patient with severe infective diarrhea from past 4 days has been on iv fluid for same days and had antibiotic tazobactam 4.5
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I have enough to give a thorough clinical analysis. Here is a structured assessment of this patient:
Clinical Assessment: Severe Infective Diarrhea — Day 4
The Clinical Situation
A patient has had severe infective diarrhea for 4 days, is on IV fluid replacement, and has received piperacillin-tazobactam (pip-tazo) 4.5 g (standard dose q8h or q6h depending on your regimen). Several important clinical questions arise at this stage.
1. Is Piperacillin-Tazobactam the Right Antibiotic?
Pip-tazo is a broad-spectrum beta-lactam/BLI with excellent activity against gram-negative enteric pathogens and anaerobes. It is not a first-line agent for community-acquired infective diarrhea, but may be appropriate if:
- The patient is severely ill / septic
- Intra-abdominal source is suspected
- Isolate is resistant to narrower agents
First-line empirical antibiotics for specific causes (per Rosen's Emergency Medicine):
| Organism | Preferred Antibiotic |
|---|---|
| Shigella | Ciprofloxacin 500 mg PO BD × 3 days OR Azithromycin 500 mg OD × 3 days |
| Salmonella typhi | Ciprofloxacin 500 mg BD × 7 days OR Ceftriaxone 1–2 g IV OD × 7 days |
| Non-typhoidal Salmonella (severe) | Levofloxacin 500 mg IV/PO OD × 7–10 days |
| Campylobacter | Azithromycin 500 mg OD × 3 days |
| ETEC (travelers' diarrhea) | Ciprofloxacin 750 mg once OR Rifaximin 200 mg TID × 3 days |
| V. cholerae | Doxycycline single dose up to 300 mg |
| STEC / E. coli O157:H7 | No antibiotics — increases HUS risk |
Pip-tazo is generally NOT listed as a specific agent for infective diarrhea. If used, it was likely for severity/sepsis cover or a specific susceptibility pattern.
Key question: Is stool culture / PCR panel available? Without pathogen identification, de-escalation or change of antibiotic direction cannot be guided rationally.
2. Has the Diarrhea Continued Despite 4 Days of Pip-Tazo? Critical Differentials:
🔴 C. difficile Infection (CDI) — Must Rule Out
"Risk factors for antibiotic-associated diarrhea include advanced age, use of broad-spectrum antibiotics... C. difficile colitis can be both severe and persistent in immunosuppressed patients." — Goldman-Cecil Medicine
Piperacillin-tazobactam is a broad-spectrum antibiotic that disrupts colonic flora and is a recognized risk factor for CDI. After 4 days of broad-spectrum therapy:
- Test stool for C. difficile (PCR/GDH + toxin EIA)
- Look for: watery/mucousy stools, leukocytosis, elevated creatinine, abdominal tenderness
- Onset can be from day 1 to weeks after antibiotics
- Critical warning: Assess for toxic megacolon — tachycardia, hypotension, distension, delirium
If CDI confirmed:
- Stop pip-tazo if possible
- Start oral vancomycin 125 mg QID × 10 days (first-line for non-severe CDI)
- Fidaxomicin 200 mg BD × 10 days (preferred for recurrence risk reduction)
- Metronidazole: inferior to vancomycin, used only if neither available
3. IV Fluid Management
"Patients who are severely dehydrated should receive an IV fluid bolus of isotonic solution, such as Lactated Ringer's (LR). Electrolytes should be replete, with particular attention to sodium and potassium levels." — Rosen's Emergency Medicine
After 4 days of ongoing diarrhea:
Monitor closely:
- Serum electrolytes — Na⁺, K⁺ (hypokalemia is common and dangerous), Cl⁻, HCO₃⁻
- Metabolic acidosis from bicarbonate losses in stool
- Renal function (creatinine, BUN) — pre-renal AKI from ongoing volume depletion
- Lactate if septic physiology suspected
