Biochemistry padha de English me simple language me MBBS ka
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have excellent material from Lippincott, Basic Medical Biochemistry, and Harper's. Let me compile this into a clear, student-friendly guide.
🔬 Carbohydrate Metabolism - MBBS Biochemistry (Simple English)
Sources: Lippincott Illustrated Biochemistry 8e, Basic Medical Biochemistry 6e, Harper's Biochemistry 32e
The Big Picture First
Think of carbohydrate metabolism as your body's energy factory. Glucose is the fuel. Your body breaks it down in steps to extract energy (ATP). The whole journey goes:
Glucose → Glycolysis → Pyruvate → Acetyl-CoA → TCA Cycle → Oxidative Phosphorylation → ATP (energy)
PART 1: How Does Glucose Get Into Cells?
Before anything can happen, glucose must enter the cell. There are two ways:
A. GLUT Transporters (Passive - no energy needed)
These are protein "doors" in the cell membrane. Glucose binds, the door opens, glucose slips in - no ATP needed (facilitated diffusion).
| Transporter | Where | Role |
|---|---|---|
| GLUT-1 | Most tissues | Baseline glucose uptake |
| GLUT-2 | Liver, kidneys, pancreas (β cells) | Senses high blood glucose |
| GLUT-4 | Muscle & fat | Activated by insulin |
| GLUT-5 | Small intestine, testes | Transports fructose |
Exam tip: GLUT-4 is the one insulin activates. In diabetes, GLUT-4 does not work well - muscle and fat cannot take up glucose properly.
B. SGLT (Sodium-Dependent - active, needs energy)
Used in gut and kidney tubules. Sodium drags glucose in against its concentration gradient. This needs Na⁺/K⁺ ATPase to maintain the sodium gradient. SGLT-2 inhibitors (gliflozins) are diabetic drugs that block this in the kidney, causing glucose to spill into urine.
PART 2: GLYCOLYSIS - "Breaking Glucose in Half"
Location: Cytoplasm (cytosol)
Occurs in: Every cell in the body
Simple equation:
1 Glucose (6C) → 2 Pyruvate (3C) + 2 ATP + 2 NADH
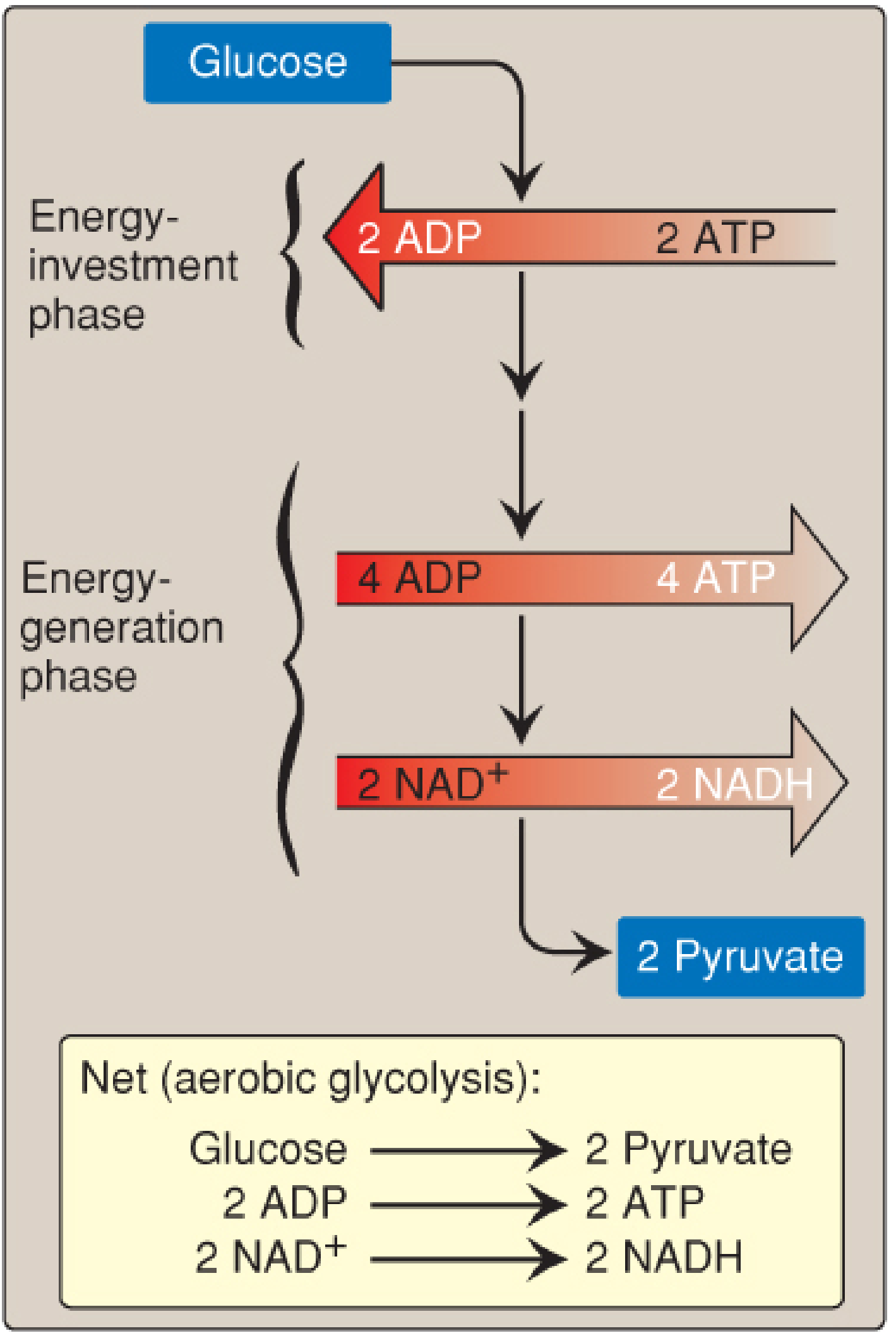
The Two Phases
Phase 1 - Energy Investment (Steps 1-5) - "Spend money to make money"
- You use 2 ATP to phosphorylate glucose
- This "primes the pump" - glucose is trapped in the cell and activated
Phase 2 - Energy Generation (Steps 6-10) - "Get returns"
- You make 4 ATP + 2 NADH
- Net gain = 4 - 2 = 2 ATP per glucose
The 10 Key Steps (Simplified)
| Step | Reaction | Enzyme | Notes |
|---|---|---|---|
| 1 | Glucose → Glucose-6-P | Hexokinase (or Glucokinase in liver) | Irreversible. Traps glucose in cell |
| 2 | Glucose-6-P → Fructose-6-P | Phosphoglucose isomerase | |
| 3 | Fructose-6-P → Fructose-1,6-bisP | Phosphofructokinase-1 (PFK-1) | MOST IMPORTANT regulatory step. Irreversible |
| 4 | Fructose-1,6-bisP → DHAP + GAP | Aldolase | Splits 6C into two 3C molecules |
| 5 | DHAP → GAP | Triose phosphate isomerase | |
| 6 | GAP → 1,3-bisphosphoglycerate | GAP dehydrogenase | Makes NADH |
| 7 | 1,3-bisP glycerate → 3-phosphoglycerate | Phosphoglycerate kinase | Substrate-level phosphorylation (makes ATP) |
| 8 | 3-PG → 2-PG | Phosphoglycerate mutase | |
| 9 | 2-PG → Phosphoenolpyruvate (PEP) | Enolase | Inhibited by fluoride (used in lab tubes!) |
| 10 | PEP → Pyruvate | Pyruvate kinase | Irreversible. Makes ATP |
The 3 Irreversible (Key) Enzymes - Remember "HoPK"
- Hexokinase / Glucokinase (step 1)
- PFK-1 (step 3) - the rate-limiting step
- Pyruvate Kinase (step 10)
These three are bypassed in gluconeogenesis (making new glucose).
What Controls PFK-1?
- Activated by: AMP, ADP (low energy state = speed up glycolysis), Fructose-2,6-bisphosphate (most potent activator, stimulated by insulin)
- Inhibited by: ATP, citrate (high energy state = slow down)
PART 3: WHAT HAPPENS TO PYRUVATE?
Pyruvate has two fates depending on oxygen availability:
[WITH O2]
Pyruvate ─────────────────────────→ Acetyl-CoA → TCA Cycle
(Pyruvate Dehydrogenase)
[WITHOUT O2]
Pyruvate ─────────────────────────→ Lactate
(Lactate Dehydrogenase)
PART 4: PYRUVATE DEHYDROGENASE COMPLEX (PDC)
Location: Mitochondrial matrix
Function: Links glycolysis to TCA cycle
Pyruvate (3C) → Acetyl-CoA (2C) + CO₂ + NADH
This is an irreversible reaction - you cannot go back from Acetyl-CoA to pyruvate (which is why you cannot convert fat into glucose!).
Cofactors needed (remember "Tender Loving Care For Nancy")
- TPP (Thiamine - Vitamin B1)
- Lipoate (Lipoic acid)
- CoA (Coenzyme A - Pantothenic acid, B5)
- FAD (Riboflavin, B2)
- NAD⁺ (Niacin, B3)
Clinical link: Thiamine (B1) deficiency → PDC cannot work → pyruvate builds up → lactic acidosis. This is why alcoholics get Wernicke's encephalopathy!
PDC Regulation
- Activated by: ADP, NAD⁺, CoA, Ca²⁺, insulin
- Inhibited by: Acetyl-CoA, NADH, ATP (products inhibit when energy is high)
PART 5: TCA CYCLE (Krebs Cycle / Citric Acid Cycle)
Location: Mitochondrial matrix
Occurs in: All cells with mitochondria (NOT RBCs)
The TCA cycle is a cycle - it starts and ends with the same molecule (oxaloacetate, OAA).
Simple concept: Acetyl-CoA (2C) enters + OAA (4C) → Citrate (6C). After one full turn, OAA is regenerated, 2 CO₂ are released, and energy carriers are made.
