Explain pleomorphic adenoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pleomorphic adenoma"[MeSH Terms] AND salivary gland
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks along with histology images. Here is a thorough explanation:
Pleomorphic Adenoma
Also called benign mixed tumor, pleomorphic adenoma is the most common tumor of the salivary glands. The term "pleomorphic" refers to its remarkable histological diversity - it contains both epithelial and mesenchymal-like (stromal) elements, giving it a "mixed" appearance.
Epidemiology
- Most common salivary gland tumor overall (~50% of all salivary gland tumors)
- Annual incidence: ~2.4-3.05 per 100,000 population
- Most common between the 3rd and 6th decade; average age of presentation is 45 years
- Slightly more common in women
- Distribution by gland:
- Parotid gland: >80% of cases (most common site); represents ~65% of all parotid tumors
- Submandibular gland: less common
- Minor salivary glands: ~40% of intra-oral minor salivary gland tumors; most common site within the oral cavity is the hard palate
(Bailey and Love's Surgery 28th ed.; Scott-Brown's Otorhinolaryngology Vol 2)
Clinical Features
- Slow-growing, painless, firm, mobile, well-defined solitary mass
- Gradual progression over many years - can reach enormous proportions if untreated
- When arising from the deep lobe of the parotid, it may present as a paratonsillar bulge
- Occasionally presents as metachronous or synchronous tumors
- Warning signs of malignant transformation: sudden increase in size, facial nerve palsy, pain, fixation
(Bailey and Love's)
Macroscopic (Gross) Appearance
- Rounded or ovoid, well-demarcated mass, several centimeters in greatest dimension
- Variably encapsulated - capsule may be thick and fibrotic, attenuated, or even incomplete (especially on the palate)
- Cut surface: gray-white with myxoid and blue translucent chondroid areas
- May have areas of cystic change and calcification
- Protuberant pericapsular nodules may be seen, sometimes attached by a slender pedicle - these are key surgical pitfalls
(Robbins & Kumar Basic Pathology; Scott-Brown's)
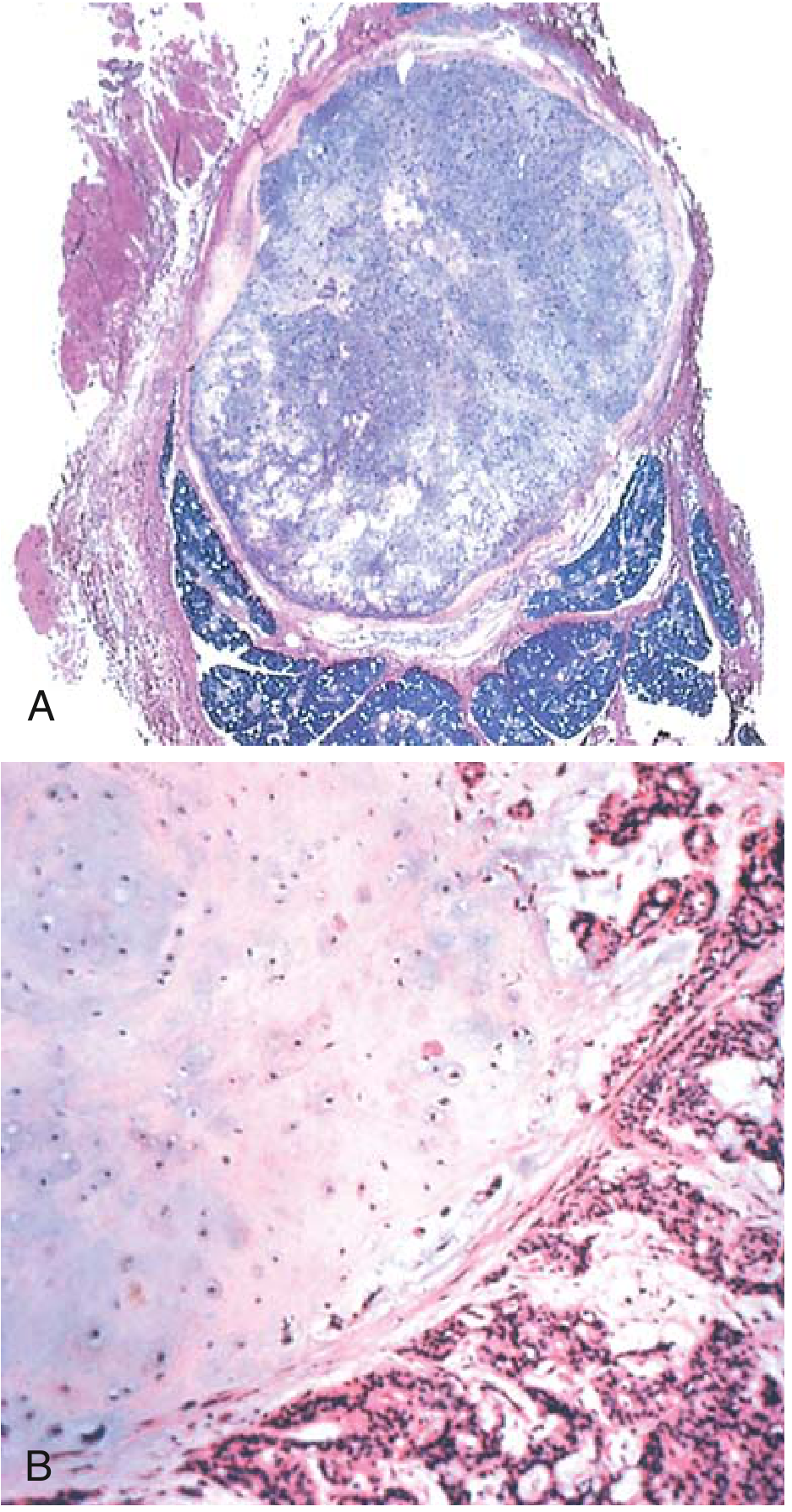
Microscopic (Histological) Appearance
The hallmark is remarkable heterogeneity - hence "pleomorphic":
Two basic components:
- Ductal (epithelial) and myoepithelial cells - arranged in ducts, acini, tubules, strands, or sheets
- Chondromyxoid stroma - loose myxoid tissue with islands of cartilage, and rarely foci of bone
Cellular appearances include:
- Oval, epithelioid, spindle-shaped, plasmacytoid, and clear cells in variable proportions
- Well-formed ducts lined by cuboidal-to-columnar luminal cells with an underlying layer of small, deeply chromatic myoepithelial cells
- Islands of well-differentiated squamous epithelium may be present
- No epithelial dysplasia or significant mitotic activity in benign cases
