Describe the clinical tests and modern investigation used to diagnose vericose veins. Discuss their significance.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the complete answer.
Diagnosis of Varicose Veins: Clinical Tests and Modern Investigations
Varicose veins are tortuous, dilated, and elongated superficial veins resulting primarily from incompetent valves - most commonly at the saphenofemoral junction (GSV system, ~60%) or saphenopopliteal junction (SSV system, ~20%). Diagnosis proceeds in two stages: clinical assessment and modern investigations.
Part I - Clinical Assessment
History
Patients report aching, heaviness, throbbing, burning or bursting over affected areas, worsening throughout the day and with prolonged standing, and relieved by leg elevation or compression hosiery. Itching, ankle swelling, and cosmetic concern are common. Symptoms may be severe yet independent of the degree of incompetence. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Inspection and Palpation
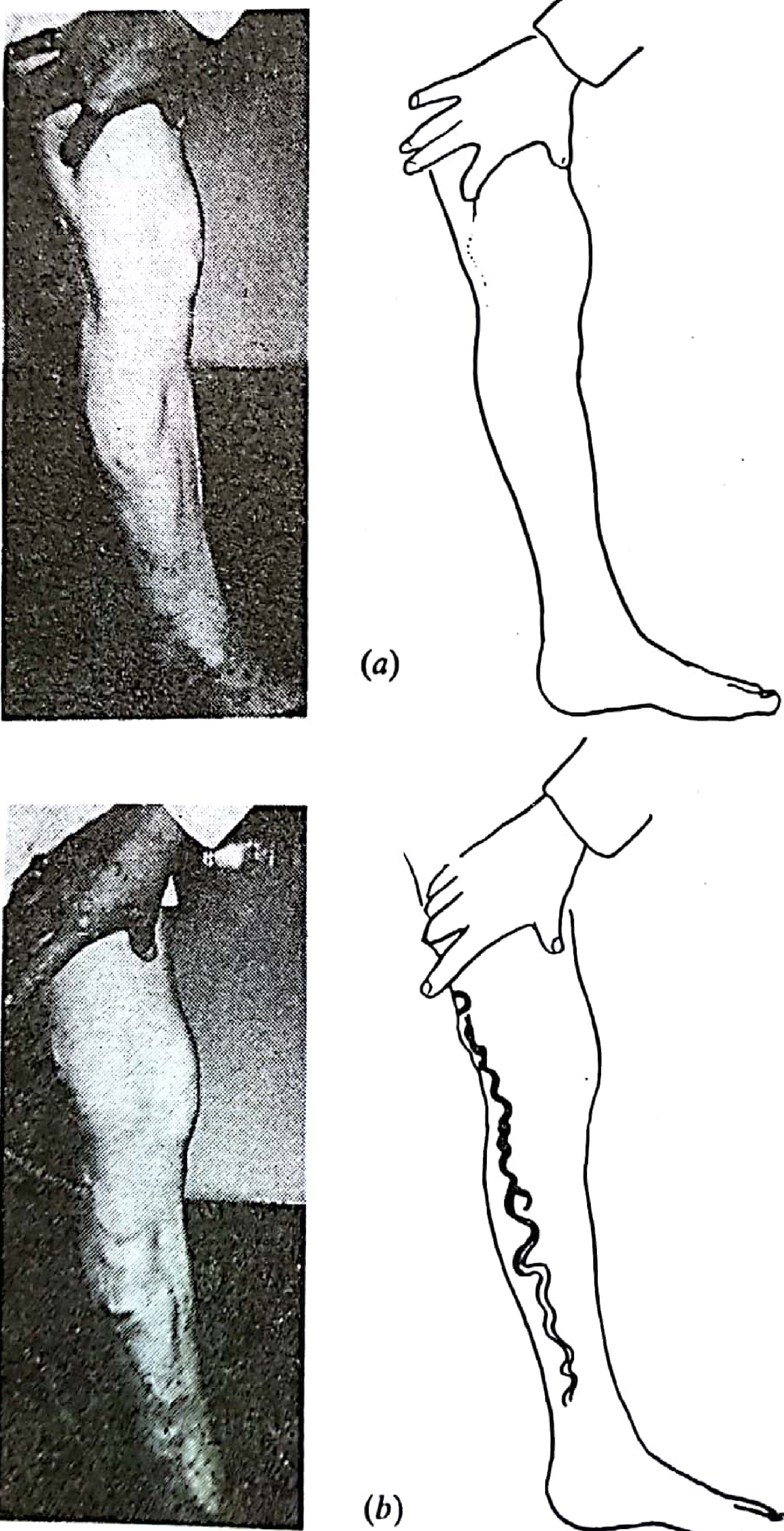
- Tortuous, dilated subcutaneous veins visible on standing
- Distribution suggests the affected axis: medial thigh/calf = GSV; posterolateral calf = SSV; anterolateral thigh/calf = anterior accessory GSV (AAGSV)
- A saphena varix (dilated SFJ blowout) appears as a painless groin lump that disappears on recumbency - distinguished from a femoral hernia by its disappearance when lying flat and by eliciting a fluid thrill on tapping lower varices
- Skin changes: hyperpigmentation, lipodermatosclerosis, venous eczema, healed/active ulcers in the gaiter area
Part II - Classical Clinical Tests
1. Brodie-Trendelenburg Test (Tourniquet Test)
Procedure: The patient lies supine; the leg is elevated to drain the veins. A tourniquet is applied to the proximal thigh, and the patient stands.
Interpretation:
| Observation | Interpretation |
|---|---|
| Veins remain empty while tourniquet is on, then fill promptly on release | SFJ incompetence - primary varicose veins |
| Veins fill rapidly from below within 30 s despite the tourniquet | Deep vein incompetence or incompetent perforators below the tourniquet |