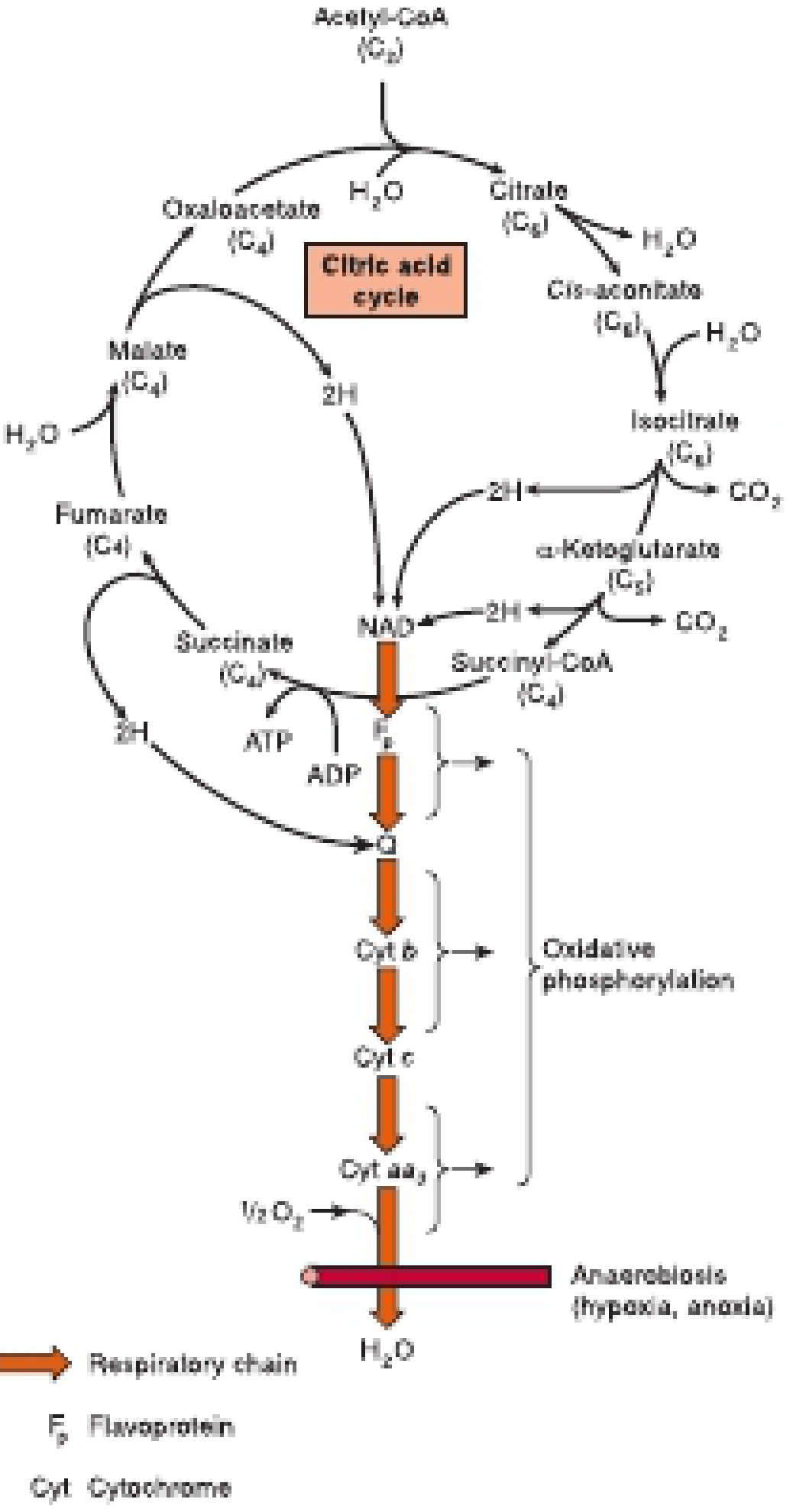
The 8 Steps of TCA
| Step | Substrate → Product | Enzyme | What's Made |
|---|---|---|---|
| 1 | OAA + Acetyl-CoA → Citrate | Citrate synthase | (condensation) |
| 2 | Citrate → Isocitrate | Aconitase | |
| 3 | Isocitrate → α-ketoglutarate | Isocitrate dehydrogenase | NADH + CO₂ |
| 4 | α-KG → Succinyl-CoA | α-KG dehydrogenase | NADH + CO₂ |
| 5 | Succinyl-CoA → Succinate | Succinyl-CoA synthetase | GTP (= ATP) |
| 6 | Succinate → Fumarate | Succinate dehydrogenase | FADH₂ |
| 7 | Fumarate → Malate | Fumarase | |
| 8 | Malate → OAA | Malate dehydrogenase | NADH |
Per Turn of TCA Cycle, you get:
- 3 NADH + 1 FADH₂ + 1 GTP + 2 CO₂
Regulation of TCA Cycle
- Citrate synthase - inhibited by citrate, ATP, NADH
- Isocitrate dehydrogenase - inhibited by NADH, ATP; activated by ADP
- α-KG dehydrogenase - inhibited by succinyl-CoA, NADH
PART 6: TOTAL ATP YIELD FROM 1 GLUCOSE
| Step | ATP Produced |
|---|---|
| Glycolysis (substrate level) | 2 ATP |
| Glycolysis - 2 NADH (via ETC) | ~5 ATP (2.5 each) |
| PDC - 2 NADH | ~5 ATP |
| TCA x 2 turns - 6 NADH | ~15 ATP |
| TCA x 2 turns - 2 FADH₂ | ~3 ATP |
| TCA x 2 turns - 2 GTP | 2 ATP |
| TOTAL | ~30-32 ATP |
Old textbooks said 36-38 ATP but modern counts give 30-32 due to mitochondrial transport costs.
PART 7: ANAEROBIC GLYCOLYSIS - When No Oxygen is Available
Without oxygen, NADH cannot be reoxidized in the ETC. But glycolysis needs NAD⁺ to continue (step 6). So the cell recycles NADH → NAD⁺ by converting pyruvate to lactate.
Pyruvate + NADH → Lactate + NAD⁺ (enzyme: Lactate Dehydrogenase)
Net yield: Only 2 ATP per glucose (much less efficient!)
Where this matters:
- RBCs - no mitochondria, always use anaerobic glycolysis
- Exercising muscle - when O₂ supply cannot keep up with demand
- Cancer cells - prefer anaerobic glycolysis even with O₂ present (Warburg effect)
- Eye lens, cornea - no blood supply
Clinical: Lactic Acidosis - excess lactate accumulates when tissues are hypoxic (shock, sepsis) or when PDC/mitochondria are dysfunctional.
PART 8: GLYCOGEN METABOLISM (Quick Overview)
Glycogen = storage form of glucose, like a "glucose battery"
- Stored mainly in liver (for blood glucose maintenance) and muscle (for local use)
| Process | What | Where | Key Enzyme |
|---|---|---|---|
| Glycogenesis | Glucose → Glycogen | Liver & Muscle | Glycogen synthase |
| Glycogenolysis | Glycogen → Glucose | Liver & Muscle | Glycogen phosphorylase |
Hormonal control:
- Insulin - promotes glycogenesis (after meals)
- Glucagon/Epinephrine - promotes glycogenolysis (fasting/stress)
Glycogen Storage Diseases (GSDs): Inherited enzyme defects. Most important:
- Von Gierke (Type I): Glucose-6-phosphatase deficiency → severe hypoglycemia, liver enlargement
- McArdle (Type V): Muscle phosphorylase deficiency → muscle cramps on exercise
- Pompe (Type II): Lysosomal acid maltase (GAA) deficiency → cardiomegaly in infants
PART 9: GLUCONEOGENESIS - "Making New Glucose"
When blood glucose is low (fasting), the liver (and kidney) can make glucose from non-carbohydrate precursors.
Precursors (the 4 main ones):
- Lactate (from RBCs, exercising muscle)
- Glycerol (from fat breakdown)
- Alanine (from muscle protein)
- Oxaloacetate (from most amino acids)
Key concept: Gluconeogenesis is mostly the REVERSE of glycolysis, EXCEPT at the 3 irreversible steps which need special bypass enzymes:
| Glycolysis (irreversible) | Gluconeogenesis bypass |
|---|---|
| Pyruvate kinase (PEP → Pyruvate) | Pyruvate carboxylase + PEPCK |
| PFK-1 (F-6-P → F-1,6-bisP) | Fructose-1,6-bisphosphatase |
| Hexokinase (Glucose → G-6-P) | Glucose-6-phosphatase |
Main site: Liver (and kidney during prolonged fasting)
Glucose-6-phosphatase is only in liver and kidney - muscle cannot release free glucose into blood!
PART 10: PENTOSE PHOSPHATE PATHWAY (HMP Shunt)
An alternative fate of Glucose-6-P (not just glycolysis)
Purpose:
- Makes NADPH (needed for fatty acid synthesis, steroid synthesis, and to protect RBCs from oxidative damage via glutathione)
- Makes Ribose-5-phosphate (needed for nucleotide/DNA/RNA synthesis)
High activity in: Liver, adrenal cortex (steroid synthesis), RBCs (antioxidant defense), lactating breast (fatty acid synthesis)
Clinical: G6PD deficiency - most common enzyme deficiency worldwide. RBCs cannot make NADPH → cannot protect against oxidative stress → hemolytic anemia triggered by drugs (primaquine, dapsone), infections, or fava beans.
Summary Flowchart
GLUCOSE
│
↓ [Glycolysis - Cytoplasm]
PYRUVATE + 2 ATP + 2 NADH
│
├──[No O2]──→ LACTATE (only 2 ATP total)
│
↓ [Pyruvate Dehydrogenase - Mitochondria]
ACETYL-CoA + CO2 + NADH
│
↓ [TCA Cycle - Mitochondria]
3 NADH + 1 FADH2 + 1 GTP + 2 CO2 per turn
│
↓ [Oxidative Phosphorylation - ETC]
~30-32 ATP TOTAL
High-Yield Exam Points
| Topic | Fact to Remember |
|---|---|
| Rate-limiting step of glycolysis | PFK-1 (step 3) |
| Activated by insulin | PFK-1, Pyruvate kinase, PDC, Glycogen synthase |
| Cannot do gluconeogenesis | Muscle (no glucose-6-phosphatase) |
| Irreversible in PDC | Pyruvate → Acetyl-CoA (fat cannot become glucose) |
| TCA per turn | 3 NADH, 1 FADH₂, 1 GTP, 2 CO₂ |
| Enzyme inhibited by fluoride (lab tubes) | Enolase (step 9 of glycolysis) - prevents glycolysis in blood glucose samples |
| Warburg effect | Cancer cells use anaerobic glycolysis even in O₂ |
| Vitamin B1 deficiency | PDC fails → lactic acidosis, Wernicke's |
| G6PD deficiency | Hemolytic anemia with oxidative stress |
| Von Gierke's disease | G6Pase deficiency, fasting hypoglycemia |
Sources:
- Lippincott Illustrated Reviews: Biochemistry, 8e, pp. 294-298
- Basic Medical Biochemistry: A Clinical Approach, 6e, pp. 791-793, 844
- Harper's Illustrated Biochemistry, 32e, pp. 168-170
Koi bhi step detail me samajhna ho - glycolysis ke steps, TCA cycle, ya koi clinical disease - batao, aur detail karke explain kar deta hoon!