Superimposed changes may include:
- Metaplastic changes (squamous, lipomatous, osseous, neuroid, angiomatoid)
- Degeneration (cystic change, infarction, mineralization, hyalinization)
- Various growth patterns mimicking other tumors (adenoid cystic carcinoma-like, basaloid, clear cell, etc.) - this can make diagnosis from limited FNAB samples difficult
Immunohistochemistry:
- Luminal cells: CK7 (strong and diffuse)
- Myoepithelial cells: p63, S-100, SOX10, SMA
(Robbins Pathologic Basis of Disease; Bailey and Love's)
Histology Images
Surgical Considerations and Recurrence
- Treatment: complete surgical excision with a cuff of normal surrounding tissue (superficial or total parotidectomy with facial nerve preservation)
- Enucleation alone is inadequate and must be avoided - risks:
- Detaching pericapsular pseudopods/nodules (which remain in the field as nidi for recurrence)
- Capsular rupture, especially with predominantly myxoid tumors, which can spill semi-fluid tumor throughout the operative field
- Recurrence rates:
- After simple enucleation: ~25%
- After wider excision with cuff: ~4%
- Recurrences are typically multifocal due to seeding
- For oral cavity pleomorphic adenomas: transoral excision is appropriate
(Robbins Basic Pathology; Scott-Brown's; Cummings Otolaryngology)
Malignant Transformation: Carcinoma Ex Pleomorphic Adenoma
This is one of the most important complications:
- Overall risk: ~6% (Scott-Brown's) - Robbins cites 2% at <5 years rising to nearly 10% at >15 years
- Clinical warning signs: rapid growth, pain, facial nerve palsy, fixation
- Risk factors for transformation:
- Older patient age
- Male sex
- Long duration of tumor
- Multiple recurrences
- Deep lobe parotid location
- Histology: usually adenocarcinoma or undifferentiated carcinoma
- Prognosis: 30-50% mortality at 5 years - among the most aggressive salivary gland malignancies
- Carcinogenesis associated with frequent attempts at removal of recurrent benign disease - yet another reason to get the surgery right the first time
(Robbins Pathologic Basis of Disease; Scott-Brown's Otorhinolaryngology)
Summary Table
| Feature | Detail |
|---|---|
| Type | Benign epithelial tumor (benign mixed tumor) |
| Most common site | Parotid gland (>80%) |
| Presentation | Painless, slow-growing, mobile, firm mass |
| Hallmark histology | Epithelial + myoepithelial cells in chondromyxoid stroma |
| Capsule | Variable; often incomplete |
| IHC markers | Luminal: CK7; Myoepithelial: p63, S-100, SOX10, SMA |
| Treatment | Wide local excision (not enucleation) |
| Recurrence (enucleation) | ~25% |
| Recurrence (wide excision) | ~4% |
| Malignant transformation | ~6-10% (risk increases with duration) |
| Malignant form mortality | 30-50% at 5 years |
No recent meta-analyses or systematic reviews (last 2 years) were identified on PubMed that would contradict these established textbook findings.