| Veins fill slowly from below but rapidly on releasing tourniquet | Both SFJ incompetence AND perforator incompetence |
Significance: This is the foundational test to localise the dominant point of venous incompetence and to differentiate primary (superficial) from secondary (deep) varicose veins. By moving the tourniquet to successively lower levels (e.g., above the knee, below the knee), the clinician can map incompetent perforators. - Harrison's Principles of Internal Medicine, 22nd Ed.; Pye's Surgical Handicraft, 22nd Ed.
2. Perthes' Test
Procedure: A tourniquet is placed at the mid-thigh after the patient has stood (i.e., with veins filled). The patient walks for 5 minutes.
Interpretation:
| Observation | Interpretation |
|---|---|
| Superficial veins collapse | Deep veins are patent; perforators are competent - safe to strip |
| Superficial veins remain filled | Deep vein patent but perforators are incompetent |
| Superficial veins distend further and become painful | Deep vein obstruction - stripping is CONTRAINDICATED |
Significance: Perthes' test is the key pre-operative safety test. A positive result (worsening distension with walking) indicates the patient depends on superficial veins for venous return due to a blocked deep system - intervention on the varicosities in this setting could precipitate limb-threatening venous hypertension. - Harrison's Principles of Internal Medicine, 22nd Ed.
3. Cough Impulse Test
Procedure: The examiner places a finger over the saphenofemoral junction (SFJ) in the groin, and the patient coughs.
Significance: A transmitted impulse (palpable thrill) at the SFJ confirms a patent, incompetent channel from the abdomen to the superficial venous system. It is a quick bedside confirmation of SFJ incompetence. Similarly, a saphena varix will show a cough impulse and can be distinguished from a femoral hernia (which would give an expansile impulse, not a venous thrill). - Pye's Surgical Handicraft, 22nd Ed.
4. Percussion (Tap) Test / Schwartz Test
Procedure: The examiner taps the varicosities at one point while palpating proximally or distally along the vein.