Sab details me samjhao
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Yeh lo - Carbohydrate Metabolism ke Complete Detailed MBBS Notes - sab kuch cover kar diya! 🎯
Quick Summary - Kya Kya Cover Kiya:
| # | Topic | Details |
|---|---|---|
| 1 | Glucose Transport | GLUT 1-5 differences, SGLT mechanism, clinical drugs |
| 2 | Glycolysis | All 10 steps, each enzyme, regulation, clinical (arsenic, fluoride, PK deficiency, MODY) |
| 3 | Pyruvate Fate | Aerobic vs anaerobic, 3 possible fates |
| 4 | PDC | Structure (E1/E2/E3), cofactors (B1,B2,B3,B5,Lipoate), regulation, PDC deficiency, Wernicke's |
| 5 | TCA Cycle | All 8 steps, each enzyme, NADH/FADH2/GTP yield, anaplerosis |
| 6 | ETC & Oxidative Phosphorylation | All 4 complexes, chemiosmotic theory, inhibitors (cyanide, CO, rotenone), uncouplers |
| 7 | Total ATP | 30-32 ATP, why not 38 |
| 8 | Gluconeogenesis | 4 precursors, 3 bypass enzymes (Pyruvate Carboxylase, PEPCK, FBPase, G6Pase), regulation |
| 9 | Glycogen Metabolism | Synthesis, degradation, all 6 GSDs with features and treatment |
| 10 | Pentose Phosphate | NADPH, Ribose-5P, G6PD deficiency, Heinz bodies, favism, two variants |
| 11 | Cori & Alanine cycles | Complete pathways |
| 12 | Clinical Summary | All diseases + hormonal regulation table |
Koi bhi concept aur acha samajhna ho - mechanisms, diagrams, ya MCQ practice - batao! 📚
HMP Shunt
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Ab mere paas sab images aur complete textbook content hai. Poora detailed HMP Shunt guide likhta hoon!
🔬 HMP SHUNT (Hexose Monophosphate Pathway / Pentose Phosphate Pathway)
Complete MBBS Notes - Simple English
Sources: Basic Medical Biochemistry 6e | Harper's Biochemistry 32e | Lippincott 8e
INTRODUCTION - "Yeh Pathway Kya Hai?"
HMP Shunt ek alternative glucose pathway hai. Glycolysis se alag, yeh pathway:
- ATP nahi banata
- NADPH banata hai (reducing power - antioxidant + biosynthesis)
- Ribose-5-Phosphate banata hai (DNA/RNA ke liye nucleotides)
Bypass kyun? Yeh Glucose-6-Phosphate (G6P) par shunt (detour) leta hai - isliye naam "HMP Shunt"
KEY FACTS AT A GLANCE
| Feature | HMP Shunt | Glycolysis |
|---|---|---|
| Location | Cytosol | Cytosol |
| ATP produced | ❌ ZERO | ✅ 2 ATP |
| NADPH produced | ✅ YES | ❌ No |
| NADH produced | ❌ No | ✅ YES |
| CO2 produced | ✅ YES | ❌ No |
| Coenzyme used | NADP+ | NAD+ |
| Starting material | Glucose-6-P | Glucose-6-P |
WHERE DOES IT OCCUR? (Tissue Distribution)
| Tissue | Why active? |
|---|---|
| Liver | Major site - fatty acid synthesis needs NADPH; enzyme induced by insulin |
| Adrenal cortex | Steroid (cortisol/aldosterone) synthesis needs NADPH |
| RBCs | Antioxidant defense - ONLY source of NADPH here |
| Lactating breast | Fatty acid synthesis for milk lipids |
| Testes/ovaries | Steroid hormone synthesis |
| Phagocytes (neutrophils) | NADPH oxidase uses NADPH to kill bacteria (respiratory burst) |
| Lens of eye | Protection from oxidative damage |
| Rapidly dividing cells | Need Ribose-5-P for nucleotide synthesis |
Low activity in: Muscle (mainly does glycolysis)
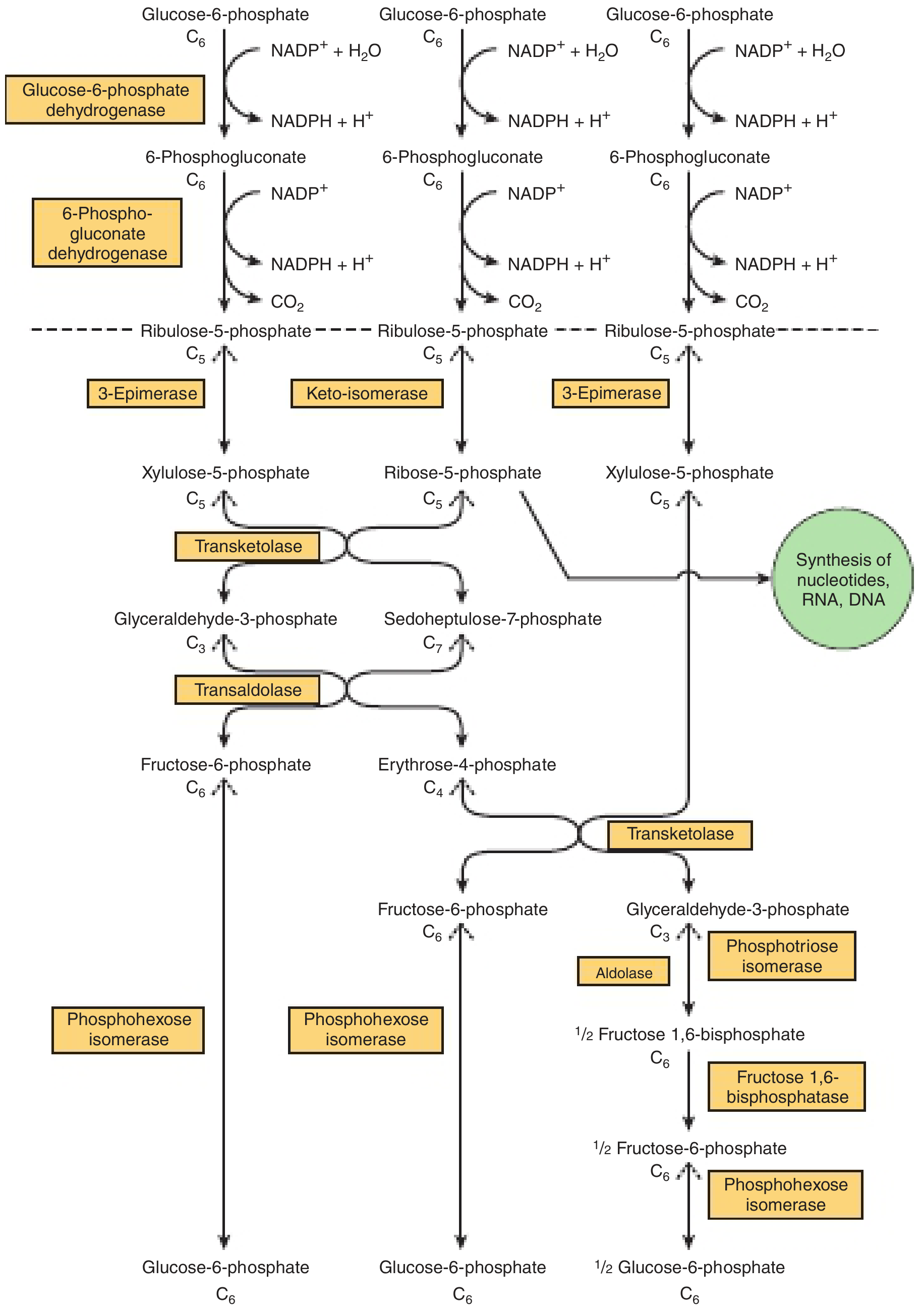
THE TWO PHASES
Phase 1 (Oxidative) = IRREVERSIBLE → makes NADPH
Phase 2 (Non-Oxidative) = REVERSIBLE → shuffles carbon skeletons
PHASE 1: OXIDATIVE PHASE - "NADPH Factory"
3 reactions, 2 NADPH produced per glucose-6-P
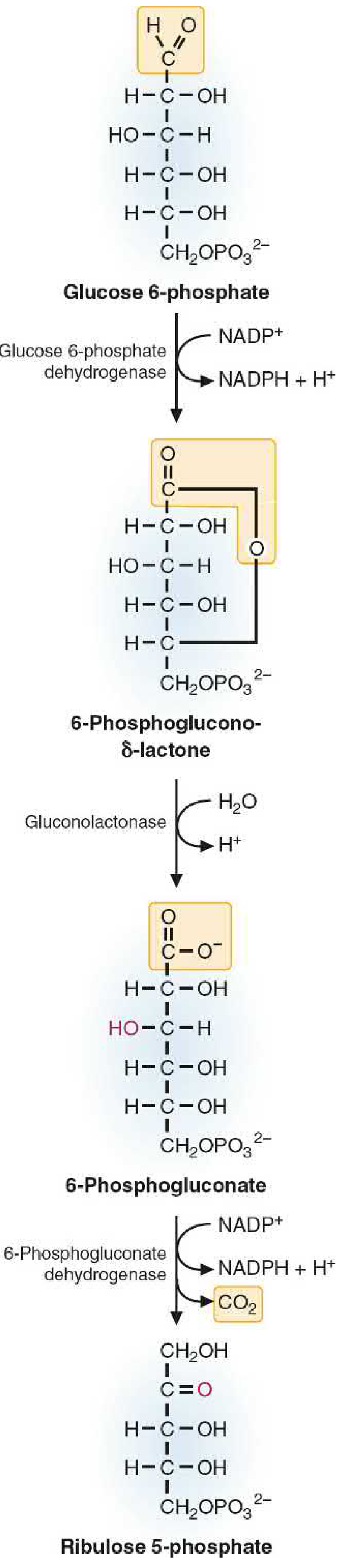
Step 1: Glucose-6-P → 6-Phosphoglucono-δ-lactone
Enzyme: Glucose-6-Phosphate Dehydrogenase (G6PD)
- Uses: NADP+ → makes NADPH
- This is the committed step (rate-limiting)
- Carbon 1 (aldehyde group) is oxidized
- Inhibited by NADPH (product inhibition - if NADPH is enough, pathway slows)
- This is the enzyme deficient in G6PD deficiency!
Step 2: 6-Phosphoglucono-δ-lactone → 6-Phosphogluconate
Enzyme: Gluconolactonase (Gluconolactone Hydrolase)
- Simple hydrolysis - adds water
- Opens the ring structure
- No coenzyme needed
Step 3: 6-Phosphogluconate → Ribulose-5-Phosphate + CO2
Enzyme: 6-Phosphogluconate Dehydrogenase
- Uses: NADP+ → makes NADPH
- An oxidative decarboxylation (loses one CO2)
- Similar mechanism to isocitrate dehydrogenase in TCA cycle
- Product: Ribulose-5-P (5-carbon ketose sugar)
Phase 1 Net Result (per molecule):
1 Glucose-6-P + 2 NADP+ → 1 Ribulose-5-P + 2 NADPH + CO2
PHASE 2: NON-OXIDATIVE PHASE - "Carbon Shuffler"
After phase 1, the cell has Ribulose-5-P. Now what? Depends on what the cell needs!
