Classification and grading of neuroendocrine neoplasm of git
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
neuroendocrine neoplasm gastrointestinal classification grading WHO
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the key information needed for a comprehensive answer. Let me compile the full response.
Classification and Grading of Neuroendocrine Neoplasms (NENs) of the GIT
Overview and Terminology
The term "carcinoid" is now obsolete as a general label. The 2019 WHO classification introduced a uniform framework that divides all gastrointestinal/pancreatic neuroendocrine neoplasms (GI-PaNENs) into two biologically distinct groups based on differentiation:
- Well-differentiated neuroendocrine tumors (NETs) - previously called "carcinoid tumors" in the GI tract
- Poorly differentiated neuroendocrine carcinomas (NECs) - high-grade, aggressive tumors
This distinction carries major prognostic and therapeutic implications. The 2019 WHO classification framework replaced the older site-specific systems that caused confusion across GI subsites.
WHO 2019 Classification Framework
| Category | Differentiation | Grade | Behavior |
|---|---|---|---|
| NET G1 | Well-differentiated | Low | Indolent |
| NET G2 | Well-differentiated | Intermediate | Intermediate |
| NET G3 | Well-differentiated | High | Aggressive |
| NEC (small cell type) | Poorly differentiated | High | Very aggressive |
| NEC (large cell type) | Poorly differentiated | High | Very aggressive |
| MiNEN | Mixed | Variable | Variable |
- Yamada's Textbook of Gastroenterology, 7th ed.