541c2e82-7631-45ee-ad33-ee68bb1c1166.jpeg
Explain what given in picture
analyse_media
This is a page from the Textbook of Oral Pathology (page 430). It covers two main topics: the TNM Staging for salivary gland tumors, and the beginning of the Pleomorphic Adenoma chapter. Here is a full breakdown:
Part 1: TNM Staging of Salivary Gland Tumors (By American Joint Committee)
This is the classification system used to stage salivary gland tumors based on tumor size, lymph node spread, and distant spread.
Primary Tumor (T)
| Stage | Description |
|---|---|
| Tx | Tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| T1 | Tumor ≤2 cm, no significant local extension |
| T2 | Tumor 2-4 cm, no significant local extension |
| T3 | Tumor >4 cm but ≤6 cm, no significant local extension |
| T4a | Tumor >6 cm, no significant local extension |
| T4b | Tumor of any size WITH significant local extension |
Nodal Involvement (N)
| Stage | Description |
|---|---|
| Nx | Regional lymph node cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Clinically/histologically positive regional lymph nodes |
Distant Metastasis (M)
| Stage | Description |
|---|---|
| Mx | Cannot be assessed |
| M0 | No distant metastasis |
| M1 | Distant metastasis present |
Stage Grouping
| Stage | Criteria |
|---|---|
| Stage I | T1N0M0 or T2N0M0 |
| Stage II | T3N0M0 |
| Stage III | T1 or T2, N1M0; OR T4a or T4b, N0M0 |
| Stage IV | T3N1M0; T4a/T4b, N1M0; any T, any N, M1 |
Part 2: Pleomorphic Adenoma - Oral Pathology Perspective
Introduction
- Most common salivary gland tumor overall
- Term "pleomorphic adenoma" was coined by Willis, referring to the unusual histological pattern of the lesion
- The morphologically diverse appearance is its pathognomonic (defining) feature
- Derived from a mixture of ductal and myoepithelial elements
- It is the only tumor showing remarkable diversity both between different tumors AND within different areas of the same tumor
Why "Mixed Tumor"?
The tumor cells have the ability to differentiate into both epithelial and mesenchymal cells, producing a mixed picture of:
- Fibrous areas
- Hyalinised areas
- Chondroid (cartilage-like) areas
- Myxoid areas
- Epithelial cells with metaplasia
The term "mixed tumor" refers to this varied histopathological appearance - it does NOT mean the tumor is teratomatous (derived from germ cells).
Other Names for Pleomorphic Adenoma
- Iceberg tumor
- Endothelioma
- Branchioma
- Enchondroma
- Enclavoma
Histogenesis and Pathogenesis
The tumor is believed to arise from myoepithelial cells and intercalated duct reserve cells.
Two Main Theories:
1. Batsakis Theory
- Reserve cells of the intercalated duct differentiate into ductal and myoepithelial cells
- These then undergo mesenchymal metaplasia (transforming into cartilage, bone, etc.)