Significance: A transmitted fluid thrill confirms continuity of the varicose venous trunk. It is useful to establish that an apparently separate cluster of varicosities is in fact connected to the main venous trunk - important for deciding the extent of surgical avulsion. - Pye's Surgical Handicraft, 22nd Ed.
5. Fegan's Test (Tourniquet + Perforator Localisation)
Procedure: After elevating the leg, the examiner systematically palpates for fascial defects along the medial and posterior calf. Small pits or indentations in the deep fascia can be felt, corresponding to sites where dilated perforating veins have punched through.
Significance: Localises incompetent perforating veins prior to operation, guiding the level of subfascial ligation. Accurate localisation reduces recurrence by ensuring all feeding perforators are addressed.
6. Morrissey's Test (Retrograde Filling Test)
A simpler variant of the Trendelenburg test - the leg is elevated, the GSV compressed at the groin, and the patient stands. Rapid retrograde filling of the vein distal to the compression on releasing the finger confirms reflux from the SFJ. It is a quick bedside confirmation of SFJ incompetence.
Part III - Modern Investigations
1. Duplex Ultrasound Scanning (DUS) - The Gold Standard
This is the principal and now mandatory diagnostic investigation for all patients with varicose veins prior to any intervention. Bailey & Love states plainly: "There is good evidence to support the policy of duplex ultrasound scanning for all patients with varicose veins prior to any intervention." Tourniquet tests and hand-held Doppler have largely been abandoned in favour of DUS. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Equipment: High-frequency linear array transducer (7.5-13 MHz); patient stands facing the examiner with the leg externally rotated.
What duplex ultrasound establishes:
| Parameter | Technique |
|---|---|
| Reflux in deep and superficial system | B-mode + spectral/colour Doppler |
| Exact distribution of reflux (junction involved, perforators) | Whole-leg mapping |