Fluid choice:
- Lactated Ringer's is preferred over normal saline (avoids hyperchloremic acidosis)
- Switch to oral rehydration therapy (ORT) as soon as tolerated
4. What Should Happen Next — Stepwise Plan
| Priority | Action |
|---|---|
| Immediate | Send stool C. difficile PCR/toxin test |
| Immediate | Check electrolytes, renal function, CBC, CRP/procalcitonin |
| Immediate | Stool culture + sensitivity (if not already done) |
| Reassess antibiotic | Is pip-tazo justified? Consider de-escalation based on culture results |
| If CDI confirmed | Stop pip-tazo, start oral vancomycin |
| Monitor | Daily electrolyte replacement, fluid balance, urine output |
| If no improvement by day 5–7 | Re-evaluate — consider imaging (CT abdomen) to exclude complications: perforation, abscess, toxic megacolon |
| Nutritional support | Consider early enteral nutrition if prolonged illness |
5. Red Flag Signs Requiring Urgent Escalation
- Fever > 38.5°C with hypotension → Septic shock → Escalate antibiotics, blood cultures, ICU
- Abdominal distension + absent bowel sounds → Toxic megacolon
- Bloody diarrhea worsening → Severe dysentery, ischemic colitis
- Altered sensorium → Septic encephalopathy
Summary: At day 4, the most critical concern is C. difficile superinfection from broad-spectrum pip-tazo. If CDI is not the cause, stool culture should guide targeted antibiotic de-escalation. IV fluid management should focus on electrolyte correction (especially K⁺ and bicarbonate). Pip-tazo alone is not a standard agent for community infective diarrhea and should be reassessed against culture sensitivities.
Sources: Rosen's Emergency Medicine, Goldman-Cecil Medicine; Sherris & Ryan's Medical Microbiology 8e
patient had frver and hypotension also now is stable ... he had metronidazole orally after doscharge from hospital ... now taking nprfloxiccin and lactobacillus tablets ... has backache ... bear kidneys ...
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Now I have an excellent picture. Let me put this together.
Updated Clinical Picture — Post-Discharge
Reconstructing the Timeline
| Phase | Events |
|---|---|
| Days 1–4 (inpatient) | Severe infective diarrhea, fever, hypotension (septic shock), IV fluids, pip-tazo 4.5g |
| Discharge | Patient now stable, prescribed oral metronidazole |
| Currently | On norfloxacin + Lactobacillus (probiotic) tablets |
| New symptom | Backache + "bare kidneys" (renal angle/flank pain/tenderness) |
🔴 Most Likely Diagnosis: Acute Pyelonephritis / Urosepsis Post-Enteric Infection
The combination of backache + bare kidneys (costovertebral angle tenderness) in a patient who just recovered from severe enteric sepsis is highly suspicious for ascending urinary tract infection / acute pyelonephritis.
"The classic presentation [of acute pyelonephritis] is an abrupt onset of chills, fever, and unilateral or bilateral flank or costovertebral angle pain and/or tenderness... Acute pyelonephritis may also simulate GI tract abnormalities with abdominal pain, nausea, vomiting, and diarrhea." — Campbell-Walsh-Wein Urology
Why it fits:
- Enteric gram-negative bacteria (e.g., E. coli, Klebsiella, Salmonella) from the bowel can seed the urinary tract — especially after a severe enteric illness
- The prior gram-negative septicemia may have caused hematogenous seeding of the kidneys
- Norfloxacin is being prescribed — a fluoroquinolone used specifically for urinary tract infections (it achieves high urinary concentrations but low systemic levels, hence why it is chosen for UTI/pyelonephritis rather than systemic infection)
Why Norfloxacin?