- Goldman-Cecil Medicine International Edition
Grading System (WHO 2019)
The grading of well-differentiated NETs uses two parameters: mitotic count and Ki-67 proliferation index. When the two parameters give discordant grades, the higher grade is assigned.
| Grade | Mitotic Count (per 2 mm²) | Ki-67 Index | Behavior |
|---|---|---|---|
| G1 | < 2 mitoses/2 mm² | < 2% | Low-grade, indolent |
| G2 | 2-20 mitoses/2 mm² | 3-20% | Intermediate-grade |
| G3 | > 20 mitoses/2 mm² | > 20% | High-grade (well-differentiated) |
NECs are by definition high-grade (> 20 mitoses/2 mm² and > 20% Ki-67) but are poorly differentiated - a critical distinction from G3 NETs.
Key point: G3 NETs and high-grade NECs both have high mitotic rates, but differ in morphology, molecular genetics, and treatment response. G3 NETs often respond to somatostatin analogues/everolimus, while NECs are treated like small-cell lung cancer (platinum-based regimens).
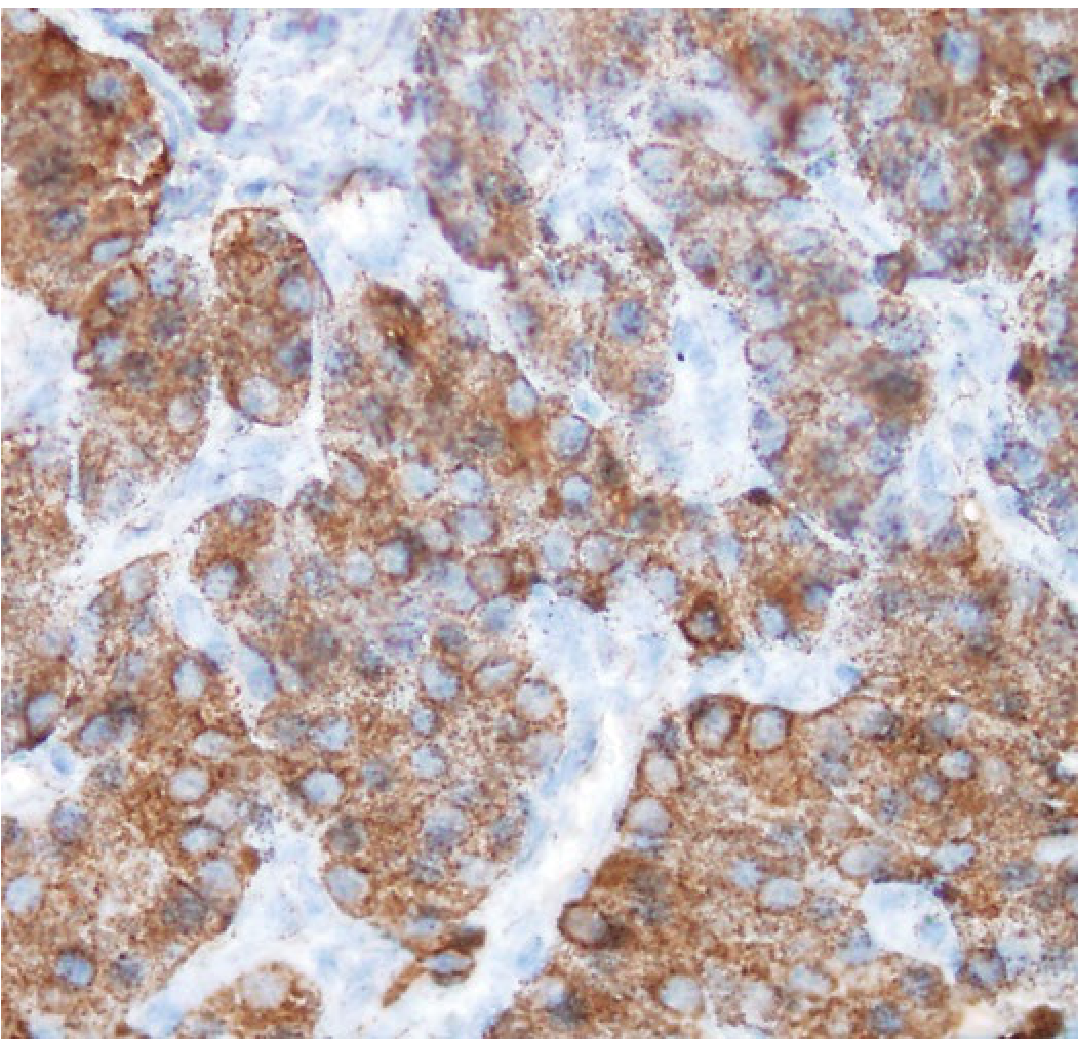
Immunohistochemical Markers
All NENs are defined by expression of general neuroendocrine markers on IHC:
- Chromogranin A (most specific)
- Synaptophysin (most sensitive)
- Neuron-specific enolase (NSE)
Ultrastructurally, they contain electron-dense cytoplasmic secretory granules.
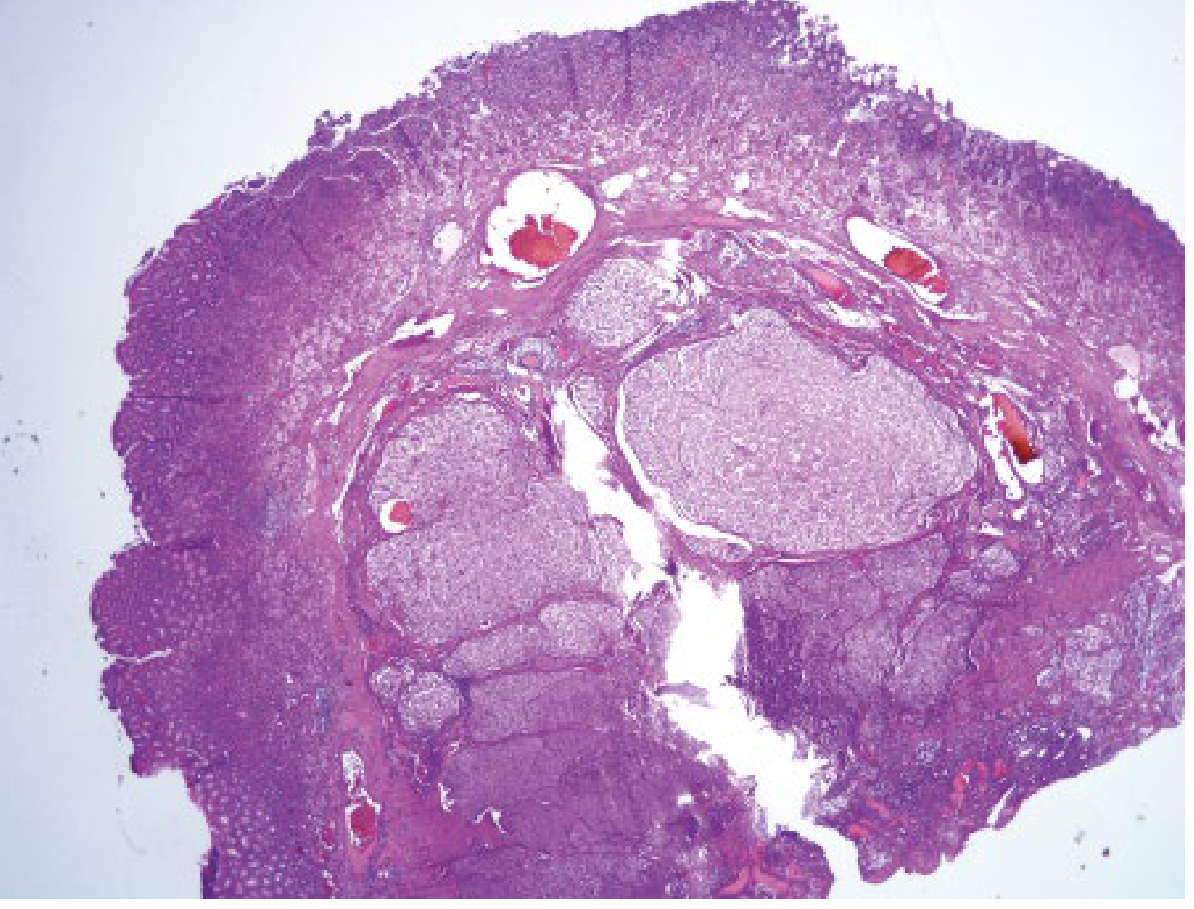
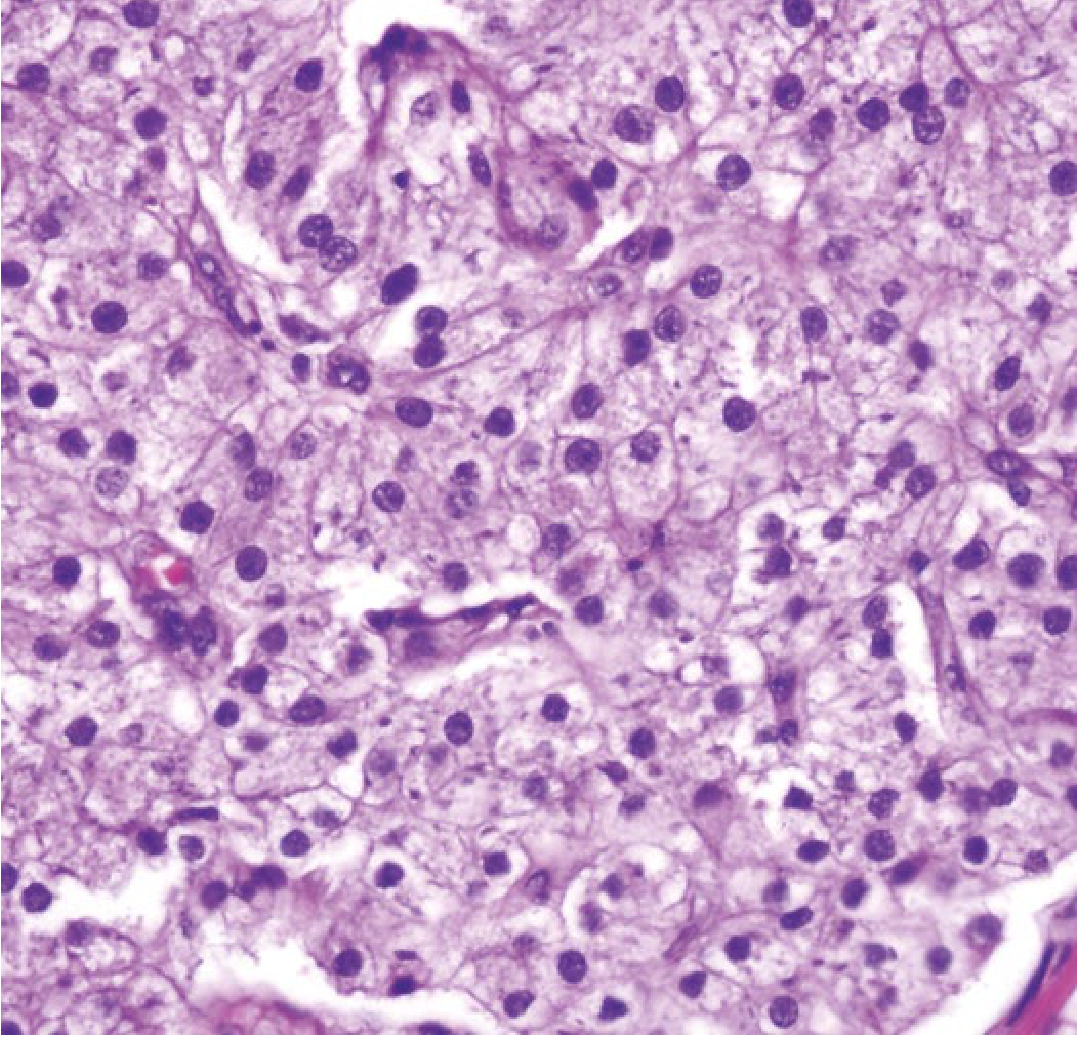
Histologic appearance (well-differentiated NET):
Site-Specific Classification of GI NETs
1. Gastric NETs (ECL-cell tumors) - Three-Type Classification
| Type | Background | Gastrin Level | Malignant Potential | Management |