| Obstruction in deep system | Absence of flow; echogenic thrombus; failure to compress |
| Suitability for treatment (diameter, extent, tortuosity) | B-mode measurement |
| Thrombus within superficial veins | B-mode |
| Anatomical variants | Longitudinal survey |
Diagnostic thresholds for reflux:
- Superficial / crural veins: retrograde flow lasting ≥ 0.5 seconds
- Proximal deep veins: retrograde flow lasting ≥ 1 second
Reflux is elicited by calf/foot squeeze and release, Valsalva manoeuvre, or pneumatic cuff deflation.
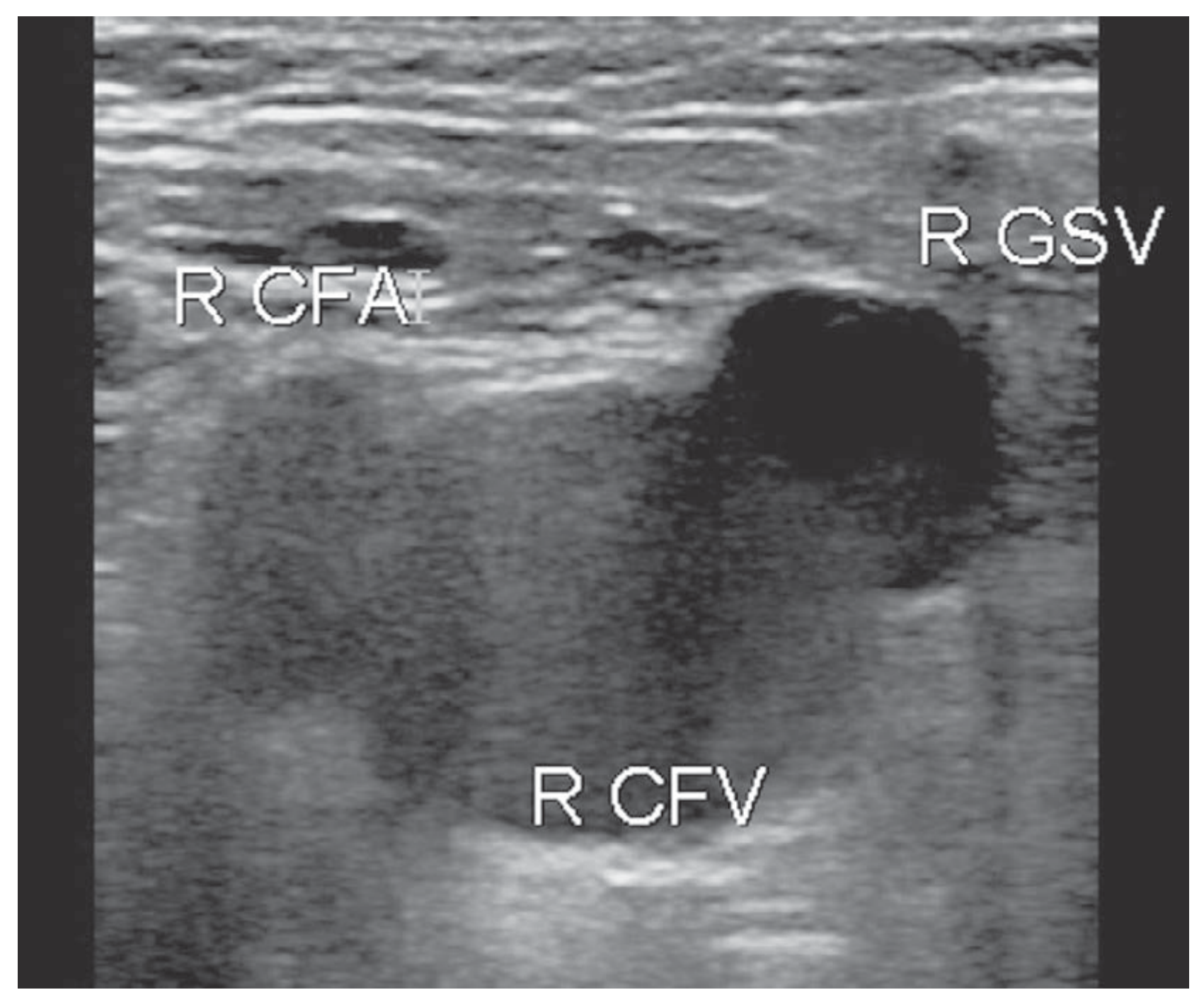
Landmark finding at the SFJ - the 'Mickey Mouse' sign: In transverse B-mode at the groin, the common femoral artery (CFA), common femoral vein (CFV), and great saphenous vein (GSV) form a characteristic three-circle pattern resembling Mickey Mouse's head and ears.
Significance of DUS:
- Provides a precise anatomical map of incompetence, guiding personalised treatment planning
- Detects concurrent deep vein obstruction or reflux (contraindication to superficial vein ablation)
- Determines suitability for endovenous procedures vs. open surgery
- Guides real-time ultrasound-guided endovenous thermal ablation (EVLA/RFA)
- Identifies recurrence patterns and sources (incompetent thigh perforators, pelvic reflux)
- Colour Doppler uses: blue = antegrade (toward heart); red = retrograde (reflux)
- Bailey and Love's Short Practice of Surgery, 28th Ed.; Harrison's Principles of Internal Medicine, 22nd Ed.
2. Hand-held (Continuous Wave) Doppler
A simple 8-10 MHz Doppler probe placed over the SFJ or SPJ with calf augmentation. A biphasic signal (forward flow + reversal) indicates reflux.
Current status: Previously used widely as a screening tool at the bedside and clinic. Now largely superseded by duplex ultrasound, which provides anatomical detail CW Doppler cannot. Bailey & Love notes these have been "abandoned" in favour of duplex scanning. Still useful as a rapid screening tool in primary care or to confirm significant SFJ/SPJ reflux before formal duplex. - Pye's Surgical Handicraft, 22nd Ed.