- The intercalated duct reserve cell is the histogenetic precursor of pleomorphic adenoma
2. Dardick's Theory
- Any neoplastically altered epithelial cell can differentiate in multiple directions (multidirectionally)
- Origin is NOT necessarily restricted to intercalated duct and myoepithelial cells
Clinical Features (beginning)
Sex and Age
- Women to men ratio: 6:4 (slight female predominance)
- Most common in the 4th to 6th decades, but can occur in young adults and children
Site
- Parotid gland: 90% of cases
- Lower pole of the superficial lobe of the parotid is the most commonly affected specific site
- Intraoral: palatal gland and lip
- Upper lip and buccal mucosa are very uncommonly affected
Appearance (partially visible)
- Palatal tumors present as smooth-surfaced, dome-shaped lesions
- Ulceration may be present (text cut off at the bottom of the page)
This page gives a nice oral pathology-specific view of pleomorphic adenoma, particularly the histogenesis theories (Batsakis and Dardick) which are commonly tested in dental and oral pathology exams.
analyse_media
This is a continuation of the Salivary Gland Pathology chapter on Pleomorphic Adenoma, covering its clinical presentation and histopathological features in detail. Here is the full explanation:
Pleomorphic Adenoma - Clinical Features (continued from previous page)
Mobility
- Palatal tumors are IMMOBILE - due to their location and tight microanatomy of the palate
- Lip and buccal mucosa tumors are MOBILE
- Parotid tumors are typically mobile (as seen in Fig. 17.18 - the elderly patient with a large parotid swelling)
Symptoms
- Starts as a small, painless, quiescent (quiet) nodule
- Slowly increases in size, sometimes intermittently (not constantly growing)
- Patient is usually aware of it for months to years before seeking help
- If neglected, can grow to a very large size (as shown in the photo - a man with a massive parotid tumor)
Shape
- Small tumor: round or oval
- As it grows: becomes lobulated (multi-nodular)
Size
- Parotid tumors can reach cricket ball size or larger, weighing in pounds