|---|---|---|---|---|
| Type I (80-90%) | Chronic atrophic gastritis (autoimmune) | High (reactive hypergastrinemia) | Low (<5% metastasis) | Endoscopic resection, surveillance |
| Type II (5-7%) | ZES + MEN1 (gastrinoma-driven) | High (from gastrinoma) | Intermediate | Treat underlying gastrinoma |
| Type III (10-15%) | Sporadic - no hypergastrinemia | Normal | High (>50% metastasis) | Surgical resection |
- Types I and II are driven by hypergastrinemia causing enterochromaffin-like (ECL) cell hyperplasia and are relatively benign
- Type III sporadic gastric NETs require aggressive surgical management
- Gastric NECs (poorly differentiated) account for ~21% of all gastric NENs, predominantly in males
2. Small Intestinal NETs (most common NEN overall)
- Account for 35-45% of all GI NETs; most within 60 cm of the ileocecal valve
- Derived from enterochromaffin (Kulchitsky) cells in crypts of Lieberkühn
- At presentation: 40% have multifocal tumors >2 cm, 70% have invaded muscularis propria, 50% have liver metastases
- Often cause carcinoid syndrome (flushing, diarrhea, wheezing) when liver metastases are present - serotonin bypass hepatic inactivation
- On CT: hyperenhancing lesions (vs. adenocarcinoma which is moderately enhancing); can cause desmoplastic mesenteric reaction
3. Pancreatic NETs (pNETs/pNENs)
Subdivided into functional (secrete active hormones) and nonfunctional (60-80% of all pNENs):
Functional pNETs:
| Tumor | Syndrome | Location | Malignancy Rate |
|---|---|---|---|
| Gastrinoma | Zollinger-Ellison syndrome | Duodenum (70-90%), Pancreas (10-30%) | 60-90% |