First - Ribulose-5-P is converted to two products:
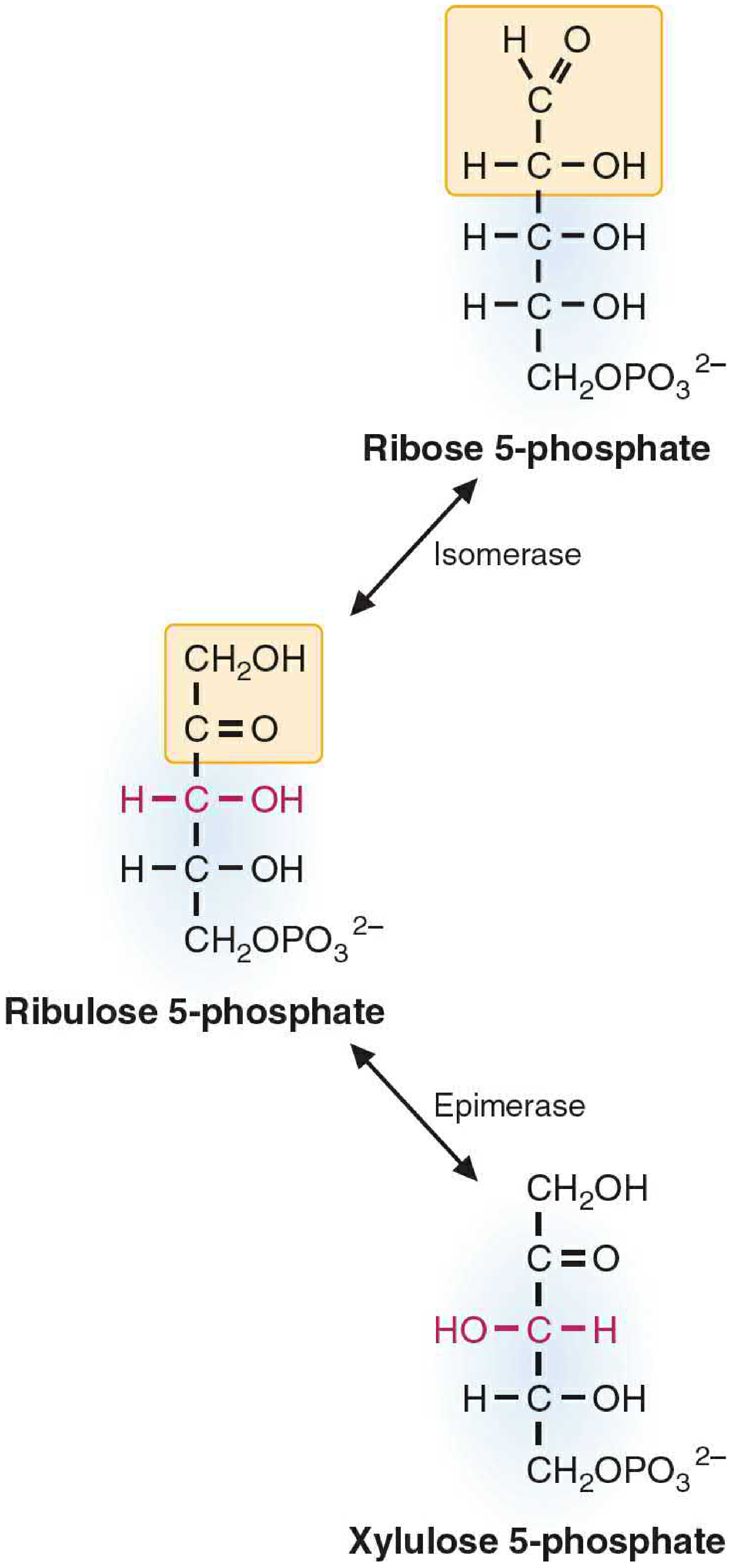
- Ribulose-5-P → Ribose-5-P (by Isomerase - aldose/ketose conversion) → Used for nucleotide synthesis (DNA, RNA, ATP, NAD+, FAD, CoA)
- Ribulose-5-P → Xylulose-5-P (by Epimerase - changes stereochemistry at C3) → Used in carbon-shuffling reactions below
The Two Key Enzymes of Non-Oxidative Phase:
Transketolase (Cofactor: Thiamine - Vitamin B1)
- Transfers a 2-carbon unit from a ketose to an aldose
- Reaction: ketose (shorter by 2C) + aldose (longer by 2C)
- Requires TPP (Thiamine Pyrophosphate, Vitamin B1) as cofactor!
- Clinical: B1 deficiency → transketolase fails → HMP shunt cannot recycle carbons → measured as RBC transketolase activity test (gold standard for B1 deficiency)
Transaldolase (No cofactor needed)
- Transfers a 3-carbon unit from a ketose to an aldose
- Proceeds via Schiff base intermediate (3C unit attached to lysine in enzyme)
The Non-Oxidative Reactions:
Starting with: 2 Xylulose-5-P + 1 Ribose-5-P (from 3 Ribulose-5-P)
Step A (Transketolase):
Xylulose-5-P (C5) + Ribose-5-P (C5) → Sedoheptulose-7-P (C7) + Glyceraldehyde-3-P (C3)
Step B (Transaldolase):
Sedoheptulose-7-P (C7) + Glyceraldehyde-3-P (C3) → Fructose-6-P (C6) + Erythrose-4-P (C4)
Step C (Transketolase):
Xylulose-5-P (C5) + Erythrose-4-P (C4) → Fructose-6-P (C6) + Glyceraldehyde-3-P (C3)
End products: Fructose-6-P and Glyceraldehyde-3-P (both are glycolytic intermediates!)
These can re-enter glycolysis - so the carbon is NOT wasted.
OVERALL EQUATION
If the goal is to maximize NADPH (cycle keeps running):
Glucose-6-P + 12 NADP+ + 6 H₂O → 6 CO₂ + 12 NADPH + Phosphate
For 3 glucose-6-P going through once:
- Input: 3 Glucose-6-P
- Output: 6 NADPH + 3 CO2 + products that regenerate 2 Glucose-6-P (and 1 GAP → can become ½ Glucose-6-P)
THE CELL'S CHOICES - "What Does the Cell Need?"
This pathway is FLEXIBLE. Depending on what the cell needs, it adjusts:
| Cell Needs | What Happens |
|---|---|
| Only NADPH | Oxidative reactions produce NADPH; non-oxidative reactions convert Ribulose-5-P BACK to Glucose-6-P → cycle repeats → maximize NADPH |
| NADPH + Ribose-5-P | Oxidative phase runs → NADPH made + Ribulose-5-P → isomerase converts to Ribose-5-P. Both products used directly |
| Only Ribose-5-P (e.g., dividing cell) | High NADPH inhibits G6PD → oxidative phase OFF; non-oxidative phase runs in reverse: Fructose-6-P + GAP → Ribose-5-P via transketolase/transaldolase |
| NADPH + Pyruvate | Both phases run; Ribulose-5-P → Fructose-6-P/GAP → enter glycolysis → pyruvate |
WHY IS NADPH SO IMPORTANT?
In RBCs - The Most Tested!
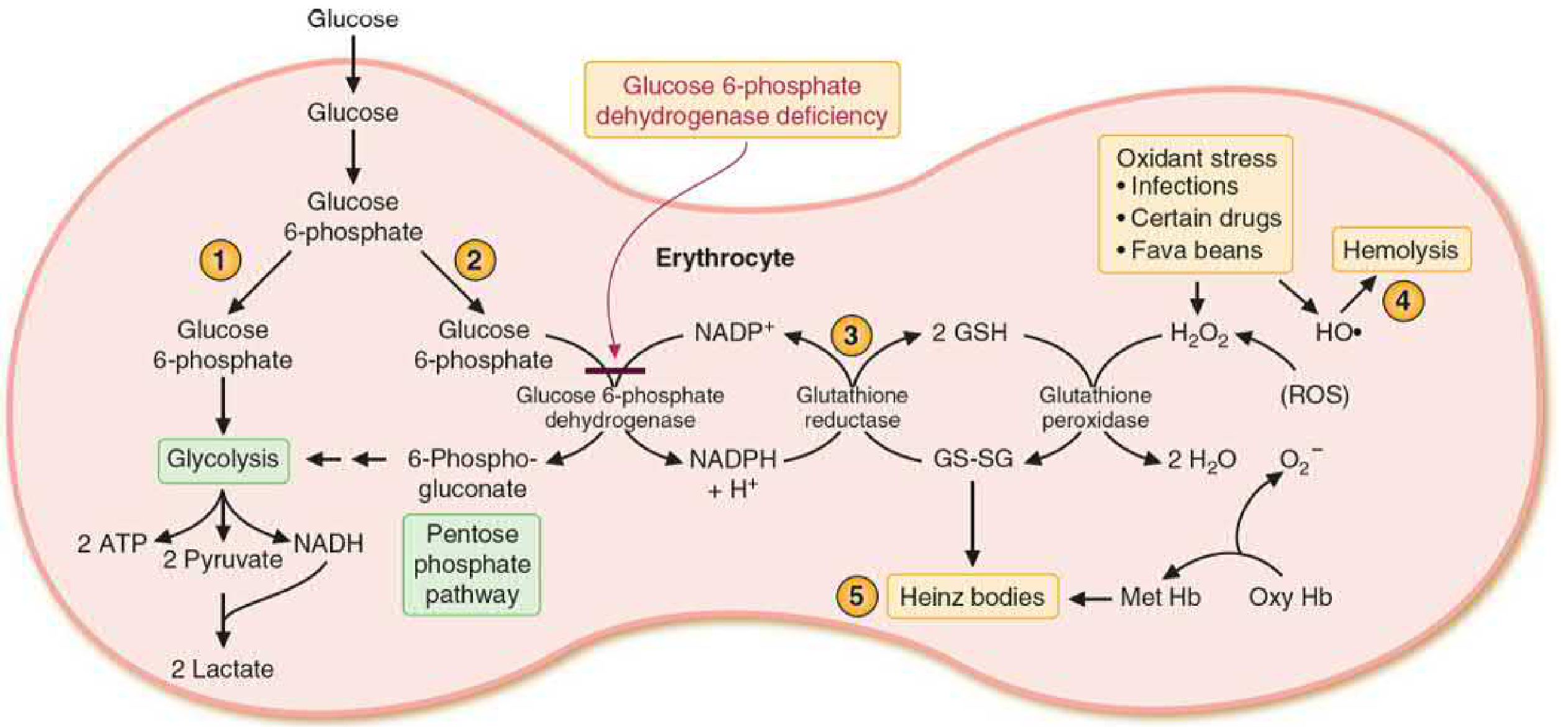
Step-by-step protection mechanism in RBCs:
HMP Shunt → makes NADPH
↓
NADPH + Glutathione Reductase → converts GSSG (oxidized) → GSH (reduced)
↓
GSH + Glutathione Peroxidase → destroys H₂O₂ and lipid peroxides
↓
Result: RBC membrane protected, Hb not oxidized
If HMP Shunt fails (G6PD deficiency):
No NADPH → cannot regenerate GSH → H₂O₂ accumulates
↓
H₂O₂ oxidizes Hb → methemoglobin → denatured Hb = Heinz bodies
↓
Heinz bodies attach to RBC membrane → membrane damage → HEMOLYSIS
Complete List of NADPH Roles:
| Role | Where |
|---|---|
| Reduce glutathione (GSH) | ALL cells, especially RBCs |
| Fatty acid synthesis | Liver, adipose, lactating breast |
| Cholesterol synthesis | Liver, steroidogenic cells |
| Steroid synthesis | Adrenal cortex, gonads |
| Cytochrome P450 reactions | Liver (drug metabolism) |
| NADPH Oxidase - kills bacteria | Neutrophils, macrophages |
| Nitric oxide synthesis (eNOS) | Endothelial cells |
| Deoxynucleotide synthesis | All dividing cells |
| Fatty acid chain elongation | ER membrane |
G6PD DEFICIENCY - Complete Coverage
Basic Facts:
- Most common enzyme deficiency in the world (~400 million people)
- Gene is on X chromosome → X-linked recessive → mainly males affected
- Females are carriers (one normal X protects them usually)
- Malaria belt distribution - heterozygous females have partial malaria protection (infected RBCs are more fragile and lyse faster)
Mechanism:
No G6PD → No NADPH → No reduced glutathione (GSH)
→ Cannot remove H₂O₂ when oxidative stress occurs
→ H₂O₂ oxidizes hemoglobin → Heinz bodies
→ RBC membrane damaged → HEMOLYSIS
Triggers of Hemolytic Crisis:
| Category | Examples |
|---|---|
| Antimalarial drugs | Primaquine, Chloroquine (high dose) |
| Antibiotics | Dapsone, Sulfonamides, Nitrofurantoin, Trimethoprim |
| Other drugs | Rasburicase, Methylene blue |
| Food | Fava beans (Favism) - contains vicine + convicine → generate H₂O₂ |
| Infection | Viral/bacterial infections - immune response → oxidative stress |
| Chemicals | Naphthalene (mothballs), henna |
Two Main Variants:
| Feature | African (A-) | Mediterranean |
|---|---|---|
| Population | Sub-Saharan Africa | Mediterranean, Middle East, India |
| Enzyme | Unstable, degrades in old RBCs | Stable but LOW activity in all RBCs |
| Severity | Mild-moderate, SELF-LIMITING | Severe, can be fatal |
| Why self-limiting? | Young RBCs (reticulocytes) still have enough G6PD → as old cells lyse, new ones replace them | All cells affected - no "safe" RBCs |
Lab Findings During Crisis:
- Decreased Hb (hemolytic anemia)
- Increased bilirubin (indirect - from Hb breakdown)
- Increased reticulocytes (bone marrow response)
- Heinz bodies on peripheral smear with methyl violet/crystal violet stain
- Normal G6PD activity may be falsely normal DURING the crisis (old cells with low G6PD have already lysed; only young cells with higher activity remain!)