- Intraoral tumors: usually not more than 1-2 cm in diameter
Surface
- Surface is smooth
- Sometimes bosselated (covered in boss-like bumps)
- Occasionally crossed by deep furrows
Consistency
- Firm and rubbery to feel
- Sometimes cystic degeneration may be present (giving a softer feel)
Histopathological Features
Macroscopic (Gross) Appearance
(as shown in Fig. 17.19 - the cut specimen image)
- Encapsulated lesion with firm to rubbery consistency
- Minor salivary gland tumors may not have a well-defined capsule
- Cut surface shows a classic "cut potato" appearance - a key descriptive hallmark
- May be associated with:
- Small cystic areas
- Mucoid areas
- Hemorrhagic areas
The "cut potato appearance" is a classic exam answer for the gross appearance of pleomorphic adenoma.
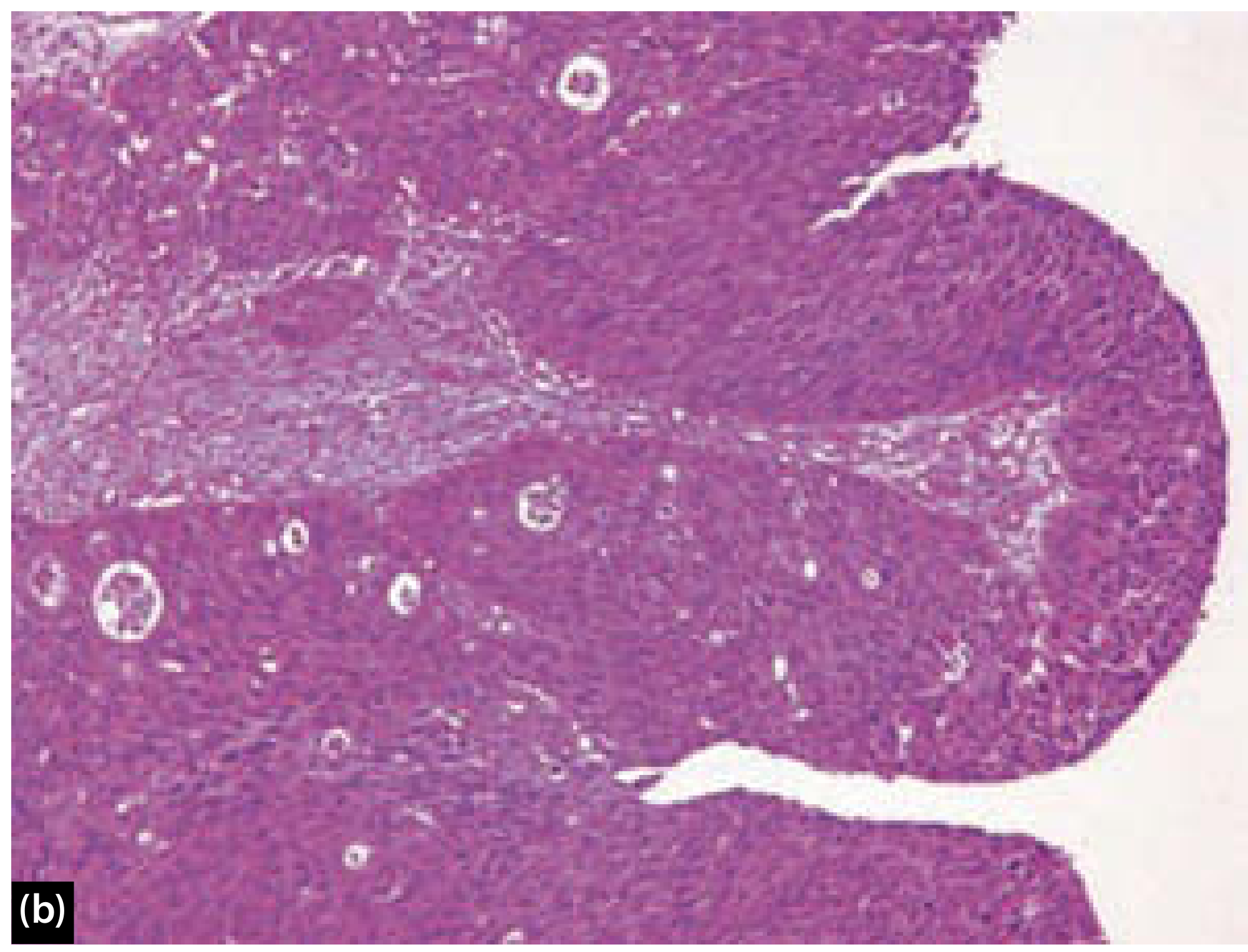
Microscopic Appearance
The tumor shows wide cytologic and architectural diversity. The tumor is typically:
- Well-circumscribed and encapsulated
- May show infiltration of the capsule by tumor cells (especially palatal tumors, which show infiltration of capsule beneath the epithelial surface)
- Considerable variation in arrangement of epithelial and stromal components between different areas of the same tumor
The tumor is described on the basis of 3 components:
1. Epithelial Cell Component
- Consists of: epithelial duct-like cells, polygonal cells, cuboidal cells, spindle cells
- Arranged in: sheets, clumps, islands, or interlacing strands
- Cuboidal cells show duct-like arrangement
- Duct-like spaces may contain eosinophilic coagulum and mucoid material
- Epithelial cells resembling squamous cells have distinct intercellular bridges
- Cystic spaces are uncommonly seen
2. Myoepithelial Cell Component
- Few stellate cells or spindle cells = myoepithelial cells
- Variable morphology
- Have rounded eccentric nucleus
- Have eosinophilic hyalinized cytoplasm - resembling plasma cells
- These are called plasmacytoid cells (or hyaline cells)
- Hyaline cells also seen with dense eosinophilic cytoplasm
Plasmacytoid (hyaline) myoepithelial cells are a characteristic feature of pleomorphic adenoma.