| Insulinoma | Hypoglycemia | Pancreas (100%) | 5-15% |
| Glucagonoma | Diabetes, necrolytic migratory erythema | Pancreas (100%) | 60% |
| VIPoma | Verner-Morrison (WDHA) | Pancreas (90%) | 80% |
| Somatostatinoma | Diabetes, cholelithiasis, diarrhea | Pancreas (56%), Duodenum/jejunum (44%) | 60% |
| GRFoma | Acromegaly | Lung (54%), Pancreas (30%) | 30% |
| ACTHoma | Cushing syndrome | Pancreas (4-16% of ectopic Cushing) | >95% |
Hereditary syndromes associated with pNENs:
- MEN1: 80-100% develop pNENs
- VHL: 10-17%
- Tuberous sclerosis: 0.5%
- NF-1 (von Recklinghausen): 12% develop duodenal somatostatinomas
4. Appendiceal NETs
- Most are found incidentally, typically < 2 cm at the tip
- Tumors < 2 cm: < 2% metastatic risk; > 2 cm: significantly higher risk
- Previously the most common GI NEN but now surpassed by ileal NETs in prevalence
5. Rectal NETs
- Usually small, submucosal, discovered incidentally on colonoscopy
- Low malignant potential if < 1 cm; endoscopic resection generally curative
NEC vs. NET: Key Differences
| Feature | Well-differentiated NET | Poorly differentiated NEC |
|---|---|---|
| Architecture | Organoid (nests, cords, ribbons) | Diffuse, sheet-like |
| Nuclear atypia | Mild, uniform | Severe, pleomorphic |
| Necrosis | Minimal | Extensive |
| Ki-67 | Variable (G1-G3) | Always > 20% |
| Chromogranin | Positive (strong) | Often focal/weak |
| Synaptophysin | Positive | Positive |
| Genetics | MEN1, DAXX/ATRX, mTOR | TP53, RB1 mutations |
| Treatment | Somatostatin analogues, targeted therapy | Platinum/etoposide chemotherapy |