- Test after crisis for reliable G6PD measurement
Treatment:
- Stop the triggering drug/exposure
- Avoid fava beans
- Supportive: fluids, folic acid (for reticulocytosis)
- Severe: blood transfusion
- NO specific enzyme replacement currently
REGULATION OF HMP SHUNT
Main regulatory enzyme = G6PD (Step 1)
Inhibited by:
- NADPH (product inhibition - the most important regulator)
- If NADPH/NADP+ ratio is HIGH → pathway slows down automatically
Activated by (Gene induction):
- Insulin (post-meal, when glucose is high and cell is in "build mode")
- Induces G6PD synthesis in liver → more flux through HMP shunt
- This couples glucose availability to NADPH production for biosynthesis
Connected to Glycolysis:
- Xylulose-5-P (a product of HMP shunt) activates a phosphatase that increases Fructose-2,6-bisphosphate → activates PFK-1 → speeds up glycolysis
- So when HMP shunt is active, glycolysis also gets boosted!
THIAMINE (B1) DEFICIENCY AND HMP SHUNT
Transketolase needs Thiamine Pyrophosphate (TPP) as cofactor.
Clinical test: Erythrocyte transketolase activity test
- Measure RBC transketolase activity WITH and WITHOUT added TPP
- If B1 deficient: baseline activity is LOW, adding TPP gives a BIG BOOST (>15-20% stimulation = deficient)
- If B1 sufficient: adding TPP has little effect (enzyme already saturated)
This is why the test is used to diagnose Beriberi / Wernicke's early - even before clinical symptoms appear.
CHRONIC GRANULOMATOUS DISEASE (CGD) - Related Condition
Deficiency: NADPH Oxidase (in neutrophils/macrophages)
Result: Cannot make superoxide (O2•⁻) → cannot kill phagocytosed bacteria
Normal mechanism:
NADPH + O₂ → NADPH Oxidase → O₂•⁻ (superoxide) → H₂O₂ → HOCl → kills bacteria
CGD: Neutrophils can engulf bacteria but cannot kill them → recurrent, severe bacterial/fungal infections (especially catalase-positive organisms like Staph aureus, Aspergillus)
Diagnosis: Nitroblue tetrazolium (NBT) test - normal cells turn blue (superoxide made); CGD cells remain colorless
Treatment: Prophylactic antibiotics (TMP-SMX), antifungals (Itraconazole), IFN-γ, bone marrow transplant (curative)
HMP SHUNT vs GLYCOLYSIS - COMPARISON TABLE
| Feature | HMP Shunt | Glycolysis |
|---|---|---|
| Location | Cytosol | Cytosol |
| Starts with | Glucose-6-P | Glucose |
| ATP consumed | 0 | 2 |
| ATP produced | 0 | 4 (net 2) |
| NADPH produced | 2 per G6P | 0 |
| NADH produced | 0 | 2 |
| CO2 produced | 1 per G6P | 0 |
| Coenzyme | NADP+ | NAD+ |
| Products | Ribulose-5-P, NADPH | Pyruvate, ATP, NADH |
| Reversible phase? | Phase 2 is reversible | Most steps reversible except 3 |
| Key enzyme | G6PD | PFK-1 |
| Purpose | Biosynthesis + antioxidant | Energy production |
| Oxygen needed? | No | No (anaerobic glycolysis) |
IMPORTANT INTERMEDIATES - REMEMBER THESE
| Compound | Carbons | Made by | Goes to |
|---|---|---|---|
| Ribulose-5-P | 5C | Phase 1 (oxidative) | Ribose-5-P OR Xylulose-5-P |
| Ribose-5-P | 5C | Isomerase | Nucleotide synthesis (DNA, RNA) |
| Xylulose-5-P | 5C | Epimerase | Transketolase reactions |
| Sedoheptulose-7-P | 7C | Transketolase (step A) | Transaldolase reaction |
| Erythrose-4-P | 4C | Transaldolase (step B) | Transketolase (step C) + Aromatic amino acid synthesis |
| Fructose-6-P | 6C | Non-oxidative phase output | Re-enters glycolysis |
| Glyceraldehyde-3-P | 3C | Non-oxidative phase output | Re-enters glycolysis |
Special note on Erythrose-4-P: Also used for synthesis of aromatic amino acids (phenylalanine, tyrosine, tryptophan) in bacteria (shikimate pathway) - this is the target of the herbicide glyphosate and the antibiotic chloramphenicol's basis of selectivity
HIGH-YIELD EXAM POINTS - MUST KNOW!
| Point | Fact |
|---|---|
| Rate-limiting enzyme | G6PD (Glucose-6-Phosphate Dehydrogenase) |
| Inhibited by | NADPH (product inhibition) |
| Induced by | Insulin (in liver) |
| Cofactor for Transketolase | Thiamine (Vitamin B1) |
| Only NADPH source in RBCs | HMP Shunt (RBCs have no mitochondria) |
| Most common enzyme deficiency worldwide | G6PD deficiency |
| G6PD deficiency inheritance | X-linked recessive |
| Heinz body stain | Crystal violet / Methyl violet |
| Favism caused by | Fava beans (broad beans) |
| Test for B1 deficiency using HMP | Erythrocyte transketolase activity |
| CGD - deficiency | NADPH Oxidase |
| CGD - test | Nitroblue tetrazolium (NBT) test |
| Phase 1 = | Irreversible |
| Phase 2 = | Reversible |
| G6PD + 6-PGD use | NADP+ (not NAD+) |
| ATP produced = | ZERO |
CLINICAL SCENARIO - QUICK MCQ APPROACH
Q: Patient develops hemolytic anemia after taking primaquine for malaria. Peripheral smear shows Heinz bodies. Diagnosis?
→ G6PD deficiency - oxidant drug → RBCs lack NADPH → cannot regenerate GSH → H2O2 destroys Hb → Heinz bodies → hemolysis
Q: Child with recurrent bacterial (Staph, Aspergillus) infections. NBT test negative. Diagnosis?
→ Chronic Granulomatous Disease (CGD) - NADPH oxidase deficiency
Q: B1 deficiency patient - which HMP shunt enzyme activity will be LOW?
→ Transketolase (needs TPP = thiamine pyrophosphate)
Q: Which tissues have HIGH G6PD activity?
→ Liver, adrenal cortex, lactating breast, RBCs, phagocytes, gonads
Q: G6PD is inhibited by what?
→ NADPH (when cell has enough, shunt slows down)
Q: Rapidly dividing tumor cell needs ribose-5-P but NADPH is already high. Which direction does HMP shunt go?
→ Only non-oxidative phase (reverse direction): Fructose-6-P + GAP → Ribose-5-P (G6PD is inhibited by high NADPH, so oxidative phase is OFF)
Sources: Basic Medical Biochemistry: A Clinical Approach 6e (pp. 962-971), Harper's Illustrated Biochemistry 32e (pp. 203-210)
Sab kuch cover ho gaya - reactions, enzymes, regulation, G6PD deficiency, CGD, aur exam MCQ points! 🎯
Koi aur topic chahiye - jaise Lipid Metabolism, Protein Metabolism, ya Enzymes & Vitamins? Batao!
English me bta sab dubara
Here is everything about the HMP Shunt explained fully in simple English, using the same textbook content.
🔬 HMP SHUNT (Hexose Monophosphate Pathway / Pentose Phosphate Pathway)
Complete MBBS Notes — Pure English, Simple Language
Sources: Basic Medical Biochemistry 6e | Harper's Biochemistry 32e | Lippincott 8e
WHAT IS THE HMP SHUNT?
The HMP Shunt is an alternative pathway for glucose metabolism. Instead of breaking glucose down for energy (like glycolysis does), this pathway uses glucose to produce two very important things:
- NADPH — a molecule that provides reducing power for antioxidant defense and biosynthesis
- Ribose-5-Phosphate — a 5-carbon sugar needed to make DNA, RNA, and nucleotides
Think of it this way: Glycolysis is the "energy factory." HMP Shunt is the "supply factory" — it makes raw materials the cell needs to build things and protect itself.
No ATP is produced in this pathway. That is its defining feature.
KEY COMPARISON WITH GLYCOLYSIS
| Feature | HMP Shunt | Glycolysis |
|---|---|---|
| Location | Cytosol | Cytosol |
| ATP produced | ZERO | 2 (net) |
| NADPH produced | YES — 2 per glucose | None |
| NADH produced | None | 2 per glucose |
| CO2 released | YES — 1 per glucose | None |
| Coenzyme used | NADP+ | NAD+ |
| Main purpose | Biosynthesis + antioxidant protection | Energy production |
| Starting material | Glucose-6-Phosphate | Glucose |
Both pathways start from Glucose-6-Phosphate (G6P) — that is the branching point.
