millet seeds.
B. Tuberculous Pleuritis / Pleural Effusion
- Extension of a subpleural Ghon focus or secondary TB lesion into the pleural space.
- Exudative effusion: lymphocyte-predominant, high protein, low glucose, raised ADA (adenosine deaminase >40 IU/L).
- Parietal pleural biopsy shows caseating granulomas.
- May organise → empyema necessitans → pleural fibrosis / trapped lung.
C. Tuberculous Lymphadenitis (Scrofula)
- Most common extrapulmonary form of TB.
- Cervical lymph nodes (posterior triangle) most commonly involved.
- Nodes undergo caseating necrosis → matting together → collar-stud (shirt-stud) abscess: caseous material perforates the deep fascia → subcutaneous fluctuant swelling connected to deep node by a narrow neck.
- Sinus tracts to skin surface may develop.
- Microscopy: Caseating granulomas in lymph node parenchyma; Langhans giant cells.
D. Tuberculous Meningitis
- Haematogenous seeding of leptomeninges (pia-arachnoid).
- Base of brain predominantly affected — thick gelatinous exudate (basal exudative meningitis).
- Complications: hydrocephalus (obstructed CSF flow), endarteritis → cerebral infarcts, cranial nerve palsies.
- CSF findings: Clear/slightly turbid; lymphocytic pleocytosis (cells 100–500/mm³); elevated protein; very low glucose (≤45 mg/dL or CSF/serum glucose <0.5); AFB smear often negative; culture gold standard.
- Histology: Granulomas on meninges; fibrinous exudate; endarteritis of small vessels.
E. Pott's Disease (Tuberculous Spondylitis)
- Haematogenous spread to vertebral bodies (most common site of skeletal TB).
- Predilection: lower thoracic and upper lumbar vertebrae (T10–L2).
- Mechanism: Caseous necrosis destroys intervertebral disc → spreads to adjacent vertebral bodies → vertebral collapse → angular kyphosis (gibbus deformity).
- Cold (Pott's) abscess: Caseous pus tracks along the psoas sheath → presents as a fluctuant swelling in the inguinal region; "cold" = no warmth/redness (unlike pyogenic).
- Complications: Pott's paraplegia (spinal cord compression by caseous mass or collapsed vertebra).
- Histology: Caseating granulomas in bone, disc space, paravertebral soft tissue.
F. Renal Tuberculosis
- Haematogenous seeding of renal cortex (high oxygen tension).
- Sequence: Cortical granuloma → caseation → papillary necrosis → cortical cavity → "putty kidney" (entire kidney replaced by dystrophic calcification).
- Bacilli shed in urine → ureteric stricture → obstructive uropathy.
- Classic finding: Sterile pyuria — WBCs in urine with no growth on routine bacterial culture ("sterile pyuria with acid urine" = TB until proven otherwise).
G. Adrenal Tuberculosis
- Bilateral caseating granulomas → adrenocortical destruction → historically a leading cause of Addison's disease (primary adrenocortical insufficiency).
H. Intestinal / Peritoneal Tuberculosis
- Either from ingestion of M. bovis (unpasteurised milk) or swallowed infected sputum.
- Ileocaecal region most commonly involved.
- Macroscopy: Transverse (circumferential) ulcers — perpendicular to the long axis of the bowel (vs. longitudinal fissuring ulcers of Crohn's disease).
- Lymph node caseation → peritoneal seeding → ascites (lymphocytic exudate, elevated ADA) + "dough-belly" (matted omentum with caseous nodules).
TUBERCULOSIS AND HIV/AIDS
HIV is the single most important risk factor for progression of latent TB to active disease. The CD4⁺ count determines the clinical pattern:
| CD4⁺ Count | Pattern of TB |
|---|---|
| >350 cells/μL | Typical secondary TB (upper lobe cavitary) |
| 200–350 cells/μL | Atypical pattern, lower lobe involvement, less cavitation |
| <200 cells/μL | Miliary TB, extrapulmonary TB, diffuse infiltrates; non-caseating (or absent) granulomas |
- Non-caseating granulomas in HIV occur because the Th1 response is insufficient to form proper granulomas.
- Immune Reconstitution Inflammatory Syndrome (IRIS): Paradoxical worsening of TB on starting ART as the immune system recovers.
DRUG-RESISTANT TUBERCULOSIS
| Type | Definition |
|---|---|
| MDR-TB | Resistant to Rifampicin + Isoniazid |
| XDR-TB | MDR-TB + resistance to any fluoroquinolone + at least one injectable second-line drug |
| Pre-XDR-TB (WHO 2021) | MDR-TB + fluoroquinolone resistance |
Mechanisms: mutations in rpoB gene (rifampicin), katG/inhA (isoniazid), gyrA/gyrB (fluoroquinolones).
DIAGNOSIS
| Test | Details | Notes |
|---|---|---|
| Sputum AFB smear (ZN stain) | Rapid, cheap; red rods on blue background | Requires >10,000 bacilli/mL; low sensitivity |
| Culture (Gold Standard) | LJ medium (3–6 wks); BACTEC (2 wks) | Also allows drug susceptibility testing |
| GeneXpert MTB/RIF (PCR) | Detects TB DNA + rifampicin resistance in 2 hours | FDA-approved; sensitive as culture in smear+ cases |
| Mantoux / TST | Intradermal PPD; induration read at 48–72 hrs | ≥10 mm positive; ≥5 mm in HIV/immunosuppressed |
| IGRA (QuantiFERON-TB Gold) | In vitro; detects IFN-γ from sensitised T cells | Not affected by BCG; more specific than TST |
| Biopsy + histology | Caseating granulomas + ZN/auramine stain for AFB | Used for lymph node, pleural, bone, intestinal TB |
| Whole-genome sequencing | >90% accuracy for drug susceptibility | Not widely available yet |
Tuberculin Test (Mantoux) — Details:
- Basis: Type IV delayed hypersensitivity (DTH) reaction to mycobacterial PPD.