Mixed Neuroendocrine-Non-Neuroendocrine Neoplasms (MiNEN)
A category where both neuroendocrine and non-neuroendocrine components each comprise ≥ 30% of the tumor. Common examples include:
- Adenocarcinoma + NEC (most common in colorectum)
- MANEC (mixed adenoneuroendocrine carcinoma) - older term
Molecular Alterations
| Tumor Type | Key Genetic Alterations |
|---|---|
| Well-differentiated NET | MEN1, DAXX/ATRX, mTOR pathway genes, PTEN loss |
| Poorly differentiated NEC | TP53 mutations, RB1 mutations |
| pNENs (familial) | MEN1, VHL, TSC1/TSC2, NF1 |
Summary
The 2019 WHO classification replaced the old "carcinoid" framework with a two-tier differentiation system (NET vs. NEC) and a three-grade system (G1, G2, G3) based on Ki-67 and mitotic count. This is clinically relevant because:
- Grade determines prognosis and surveillance intensity
- Differentiation (well vs. poorly) determines the chemotherapy backbone
- Gastric NETs have an additional site-specific three-type classification (I, II, III) based on the background gastrin milieu
Sources:
- Yamada's Textbook of Gastroenterology, 7th ed., pp. 2947-2948
- Goldman-Cecil Medicine International Edition, Chapter 213
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Current Surgical Therapy, 14th ed.
- Klöppel G. Neuroendocrine Neoplasms: Dichotomy, Origin and Classifications. Visc Med 2017 (PMID 29177160)
- WHO 2019 Classification update - Arends et al., Histopathology 2026 (PMID 41724188)
This is a shared conversation. Sign in to Orris to start your own chat.