WHERE DOES IT OCCUR? (Tissue Distribution)
| Tissue | Reason |
|---|---|
| Liver | Major site — makes NADPH for fatty acid and cholesterol synthesis; G6PD enzyme is induced by insulin here |
| Adrenal cortex | Needs huge amounts of NADPH to synthesize steroid hormones (cortisol, aldosterone) |
| Red Blood Cells (RBCs) | HMP shunt is the ONLY source of NADPH in RBCs — used to protect the cell from oxidative damage |
| Lactating breast | NADPH needed for fatty acid synthesis to make milk fat |
| Testes and ovaries | Steroid hormone (testosterone, estrogen) synthesis |
| Neutrophils and macrophages | NADPH is used by NADPH oxidase to generate superoxide and kill bacteria |
| Rapidly dividing cells | Need large amounts of ribose-5-phosphate for DNA/RNA synthesis |
| Lens of the eye | Protection from oxidative damage (no blood supply, so very vulnerable) |
Low activity in muscle — muscle mainly uses glycolysis for energy, does not need much NADPH.
THE TWO PHASES
The HMP Shunt has two distinct phases:
- Phase 1 — Oxidative Phase → Irreversible → Produces NADPH
- Phase 2 — Non-Oxidative Phase → Reversible → Rearranges carbon skeletons
PHASE 1: OXIDATIVE PHASE
"The NADPH Factory"
3 reactions. Produces 2 NADPH and 1 CO2 per Glucose-6-P.
Reaction 1: Glucose-6-P → 6-Phosphoglucono-δ-Lactone
Enzyme: Glucose-6-Phosphate Dehydrogenase (G6PD)
- NADP+ accepts electrons → becomes NADPH
- Carbon-1 of glucose-6-P (the aldehyde carbon) is oxidized
- This is the rate-limiting, committed step of the entire pathway
- The reaction is irreversible
- Strongly inhibited by NADPH — when the cell already has enough NADPH, the pathway slows down automatically (product inhibition)
- This is the enzyme that is deficient in G6PD deficiency disease
Reaction 2: 6-Phosphoglucono-δ-Lactone → 6-Phosphogluconate
Enzyme: Gluconolactonase (Gluconolactone Hydrolase)
- A simple hydration reaction — water is added, the ring structure opens
- No coenzyme is needed
- No energy is produced or consumed
Reaction 3: 6-Phosphogluconate → Ribulose-5-Phosphate + CO2
Enzyme: 6-Phosphogluconate Dehydrogenase (6-PGD)
- This is an oxidative decarboxylation — oxidation happens AND one carbon is lost as CO2
- NADP+ accepts electrons → becomes NADPH (second NADPH of this phase)
- The product is Ribulose-5-Phosphate, a 5-carbon ketose sugar
- The mechanism is similar to isocitrate dehydrogenase in the TCA cycle
Phase 1 Summary:
1 Glucose-6-P + 2 NADP+ → 1 Ribulose-5-P + 2 NADPH + 1 CO2
PHASE 2: NON-OXIDATIVE PHASE
"The Carbon Shuffler"
After phase 1, the cell has Ribulose-5-Phosphate. What happens next depends entirely on what the cell needs at that moment.
Step 1 of phase 2 — Ribulose-5-P is converted into two different 5-carbon sugars:
-
Ribulose-5-P → Ribose-5-P (enzyme: Isomerase — converts ketose to aldose form) → Ribose-5-P goes directly into nucleotide synthesis (for DNA, RNA, ATP, NAD+, FAD, CoA)
-
Ribulose-5-P → Xylulose-5-P (enzyme: Epimerase — flips the OH group at carbon-3) → Xylulose-5-P enters the carbon-shuffling reactions below
The Two Key Enzymes of Phase 2:
1. Transketolase
- Transfers a 2-carbon unit from a ketose sugar to an aldose sugar
- Cofactor required: Thiamine Pyrophosphate (TPP) — Vitamin B1
- Without B1, this enzyme does not work → HMP shunt cannot complete Phase 2
- Clinical test: RBC transketolase activity is used to diagnose Vitamin B1 deficiency — if B1 is low, adding TPP in the test tube will strongly boost the enzyme activity
2. Transaldolase
- Transfers a 3-carbon unit from a ketose sugar to an aldose sugar
- No cofactor is required
- The 3-carbon unit forms a Schiff base with a lysine residue inside the enzyme
The 3 Non-Oxidative Reactions:
Starting material: 2 Xylulose-5-P + 1 Ribose-5-P
Reaction A — Transketolase:
Xylulose-5-P (5C) + Ribose-5-P (5C) → Sedoheptulose-7-P (7C) + Glyceraldehyde-3-P (3C)
[2-carbon unit transferred]
Reaction B — Transaldolase:
Sedoheptulose-7-P (7C) + Glyceraldehyde-3-P (3C) → Fructose-6-P (6C) + Erythrose-4-P (4C)
[3-carbon unit transferred]
Reaction C — Transketolase:
Xylulose-5-P (5C) + Erythrose-4-P (4C) → Fructose-6-P (6C) + Glyceraldehyde-3-P (3C)
[2-carbon unit transferred]
Final output from 3 Ribulose-5-P:
- 2 Fructose-6-P and 1 Glyceraldehyde-3-P
- Both of these are glycolytic intermediates — they re-enter glycolysis
- No carbon is wasted!
THE COMPLETE PATHWAY DIAGRAM
THE CELL'S FOUR CHOICES
The beauty of the HMP shunt is its flexibility. The cell can adjust what it produces based on what it needs:
| Cell Need | What Happens |
|---|---|
| NADPH only | Oxidative phase runs. Non-oxidative phase converts Ribulose-5-P back to Glucose-6-P. Cycle keeps repeating → maximum NADPH |
| NADPH + Ribose-5-P (most common) | Oxidative phase runs → 2 NADPH made. Isomerase converts Ribulose-5-P to Ribose-5-P. Both products used |
| Ribose-5-P only (rapidly dividing cells, eg. cancer) | NADPH is already high → it inhibits G6PD → oxidative phase is OFF. Non-oxidative phase runs in reverse: Fructose-6-P and GAP (from glycolysis) → Ribose-5-P |
| NADPH + pyruvate | Both phases run. Oxidative phase makes NADPH + Ribulose-5-P → non-oxidative phase converts it to Fructose-6-P + GAP → glycolysis → pyruvate |
REGULATION OF HMP SHUNT
The main regulatory enzyme is G6PD (the very first enzyme).
Inhibition:
- NADPH is the primary inhibitor — when NADPH levels are high, G6PD is inhibited, and the pathway slows down automatically. This is classic product inhibition.
Activation (Gene induction):
- Insulin induces G6PD gene expression in the liver — after a carbohydrate-rich meal, insulin rises, G6PD synthesis increases, and more flux goes through the HMP shunt. This makes sense because the cell is in "build mode" and needs NADPH for fatty acid synthesis.
Connection to Glycolysis:
- Xylulose-5-Phosphate (a product of the HMP shunt) activates a phosphatase that increases Fructose-2,6-bisphosphate → this activates PFK-1 → this speeds up glycolysis.
- So when the HMP shunt is running fast, it also boosts glycolysis simultaneously.
WHY IS NADPH SO CRITICAL?
In Red Blood Cells — The Most Exam-Tested Concept
RBCs have no mitochondria. They cannot make NADPH from any other source. The HMP shunt is their only NADPH source. This makes RBCs extremely vulnerable if G6PD fails.
Here is how RBCs use NADPH to protect themselves:
HMP Shunt makes NADPH
↓
Glutathione Reductase uses NADPH to convert:
GSSG (oxidized glutathione) → GSH (reduced glutathione)
↓
Glutathione Peroxidase uses GSH to destroy:
H₂O₂ and lipid peroxides → water
↓
RBC membrane is protected. Hemoglobin stays intact.
If G6PD is absent:
No NADPH → cannot regenerate GSH
↓
H₂O₂ accumulates when oxidative stress occurs
↓
H₂O₂ oxidizes hemoglobin → Methemoglobin → denatures further → Heinz bodies
↓
Heinz bodies attach to inner membrane → membrane rigid and fragile
↓
RBC destroyed in spleen → HEMOLYTIC ANEMIA
All Roles of NADPH — One Complete List
| Function | Tissue |
|---|---|
| Reduce glutathione (antioxidant defense) | ALL cells, especially RBCs |
| Fatty acid synthesis (acetyl-CoA → fatty acids) | Liver, adipose tissue, lactating breast |
| Cholesterol synthesis | Liver |
| Steroid hormone synthesis | Adrenal cortex, gonads |
| Drug metabolism by Cytochrome P450 | Liver |
| Respiratory burst — kills bacteria (NADPH Oxidase) | Neutrophils, macrophages |
| Nitric oxide synthesis (eNOS) | Endothelial cells |
| Deoxynucleotide synthesis (for DNA replication) | All dividing cells |
| Fatty acid chain elongation | Endoplasmic reticulum |
G6PD DEFICIENCY — Full Details
Basic Facts
- Most common enzyme deficiency in the world (~400 million carriers)
- Inheritance: X-linked recessive
- Mainly affects males (one X chromosome — if it carries the mutant gene, no backup)
- Females are usually carriers (two X chromosomes — one normal X is enough)
- Distribution overlaps with malaria-endemic regions — heterozygous females have partial protection against Plasmodium (infected RBCs are more oxidatively fragile and lyse faster, limiting parasite spread)
Triggers of Hemolytic Crisis
| Category | Specific Examples |
|---|---|
| Antimalarials | Primaquine, Chloroquine (high doses) |
| Antibiotics | Dapsone, Sulfonamides, Nitrofurantoin |
| Other drugs | Rasburicase, Methylene blue |
| Food | Fava beans (broad beans) — contain vicine and convicine which generate H₂O₂ directly. This condition is called Favism |
| Infections | Viral or bacterial infections trigger oxidative stress through the immune response |
| Chemicals | Naphthalene (mothballs) |
Two Main Variants
| Feature | African Variant (A-) | Mediterranean Variant |
|---|---|---|
| Common in | Sub-Saharan Africa, African-Americans | Mediterranean, Middle East, India |
| Enzyme | Unstable — degrades in old RBCs | Stable but has very low activity in ALL RBCs |
| Young RBCs affected? | No — enough G6PD | Yes — all RBCs affected |
| Severity | Mild to moderate, self-limiting | Severe, can be fatal |
| Why self-limiting? | Only old RBCs lyse. New reticulocytes still have enough G6PD, so crisis stops as old cells are replaced | Every RBC is affected — no "safe" young cells |
Laboratory Findings During Crisis
| Finding | Explanation |
|---|---|
| Low hemoglobin | Hemolysis destroying RBCs |
| Elevated indirect bilirubin | Heme breakdown product from lysed RBCs |
| Elevated reticulocytes | Bone marrow trying to replace lost RBCs |
| Heinz bodies on smear | Denatured, oxidized hemoglobin clumps — stain with crystal violet or methyl violet |
| G6PD level may appear normal | During crisis, old low-G6PD cells have already lysed. Remaining cells are young reticulocytes with relatively higher G6PD. Wait 2-3 weeks after crisis to test reliably. |
Treatment
- Identify and remove the trigger (stop the drug, treat infection)
- Avoid fava beans, naphthalene, triggering drugs permanently
- Supportive care — IV fluids, folic acid supplementation
- Blood transfusion for severe anemia
- No enzyme replacement therapy available currently
THIAMINE (VITAMIN B1) DEFICIENCY AND HMP SHUNT
Transketolase, the enzyme of Phase 2, requires Thiamine Pyrophosphate (TPP) as its cofactor. If Vitamin B1 is deficient:
- Transketolase cannot transfer 2-carbon units
- Phase 2 fails — carbon skeletons pile up as Ribulose-5-P
- Cannot convert HMP intermediates back to glycolytic intermediates
- Also affects PDC and alpha-KG dehydrogenase (which also need TPP)
Diagnostic test: Erythrocyte Transketolase Activation Test
- Measure RBC transketolase activity BEFORE and AFTER adding TPP in the test tube
- If B1 is sufficient: adding TPP causes less than 15% increase in activity (enzyme already saturated with TPP)
- If B1 is deficient: adding TPP causes more than 15-20% increase (enzyme was starved of its cofactor)
- This test can detect deficiency even before symptoms appear — it is more sensitive than direct thiamine measurement
CHRONIC GRANULOMATOUS DISEASE (CGD)
This disease shows what happens when NADPH oxidase — the enzyme that uses NADPH to kill bacteria — stops working.