3. Venous Plethysmography (Photoplethysmography / Air Plethysmography)
Plethysmography measures global venous function:
- Photoplethysmography (PPG): Infrared sensor on the ankle measures skin blood volume changes with calf exercises; calculates venous refilling time (VRT). A VRT < 25 seconds suggests significant venous insufficiency.
- Air plethysmography (APG): Measures ambulatory venous pressure indirectly via a pneumatic cuff on the leg during standing and walking, giving the venous filling index (VFI) and ejection fraction (EF).
Significance: Provides physiological (functional) information rather than anatomical. Useful for quantifying overall venous insufficiency severity, pre- and post-operative comparison, and research settings. Less used in routine clinical practice since DUS provides both anatomy and functional data.
4. Varicography (Ascending/Descending Venography)
Contrast medium is injected into a varicosity (varicography) or the femoral vein (descending venography) and X-ray screening performed.
Significance: Largely historical - used to map complex or recurrent varicosities prior to redo surgery, or to identify unusual sources of reflux (pelvic veins, pudendal connections). Largely replaced by duplex ultrasound, which achieves the same mapping non-invasively. Still occasionally used in highly complex recurrent cases or suspected pelvic congestion syndrome.
5. CT / MR Venography
Cross-sectional imaging of the venous system using computed tomography (CTV) or magnetic resonance (MRV) with contrast.
Significance: Indicated for:
- Suspected pelvic vein incompetence or pelvic congestion syndrome as a source of vulval/perineal varicosities
- Deep vein obstruction (iliac vein compression / May-Thurner syndrome)
- Post-thrombotic syndrome evaluation
- Recurrent varicose veins where a pelvic source is suspected
Not used as a primary test for simple varicose veins.
6. CEAP Classification (Clinical Severity Scoring)
While not an investigation per se, modern assessment of chronic venous disease now formally uses the CEAP (Clinical, Etiologic, Anatomic, Pathophysiologic) classification to standardise description and guide management:
| CEAP Class | Clinical Features |
|---|---|
| C0 | No visible or palpable signs |
| C1 | Telangiectasias / reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4 | Skin changes (pigmentation, eczema, lipodermatosclerosis) |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
The CEAP classification is supplemented by the Venous Clinical Severity Score (VCSS), a quantitative tool for tracking change over time and response to treatment. - Harrison's Principles of Internal Medicine, 22nd Ed.
Summary Table
| Test/Investigation | Type | What It Detects | Significance |
|---|---|---|---|
| Trendelenburg/Brodie test | Clinical | Level of incompetence (SFJ vs. perforators) | Localises source; differentiates primary vs. secondary |
| Perthes' test | Clinical | Deep vein patency | Safety test - rules out deep obstruction before surgery |
| Cough impulse | Clinical | SFJ incompetence, saphena varix | Quick confirmation; distinguishes from femoral hernia |
| Tap/Schwartz test | Clinical | Vein continuity | Maps connected varicose tributaries |
| Fegan's test | Clinical | Perforator sites | Localises perforators for surgical ligation |
| Duplex ultrasound | Modern (1st line) | Reflux + anatomy + obstruction | Gold standard; mandatory pre-treatment; guides ablation |
| Hand-held Doppler | Modern (screening) | Reflux at SFJ/SPJ | Quick screening - largely replaced by duplex |
| Plethysmography | Modern (functional) | Global venous function | Quantifies severity; pre/post-op comparison |
| Venography | Modern (selected) | Complex/recurrent anatomy | Complex redo surgery; pelvic reflux mapping |
| CT/MR venography | Modern (selected) | Pelvic/iliac veins | Pelvic congestion; deep obstruction |
Key teaching point: The clinical tourniquet tests (Trendelenburg, Perthes) remain important for understanding the pathophysiology and for bedside assessment, but duplex ultrasound has superseded them as the definitive pre-treatment investigation. Competent clinicians who personally perform and interpret duplex scanning achieve the best surgical outcomes by designing bespoke treatment for each patient's unique anatomy. - Bailey and Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.