Norfloxacin achieves excellent urinary tract concentrations and is appropriate for:
- Uncomplicated pyelonephritis / UTI caused by enteric gram-negatives
- Post-enteric UTI (ascending infection from gut flora)
"Three days of... norfloxacin for treatment of acute uncomplicated urinary infection..." — Brenner and Rector's The Kidney
Important caveat: Norfloxacin has poor systemic bioavailability — if the patient has signs of systemic illness (fever, high WBC, nausea/vomiting), they should be on ciprofloxacin or levofloxacin, or parenteral therapy. Norfloxacin is not adequate for complicated or systemic pyelonephritis.
Why Lactobacillus (Probiotic)?
After broad-spectrum pip-tazo → metronidazole, gut microbiota is severely disrupted. Lactobacillus is being used to:
- Restore normal colonic flora
- Prevent/treat antibiotic-associated diarrhea
- Reduce risk of C. difficile proliferation
This is appropriate and evidence-based practice.
Why Metronidazole Was Given at Discharge?
Metronidazole post-discharge was likely for one of:
- Anaerobic/gut coverage extension after pip-tazo (completing treatment)
- C. difficile prophylaxis or treatment — though oral vancomycin is now preferred for confirmed CDI
- Entamoeba histolytica — if amoebic dysentery was suspected (metronidazole is first-line)
Immediate Actions Needed
| Action | Reason |
|---|---|
| Urine routine + microscopy | Look for pyuria, bacteriuria, WBC casts (diagnostic of pyelonephritis) |
| Urine culture & sensitivity | Guide antibiotic — is norfloxacin appropriate? |
| Blood culture (if fever present) | Rule out bacteremia/urosepsis relapse |
| Renal function tests (creatinine, BUN) | Prior sepsis + volume depletion → AKI risk |
| Ultrasound kidneys/ureters | Exclude obstruction, abscess, hydronephrosis |
| Reassess norfloxacin | If systemic signs present → upgrade to ciprofloxacin 500 mg BD or levofloxacin 750 mg OD |
🚨 Upgrade Antibiotic If Any of These Are Present
Per Campbell-Walsh-Wein Urology:
"If a patient... is sufficiently ill to require hospitalization (high fever, high WBC count, vomiting, dehydration, evidence of sepsis)... a parenteral antibiotic is recommended: fluoroquinolone, aminoglycoside ± ampicillin, extended-spectrum cephalosporin ± aminoglycoside, or carbapenem."
- Ciprofloxacin 1000 mg XR OD × 7 days OR Levofloxacin 750 mg OD × 5–7 days for outpatient
- If re-hospitalized: IV ceftriaxone 1 g OD or IV ciprofloxacin until stable, then oral step-down × 10–14 days total
Summary
The "bare kidneys" (renal angle tenderness) + backache after severe enteric sepsis strongly points to acute pyelonephritis — likely from ascending or hematogenous spread of the enteric pathogen. Norfloxacin is a reasonable start for uncomplicated UTI, but must be reassessed against urine culture sensitivity. If the patient has any systemic signs, upgrade to ciprofloxacin/levofloxacin or IV therapy. Probiotic Lactobacillus is appropriate to restore gut flora post broad-spectrum antibiotics.
Sources: Campbell-Walsh-Wein Urology; Brenner and Rector's The Kidney; Goldman-Cecil Medicine
whatvare the causes pf backache .. and yeah norflox was not prescribed for uti because urine examination was normal
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Excellent. Now I have everything needed for a comprehensive, context-specific answer.
Important Clarification First: Norfloxacin Without UTI
Since urine examination is normal, norfloxacin here is being used as a gut-acting antibiotic — it achieves high luminal concentrations in the intestine but minimal systemic absorption. It is used for:
- Selective intestinal decontamination post-severe enteric infection
- Traveler's diarrhea / persistent enteric carrier state
- Prophylaxis in cirrhotic patients (SBP prevention)
This is a legitimate use. It is not for UTI in this patient.