Deficiency: NADPH Oxidase (in neutrophils and macrophages)
Normal killing mechanism (Respiratory Burst):
NADPH + O₂ → NADPH Oxidase → Superoxide (O₂•⁻)
↓
Superoxide dismutase → H₂O₂
↓
Myeloperoxidase → Hypochlorous acid (HOCl) — bleach — kills bacteria
In CGD: The neutrophil engulfs bacteria but cannot kill them. The bacteria survive inside the phagocyte and cause recurrent, deep-seated infections.
Organisms that cause infections in CGD: Catalase-positive bacteria and fungi:
- Staphylococcus aureus (most common)
- Aspergillus species (most common fungal cause)
- Serratia, Nocardia, Burkholderia
Why catalase-positive organisms? Normal organisms produce H₂O₂ themselves during metabolism, which helps partially compensate inside the defective phagocyte. Catalase-positive organisms destroy their own H₂O₂ — so even that tiny killing mechanism is gone.
Diagnosis: Nitroblue Tetrazolium (NBT) Test
- Normal neutrophils reduce yellow NBT dye to blue-purple formazan using superoxide
- CGD neutrophils: cannot make superoxide → NBT remains yellow/colorless
Treatment: Prophylactic trimethoprim-sulfamethoxazole (TMP-SMX), prophylactic itraconazole, interferon-gamma (IFN-γ), bone marrow transplant (only curative option)
IMPORTANT INTERMEDIATES TO KNOW
| Compound | Carbons | Produced By | Fate |
|---|---|---|---|
| Ribulose-5-P | 5C | Phase 1 (oxidative phase) | → Ribose-5-P or Xylulose-5-P |
| Ribose-5-P | 5C | Isomerase from Ribulose-5-P | → Nucleotide synthesis |
| Xylulose-5-P | 5C | Epimerase from Ribulose-5-P | → Carbon-shuffling via transketolase |
| Sedoheptulose-7-P | 7C | Transketolase (Reaction A) | → Transaldolase |
| Erythrose-4-P | 4C | Transaldolase (Reaction B) | → Transketolase again; also aromatic amino acid synthesis in bacteria |
| Fructose-6-P | 6C | Non-oxidative phase output | → Re-enters glycolysis at Step 2 |
| Glyceraldehyde-3-P | 3C | Non-oxidative phase output | → Re-enters glycolysis at Step 6 |
COMPLETE HIGH-YIELD EXAM TABLE
| Question | Answer |
|---|---|
| Rate-limiting enzyme of HMP shunt | G6PD |
| G6PD is inhibited by | NADPH (product inhibition) |
| G6PD is induced by | Insulin (in liver) |
| Cofactor for Transketolase | Thiamine — Vitamin B1 (TPP) |
| Cofactor for Transaldolase | None |
| Only NADPH source in RBCs | HMP Shunt (no mitochondria in RBCs) |
| Most common enzyme deficiency worldwide | G6PD deficiency |
| Inheritance of G6PD deficiency | X-linked recessive |
| What are Heinz bodies? | Denatured oxidized hemoglobin clumps inside RBCs |
| Heinz body stain | Crystal violet / Methyl violet |
| Favism is caused by | Fava beans triggering hemolysis in G6PD-deficient people |
| Test for B1 deficiency using HMP enzyme | RBC Transketolase Activity Test |
| CGD deficiency | NADPH Oxidase |
| CGD test | Nitroblue Tetrazolium (NBT) test |
| Phase 1 is | Irreversible |
| Phase 2 is | Reversible |
| ATP produced in HMP shunt | Zero |
| CO2 is produced in | Step 3 only (by 6-Phosphogluconate Dehydrogenase) |
| Net equation (per G6P) | 1 G6P + 2 NADP+ → 1 Ribulose-5-P + 2 NADPH + CO2 |
ONE-PAGE SUMMARY
Glucose-6-Phosphate
│
▼ [G6PD — Rate-limiting, needs NADP+] → NADPH #1
6-Phosphoglucono-δ-Lactone
│
▼ [Gluconolactonase — adds water]
6-Phosphogluconate
│
▼ [6-PGD — oxidative decarboxylation] → NADPH #2 + CO2
Ribulose-5-Phosphate (5C)
│
─────┴──────────────────
│ │
[Isomerase] [Epimerase]
↓ ↓
Ribose-5-P Xylulose-5-P
(nucleotides) │
[Transketolase + Transaldolase]
↓
Fructose-6-P + Glyceraldehyde-3-P
↓
RE-ENTER GLYCOLYSIS
Sources: Basic Medical Biochemistry: A Clinical Approach 6e (pp. 962-971) | Harper's Illustrated Biochemistry 32e (pp. 203-210) | Lippincott Illustrated Reviews: Biochemistry 8e
All done in clean English! If you want the next topic — Lipid Metabolism, Protein Metabolism, Vitamins, Enzymes, or anything else — just ask!
Blood glucose regulation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
All the textbook material and diagrams are in hand. Here is the complete, clean, English-only guide.
🩸 BLOOD GLUCOSE REGULATION
Complete MBBS Notes — Simple English
Sources: Guyton & Hall Medical Physiology | Costanzo Physiology 7e | Basic Medical Biochemistry 6e
WHY DOES BLOOD GLUCOSE NEED TO BE REGULATED?
Normal fasting blood glucose = 70–100 mg/dL (or 80–90 mg/100 mL)
After a meal it rises to 120–140 mg/dL, but returns to normal within 2 hours.
The body keeps glucose in this tight range for two critical reasons:
Why it must not fall too low:
- The brain, retina, and gonads rely almost exclusively on glucose for energy. They cannot easily switch to fats.
- Severe hypoglycemia → coma → death
Why it must not rise too high:
- High glucose creates osmotic pressure → cellular dehydration
- Glucose spills into urine (glycosuria) → osmotic diuresis → dehydration + electrolyte loss
- Long-term high glucose damages blood vessels → heart attack, stroke, kidney failure, blindness
THE NORMAL GLUCOSE CURVE AFTER A MEAL
Blood Glucose
(mg/dL)
140 │ ╭───╮
120 │ ╱ ╲
100 │─────╱ ╲────────── ← Fasting level restored
80 │ Fasting ╲_______
└────────────────────────── Time
0 1hr 2hrs 3hrs
After eating: glucose rises. Insulin is released. Glucose is taken up by tissues. Blood glucose falls back to normal within about 2 hours.
THE FOUR MAIN DEFENDERS OF BLOOD GLUCOSE
Blood glucose is maintained by a four-layer defense system:
| Layer | Mechanism | Speed |
|---|---|---|
| 1 | Liver as a glucose buffer | Minutes |
| 2 | Insulin and glucagon (pancreatic hormones) | Minutes |
| 3 | Epinephrine + sympathetic nervous system | Minutes (in emergencies) |
| 4 | Growth hormone and cortisol | Hours to days |
SECTION 1: THE LIVER — THE GLUCOSE BUFFER
The liver is the single most important organ for moment-to-moment blood glucose control.
- After a meal, when blood glucose is HIGH: The liver takes up glucose from the portal blood and stores it as glycogen (glycogenesis) and fat. Up to two-thirds of absorbed glucose can be stored in the liver this way.
- During fasting, when blood glucose is LOW: The liver breaks down its glycogen (glycogenolysis) and makes new glucose (gluconeogenesis) and releases it into the blood.
Key fact: The liver can release free glucose because it has Glucose-6-Phosphatase — the enzyme that removes the phosphate from G6P and releases free glucose into blood. Muscle does NOT have this enzyme, so muscle glycogen stays in muscle.
Clinical consequence: Patients with severe liver disease (cirrhosis) cannot buffer blood glucose properly. They get hypoglycemia after fasting and hyperglycemia after eating — because the liver cannot absorb or release glucose normally.
SECTION 2: INSULIN — THE "FED STATE" HORMONE
What is Insulin?