3. Stromal (Mesenchymal) Component
- Stromal changes are highly variable
- Believed to be produced by myoepithelial cells (text cuts off here)
- Typically includes: myxoid, chondroid (cartilage-like), hyalinized, and occasionally osseous (bone) areas
Summary of Key Points from This Page
| Feature | Detail |
|---|---|
| Symptoms | Painless, slow-growing, firm nodule |
| Size | Can reach cricket ball size; intraoral ≤2 cm |
| Shape | Round → lobulated as grows |
| Consistency | Firm, rubbery ± cystic |
| Gross appearance | Encapsulated, "cut potato" cut surface |
| Capsule | Present; may be infiltrated by tumor cells |
| 3 microscopic components | Epithelial + Myoepithelial + Stromal |
| Myoepithelial cells | Plasmacytoid appearance (key feature) |
| Stromal origin | Derived from myoepithelial cells |
analyse_media
This is page 432 from the Textbook of Oral Pathology, continuing the microscopic features of Pleomorphic Adenoma - specifically the Stromal Component and the Histological Classification. Here is the full explanation:
Stromal (Mesenchymal) Component - Continued
The stromal component is the "background" tissue of the tumor. It is highly variable and is produced by myoepithelial cells (which is why the stroma in pleomorphic adenoma is unique - it's not true mesenchyme but rather metaplastic change from epithelial cells).
What the stroma contains:
| Stromal Element | Description |
|---|---|
| Loose myxoid material | Wide intercellular spaces with faint staining - gives a "myxomatous appearance" |
| Hyalinized connective tissue (C.T.) | Foci of dense, glassy-looking material |
| Chondroid / cartilage-like areas | Blue translucent cartilage islands (key feature) |
| Osteoid / bone-like material | Seen between tumor cells (rarer finding) |
| Mucoid deposition | Background stroma with mucoid material = myxomatous appearance |
The presence of chondroid (cartilage) in a salivary gland tumor is a hallmark of pleomorphic adenoma, because cartilage does not normally exist in salivary glands. It is produced by the metaplastic activity of myoepithelial cells.
Special Terminology Based on Predominant Component
Depending on which component predominates, the tumor may be called by different names:
| If Predominant Component is... | The Tumor is Called... |
|---|---|
| Highly cellular / predominantly epithelial | Cellular adenoma |
| Predominantly myoepithelial cells | Myoepithelioma |
| Stroma with mucoid deposition | Shows myxomatous appearance |
| Myoepithelial cells with plasma cell-like appearance | Plasmacytoid myoepithelial cells |
Histological Types of Pleomorphic Adenoma
(Foot and Frazel Classification, 1954)
This is the classic histological classification based on the ratio of myxoid (stromal) to cellular (epithelial) components:
| Type | Description |
|---|---|
| 1. Principally myxoid | Mostly myxoid stroma; least cellular |
| 2. Myxoid-cellular in equal proportions | Balanced mixture of stroma and cells |
| 3. Predominantly cellular | Mostly cellular; less stroma |
| 4. Extremely cellular | Almost entirely cellular; very little stroma |
This classification matters clinically: Principally myxoid tumors are the most dangerous during surgery - they are semi-fluid and capsular rupture during removal can spill tumor cells, leading to multifocal recurrence.
Figure Descriptions (Histology Images on This Page)
Fig. 17.20 - Shows:
- D = Duct-like spaces
- E = Eosinophilic material filling the ducts
- M = Mucous acini (peripherally placed)
- C = Capsule surrounding the tumor
Fig. 17.21 - Shows:
- Chondroid (cartilage-like) areas within the stroma - the blue/grey material that is characteristic of pleomorphic adenoma
Fig. 17.22 - Shows:
- D = Ductal spaces filled with eosinophilic material
- C = Chondroid areas clearly visible adjacent to ducts
Fig. 17.23 - Shows (two key features together):
- C = Chondroid areas
- SM = Squamous metaplasia - islands of squamous epithelium within the tumor (another hallmark feature)
Quick Summary of This Page
Stromal component of Pleomorphic Adenoma:
├── Myxoid material (most common stromal element)
├── Hyalinized CT
├── Chondroid / cartilage islands ← KEY FEATURE
├── Osteoid / bone (rare)
└── All produced by MYOEPITHELIAL CELLS
Special names:
├── Epithelial dominant → Cellular adenoma
└── Myoepithelial dominant → Myoepithelioma
Histological types (Foot & Frazel 1954):
1. Principally myxoid
2. Equal myxoid + cellular
3. Predominantly cellular
4. Extremely cellular
The microscopic photos on this page beautifully demonstrate the three components together - ducts (epithelial), chondroid stroma, squamous metaplasia islands, and eosinophilic material - all in the same tumor, which is why it is called "pleomorphic" (many forms).
This is a shared conversation. Sign in to Orris to start your own chat.