Causes of Backache — General + In This Clinical Context
Here is the full differential, starting with what is most relevant to this patient:
🔴 MOST RELEVANT TO THIS PATIENT
1. Reactive Arthritis (Post-Enteric / Post-Dysentery)
"Enteric infections may precipitate a reactive arthritis (postdysentery reactive arthritis). Implicated agents are Salmonella, Shigella, Yersinia, and Campylobacter, and possible agents include E. coli and C. difficile." — Tintinalli's Emergency Medicine
- Occurs 2–6 weeks after enteric infection
- Presents as acute asymmetric oligoarthritis — lower limbs, sacroiliac joints, back and buttock pain
- Part of the spondyloarthropathy spectrum (formerly Reiter's syndrome)
- Normal urine fits — this is NOT a urinary cause
- Treatment: NSAIDs, rest; rheumatology referral
2. Prolonged Immobility / Deconditioned Muscles
- Patient was hospitalized for 4+ days on IV fluids, likely bedridden
- Paraspinal muscle strain / lumbar strain is the commonest cause of backache (70% of all cases)
- Exacerbated by lying in one position during illness
3. Hypokalemia-Related Muscle Weakness/Pain
- Severe diarrhea causes massive K⁺ loss in stool
- Hypokalemia → muscle cramps, generalized weakness, back muscle aches
- Check serum K⁺ — should have been replaced during admission
4. Perinephric Abscess / Renal Involvement
- Even with normal urinalysis, a perinephric abscess can exist (the infection is outside the collecting system, so urine may be sterile)
- The "bare kidneys" / flank tenderness sign still needs to be respected
- Requires ultrasound or CT to exclude
5. Vertebral Osteomyelitis / Septic Discitis
- After gram-negative bacteremia (this patient had sepsis with fever + hypotension), bacteria can seed the vertebral bodies
- Presents with deep, constant back pain, worse at rest/night, ± fever
- Rare but serious — needs MRI spine if suspected
- Listed in Goldman-Cecil's differential under "Nonmechanical spinal infections"