- Positive: Induration ≥10 mm at 48–72 hours (not redness/erythema).
- Positive test = sensitisation only (does not differentiate active disease from latent infection).
False Negatives (Anergy):
- HIV/AIDS (CD4 <200), viral infections (measles), sarcoidosis
- Hodgkin lymphoma, malnutrition, overwhelming active TB itself
False Positives:
- BCG vaccination (TST, not IGRA)
- Infection with atypical (non-tuberculous) mycobacteria
CLINICAL FEATURES
Pulmonary TB (Secondary/Active):
- Constitutional (systemic): Low-grade fever (afternoon remittent), night sweats, malaise, anorexia, progressive weight loss ("consumption," "wasting disease")
- Respiratory: Productive cough (>3 weeks), purulent sputum, haemoptysis (in ~50%), pleuritic chest pain, dyspnoea
- Examination: Dullness at apex, bronchial breathing, post-tussive suction sounds (open cavities), amphoric breathing
CXR Findings:
- Primary TB: mid/lower zone opacity + hilar adenopathy (Ghon complex); calcified lesions (Ranke complex)
- Secondary TB: upper lobe infiltrates, cavitation, fibrosis, calcification, pleural effusion
- Miliary TB: diffuse bilateral 1–3 mm nodules ("millet seed" / "snowstorm" pattern)
TREATMENT (DOTS — Directly Observed Treatment, Short Course)
Standard Regimen:
- Intensive phase (2 months): Rifampicin (R) + Isoniazid (H/I) + Pyrazinamide (Z) + Ethambutol (E) — RIPE / HRZE
- Continuation phase (4 months): Rifampicin + Isoniazid — HR/RH
- Total duration: 6 months for drug-sensitive pulmonary TB
- TB meningitis: 9–12 months + adjunct corticosteroids
BCG Vaccine: Attenuated M. bovis; protects against severe childhood forms (miliary TB, TB meningitis); less effective against adult pulmonary TB.
HISTOLOGICAL HALLMARKS — QUICK SUMMARY TABLE
| Structure | Description | Significance |
|---|---|---|
| Caseating granuloma | Central caseous necrosis + epithelioid cells + Langhans giant cells + lymphocytes + fibrous rim | Hallmark of TB |
| Caseous necrosis | Cheese-like, acellular, granular, eosinophilic; structureless on H&E | Specific to TB (unlike coagulative necrosis) |
| Epithelioid histiocytes | Elongated cells, pale eosinophilic cytoplasm, oblong "footprint" nucleus | Arise from IFN-γ activated macrophages |
| Langhans giant cell | Multinucleated; nuclei in horseshoe/peripheral arrangement | Differentiate from foreign-body giant cells |
| Ghon focus | 1–1.5 cm subpleural caseous nodule, lower/upper lobe | Primary TB parenchymal lesion |
| Ghon complex | Ghon focus + ipsilateral caseating hilar lymph node | Hallmark of primary TB |
| Ranke complex | Calcified Ghon complex | Healed/resolved primary TB on CXR |
HIGH-YIELD EXAM POINTS (MBBS)
- TB is caused by M. tuberculosis — acid-fast, aerobic bacillus, identified by Ziehl-Neelsen stain.
- Mode of spread: airborne droplet nuclei (1–5 μm); NOT fomites or droplets.
- M. tuberculosis survives in macrophages by blocking phagolysosome formation via coronin-calcineurin pathway.
- Key immune effector: IFN-γ (from Th1 cells) — activates macrophages; drives granuloma formation.
- TNF maintains granuloma integrity — TNF inhibitors → reactivation of latent TB.
- Ghon focus = primary lung lesion; Ghon complex = lesion + hilar node; Ranke complex = calcified healed complex.
- Primary TB → lower/middle zone; Secondary TB → apex of upper lobe (Simon foci).
- Caseous necrosis = cheese-like, acellular, granular on H&E — characteristic of TB (other organisms cause liquefactive, coagulative, etc.).
- Langhans giant cell = peripheral horseshoe nuclei (NOT foreign-body giant cell = randomly arranged nuclei).
- Miliary TB = haematogenous dissemination → 1–2 mm millet-seed nodules in multiple organs.
- Scrofula = tuberculous cervical lymphadenitis → collar-stud abscess → sinus tract to skin.
- Pott's disease = vertebral TB → gibbus deformity + cold psoas abscess + paraplegia.
- Sterile pyuria (WBCs in urine, no bacterial growth on routine culture) = renal TB until proven otherwise.
- Mantoux test = Type IV DTH reaction; read at 48–72 hrs; induration (not erythema) assessed.
- MDR-TB = resistant to Rifampicin + Isoniazid; XDR-TB = MDR + fluoroquinolone + injectable resistance.
- In HIV with CD4 <200: TB presents with non-caseating granulomas (poor T-cell response) or no granulomas.
- Gold standard for diagnosis = culture; fastest confirmatory test = GeneXpert PCR.
- Standard treatment = HRZE × 2 months + HR × 4 months (6 months total — DOTS).
Sources: Robbins, Cotran & Kumar — Pathologic Basis of Disease (10th ed.), Chapter 8, pp. 350–360; Robbins & Kumar — Basic Pathology (11th ed.), Chapter 11, pp. 428–432.
Create a Word document with formatted exam notes including diagrams and tables
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.