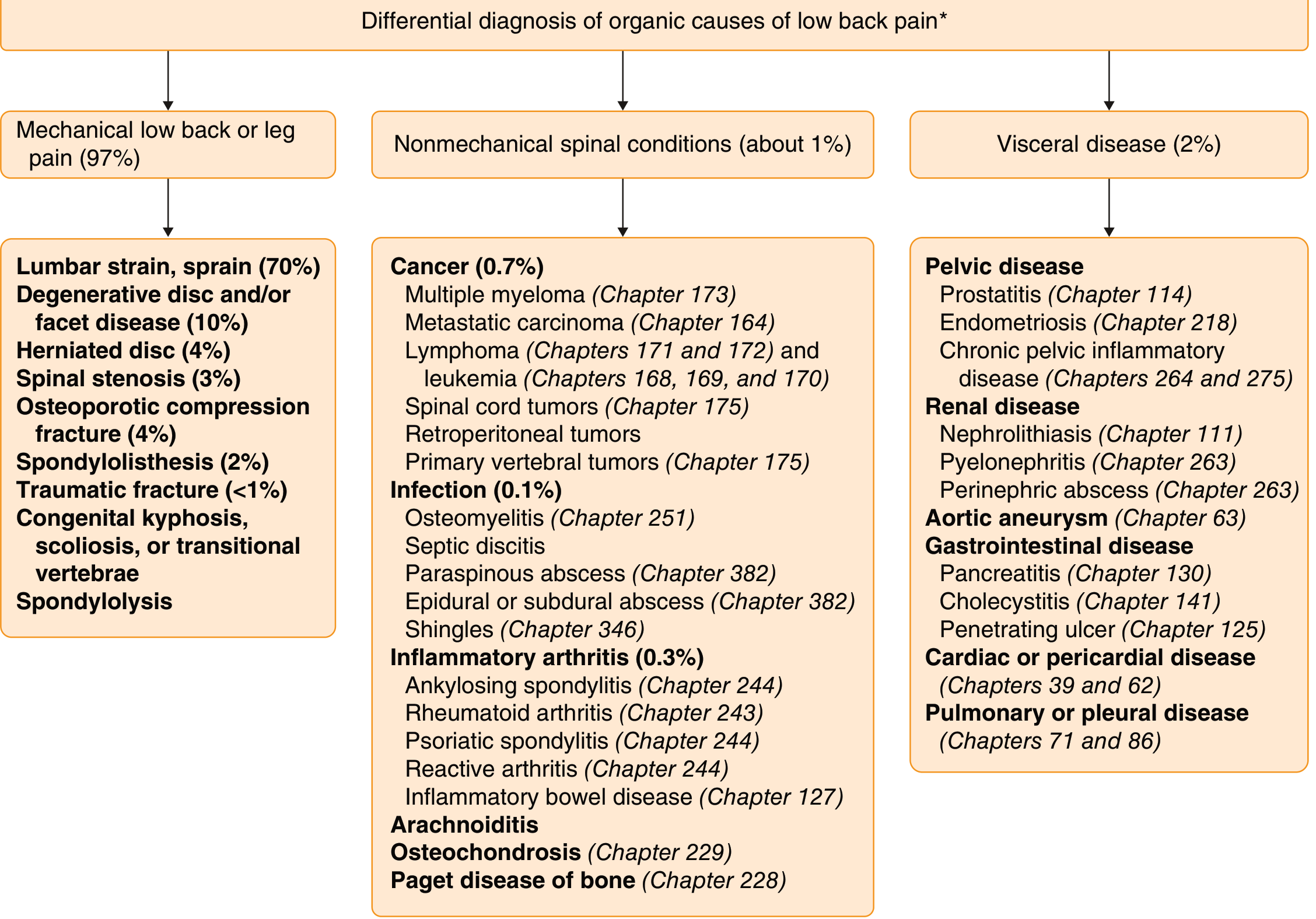
General Classification of Backache (for completeness)
| Category | Examples |
|---|---|
| Mechanical (97%) | Lumbar muscle strain (70%), disc herniation (4%), spinal stenosis (3%), osteoporotic fracture (4%), spondylolisthesis (2%) |
| Nonmechanical spinal | Osteomyelitis, septic discitis, paraspinous abscess, epidural abscess, ankylosing spondylitis, reactive arthritis, cancer (myeloma, metastases) |
| Visceral referred pain | Pyelonephritis, nephrolithiasis, perinephric abscess, pancreatitis, aortic aneurysm, pelvic disease |
What to Do Now
| Investigation | Looking For |
|---|---|
| Serum electrolytes (K⁺, Mg²⁺) | Hypokalemia from diarrhea |
| Ultrasound abdomen/kidneys | Perinephric collection, renal abscess, hydronephrosis |
| Serum CRP, ESR, CBC | Ongoing inflammation (reactive arthritis, discitis) |
| MRI spine (if deep bony pain) | Vertebral osteomyelitis / septic discitis |
| HLA-B27 (if arthritis suspected) | Reactive arthritis / spondyloarthropathy |
| Joint examination | Asymmetric oligoarthritis of lower limbs? |
Bottom line for this patient: The most likely cause is either reactive arthritis (post-enteric, caused by the same bug — Salmonella/Shigella/Campylobacter) presenting as back/sacroiliac pain 2–6 weeks post-illness, OR simple muscle pain from prolonged bed rest + hypokalemia. Perinephric abscess and vertebral osteomyelitis must be excluded given the prior sepsis, even with a normal urine exam.
Sources: Tintinalli's Emergency Medicine; Goldman-Cecil Medicine; Bradley & Daroff's Neurology in Clinical Practice
treatment
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have everything needed. Here is the treatment guide organized by diagnosis:
Treatment of Backache — Tailored to This Patient
Since the exact cause hasn't been confirmed yet, treatment is organized by most likely diagnosis first.
1. 🥇 Reactive Arthritis (Post-Enteric) — Most Likely
"Reactive arthritis generally occurs following infection with Salmonella, Shigella, Yersinia, or Campylobacter, with arthritis presenting 2–6 weeks after an episode of dysentery." — Rosen's Emergency Medicine
| Step | Treatment |
|---|---|
| First-line | NSAIDs — Ibuprofen 400–600 mg TDS with food, OR Naproxen 500 mg BD |
| If GI intolerance | Add PPI (omeprazole 20 mg OD) — especially important given recent gut illness |
| Joint rest | Avoid strenuous activity; gentle mobilization |
| Intra-articular steroids | If a specific joint is severely inflamed, rheumatologist can inject |
| Systemic steroids | Only if NSAIDs fail and diagnosis confirmed |
| Antibiotics | NOT indicated for post-enteric reactive arthritis — "antibiotics have not been shown to improve the clinical course in patients with reactive arthritis following dysentery" |
| DMARDs | Sulfasalazine, methotrexate — only if chronic/refractory (rheumatology decision) |
| Referral | Rheumatology for confirmation and long-term follow-up |
⚠️ This is self-limiting in most cases — resolves in 3–6 months. ~20% develop chronic disease.
2. Muscle Strain / Deconditioning (Simple Mechanical Backache)
| Step | Treatment |
|---|---|
| NSAIDs | Ibuprofen 400 mg TDS or Diclofenac 50 mg BD (short course, 5–7 days) |
| Muscle relaxants | Cyclobenzaprine or Methocarbamol if significant spasm |
| Heat therapy | Warm compress to lumbar region |
| Early mobilization | Bed rest is not recommended — gentle walking and movement speeds recovery |
| Physiotherapy | Stretching and core strengthening once acute phase settles |
3. Hypokalemia-Related Muscle Pain
| Treatment | Dose |
|---|---|
| Oral potassium supplementation | KCl slow-release 600–1200 mg (8–16 mEq) BD–TDS with meals |
| Potassium-rich diet | Banana, coconut water, orange juice, potatoes |
| If K⁺ < 2.5 mEq/L or symptomatic | IV potassium replacement under monitoring |
| Recheck electrolytes | After 48–72 hours |
4. If Vertebral Osteomyelitis / Septic Discitis is Suspected
"IV antibiotic treatment with coverage for S. aureus... MRI with IV contrast is the radiographic study of choice." — Rosen's Emergency Medicine / Miller's Orthopaedics
| Step | Treatment |
|---|---|
| Diagnose first | MRI spine with contrast + blood cultures + ESR/CRP |
| IV antibiotics | Cefazolin 2g IV q8h (MSSA cover) OR Vancomycin 15–20 mg/kg IV q8–12h (if MRSA risk) |
| Duration | 6 weeks IV antibiotics minimum |
| Surgery | If abscess forms or no response to medical treatment |
5. If Perinephric Abscess
| Step | Treatment |
|---|---|
| Diagnose | CT abdomen with contrast (most sensitive) |
| Drainage | Percutaneous CT-guided drainage (first-line) |
| Antibiotics | Gram-negative cover: pip-tazo 4.5g IV q8h OR ceftriaxone 2g IV OD |
| Duration | 2–4 weeks post-drainage |
Current Medications — Assessment
| Drug | Appropriate? | Comment |
|---|---|---|
| Norfloxacin | ✅ Yes | Gut decontamination / clearing enteric carrier state |
| Lactobacillus | ✅ Yes | Restore gut flora post broad-spectrum antibiotics |
| Metronidazole (completed) | ✅ Yes | Was for anaerobic/amoebic cover |
Add now:
- NSAID (ibuprofen/naproxen) + PPI for the backache — appropriate as first step
- Oral K⁺ supplementation pending electrolyte results
- Rheumatology referral if arthritis confirmed
Summary: Treat empirically with an NSAID + PPI now. Check electrolytes and replace K⁺. Order ultrasound abdomen to exclude perinephric collection. If deep constant bony back pain with night pain → MRI spine. If joint swelling develops → rheumatology for reactive arthritis confirmation.
Sources: Rosen's Emergency Medicine; Miller's Review of Orthopaedics 9e; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.