- A polypeptide hormone made of 51 amino acids (two chains — A and B — linked by disulfide bonds)
- Made by beta (β) cells of the Islets of Langerhans in the pancreas
- Secreted as proinsulin → C-peptide is cleaved → active insulin released
- Think of insulin as the "hormone of abundance" — it is released when nutrients are plenty, and it tells every cell: "Store energy now"
The Insulin Receptor
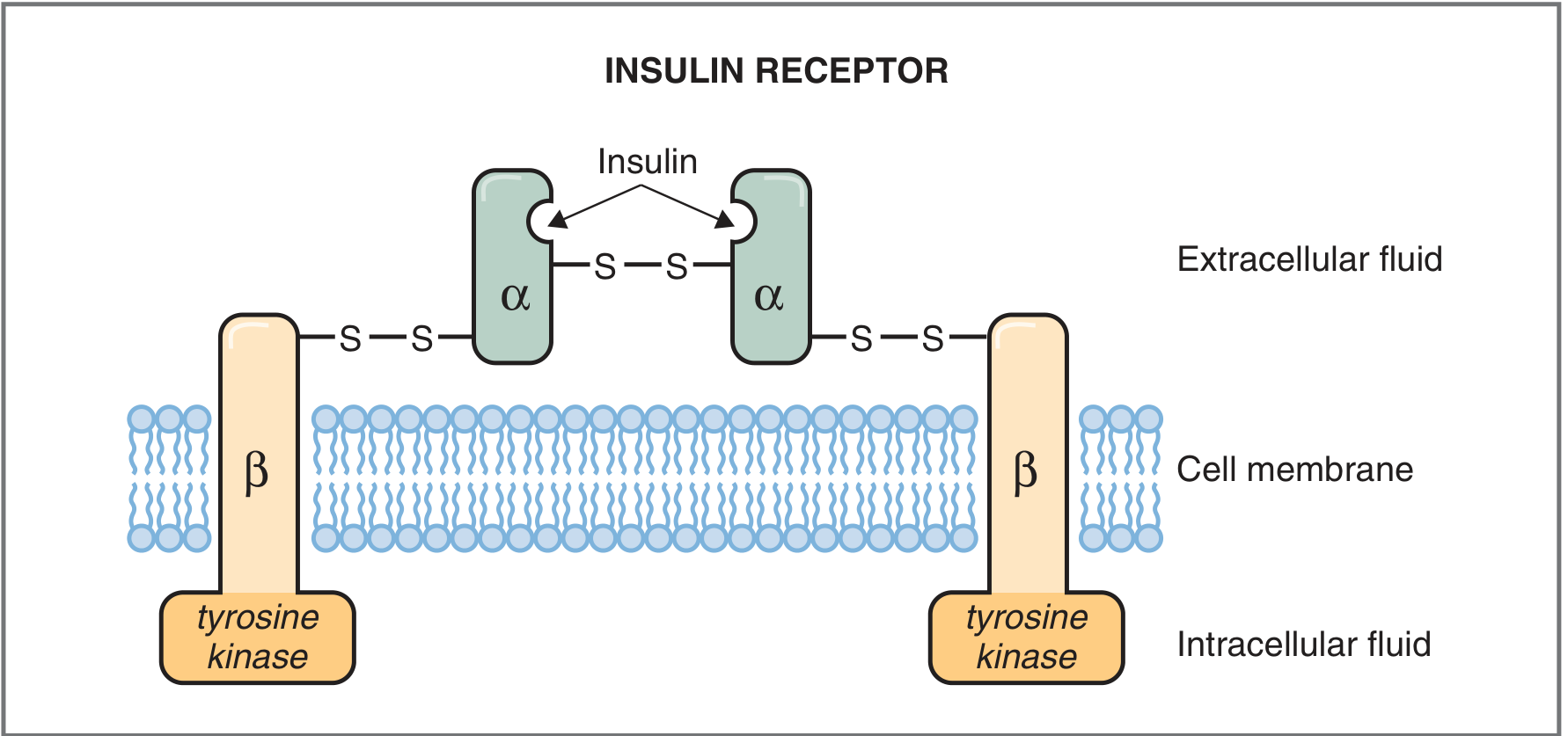
The insulin receptor is a tetramer (2α + 2β subunits):
- α subunits: Outside the cell. They bind insulin. Connected to each other by disulfide bonds.
- β subunits: Span the cell membrane. Have intrinsic Tyrosine Kinase activity on their inner (cytoplasmic) end.
How Insulin Works — Step by Step:
- Insulin binds to the α subunits → causes a conformational change in the whole receptor
- This activates tyrosine kinase in the β subunits → they phosphorylate themselves (autophosphorylation)
- Activated tyrosine kinase then phosphorylates other proteins inside the cell (kinases, phosphatases, G proteins)
- These activated proteins produce all the metabolic effects of insulin
- The insulin-receptor complex is internalized by endocytosis → insulin is degraded inside the cell
- Down-regulation: Chronic high insulin → fewer insulin receptors on cell surface. This is why obese patients and Type 2 diabetics become less sensitive to insulin
The insulin receptor is a Receptor Tyrosine Kinase (RTK) — this is an exam favorite. Contrast this with glucagon which uses a GPCR → cAMP pathway.
What Triggers Insulin Secretion?
| Stimulus | Effect |
|---|---|
| High blood glucose (most important!) | Strong stimulation — rises 10–25x above baseline |
| Amino acids (especially Arginine, Lysine) | Moderate stimulation — potentiates glucose effect |
| GLP-1 and GIP (incretins from gut) | Anticipatory boost — released when food enters the gut |
| Gastrin, Secretin, CCK | Minor stimulation |
| Parasympathetic nerves | Stimulate insulin release |
| Glucagon (at high levels) | Stimulates insulin (alpha→beta cell crosstalk) |
| Growth hormone, Cortisol (prolonged) | Stimulate insulin secretion (and cause insulin resistance) |
Incretins (GLP-1 and GIP): Released from gut cells when food enters the intestine. They signal the pancreas to prepare insulin release BEFORE glucose even reaches the blood. This is called the incretin effect — it explains why oral glucose raises insulin more than IV glucose at the same dose. This is the basis for GLP-1 agonist drugs (Semaglutide, Liraglutide) used in Type 2 Diabetes.
Sympathetic nerves: During stress and exercise, sympathetic stimulation inhibits insulin secretion and increases glucagon. This makes sense — during a fight-or-flight response, you want glucose available in the blood, not being stored.
What Does Insulin Do?
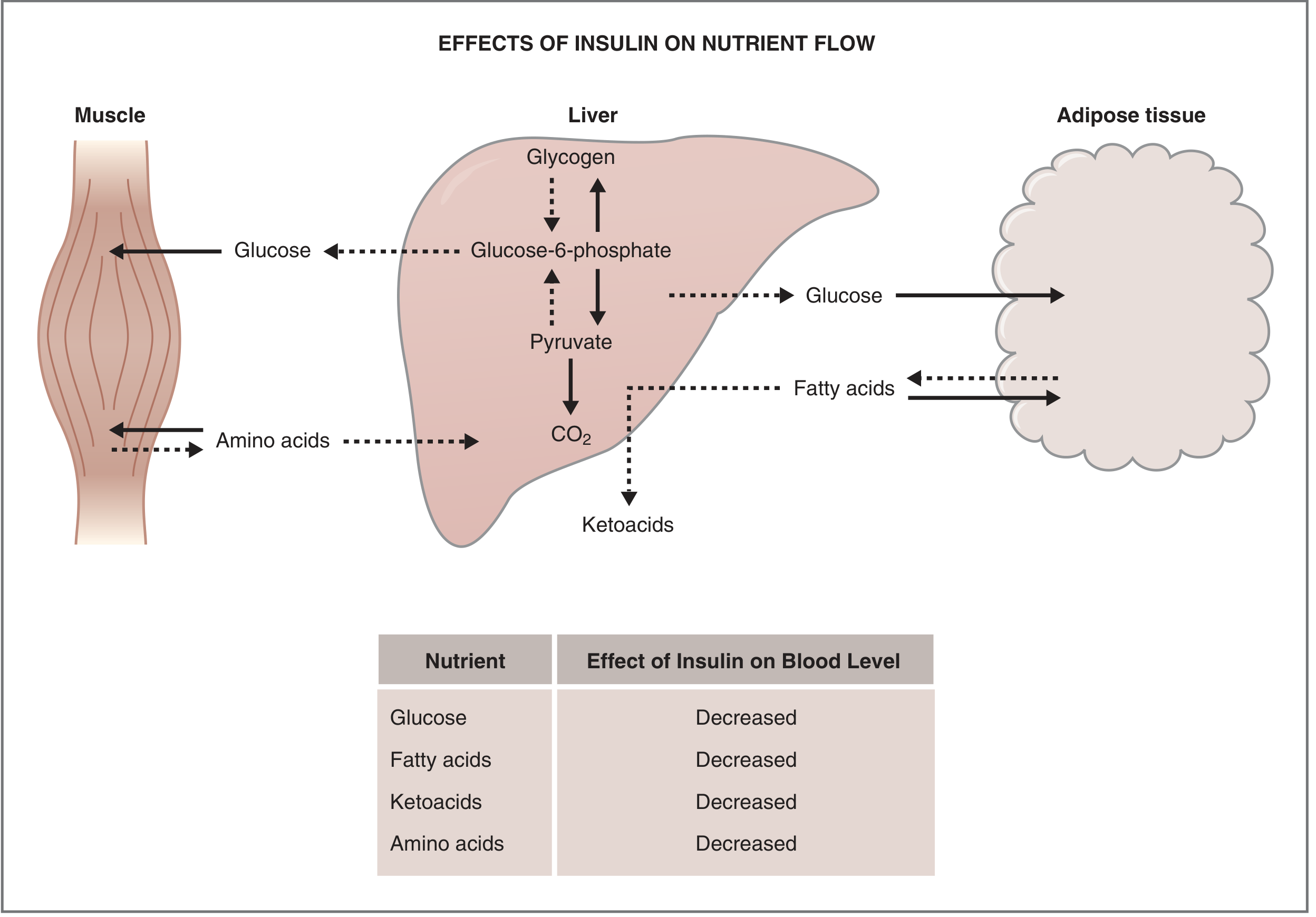
On Glucose (most important):
| Action | Mechanism |
|---|---|
| Increases glucose uptake into muscle and fat | Moves GLUT-4 transporters from intracellular vesicles to the cell surface |
| Increases glycogen synthesis (liver + muscle) | Activates Glycogen Synthase (via phosphatase) |
| Decreases glycogen breakdown | Inactivates Glycogen Phosphorylase |
| Decreases gluconeogenesis | Reduces PEPCK; increases F-2,6-bisP → activates PFK-1 away from gluconeogenesis |
| Increases glycolysis | Activates PFK-1, Pyruvate Kinase, PDC |
On Fat:
| Action | Effect |
|---|---|
| Activates Lipoprotein Lipase (LPL) in fat tissue | Takes fatty acids out of blood → stored in adipocytes |
| Inhibits Hormone Sensitive Lipase (HSL) | Stops fat breakdown → less fatty acids released |
| Promotes fatty acid synthesis in liver | Excess glucose → fat storage |
| Inhibits ketogenesis | Less fatty acid oxidation → less acetyl-CoA → fewer ketone bodies |
On Protein:
| Action | Effect |
|---|---|
| Increases amino acid uptake by muscle | Blood amino acid levels fall |
| Increases protein synthesis | Anabolic effect on muscle |
| Decreases protein degradation | Protects muscle mass |
On Potassium:
- Insulin drives K+ into cells by stimulating Na+/K+ ATPase
- Clinically important: Insulin is used to treat hyperkalemia (high potassium) in emergency medicine
- Diabetic ketoacidosis: When insulin is replaced, K+ shifts into cells → watch for hypokalemia
One-Line Summary of Insulin's Effect on Blood Levels:
Insulin lowers blood glucose, blood fatty acids, blood ketoacids, blood amino acids, and blood K+.
SECTION 3: GLUCAGON — THE "FASTING STATE" HORMONE
What is Glucagon?
- A 29 amino acid polypeptide hormone (molecular weight 3485)
- Made by alpha (α) cells of the Islets of Langerhans
- The "hyperglycemic hormone" — its job is to RAISE blood glucose
- Even 1 µg/kg of glucagon can increase blood glucose by ~20 mg/dL within 20 minutes
What Triggers Glucagon Secretion?
| Stimulus | Effect |
|---|---|
| Low blood glucose (most important!) | Strong stimulation — the lower the glucose, the more glucagon |
| Amino acids (especially Arginine) | Stimulates glucagon (makes sense — pure protein meal has no glucose, glucagon prevents hypoglycemia) |
| Sympathetic nerve stimulation | Stimulates glucagon (stress response) |
| Exercise | Increases glucagon |
| High blood glucose | INHIBITS glucagon |
| Insulin | INHIBITS glucagon (paracrine effect in islets) |
| Somatostatin | INHIBITS glucagon |
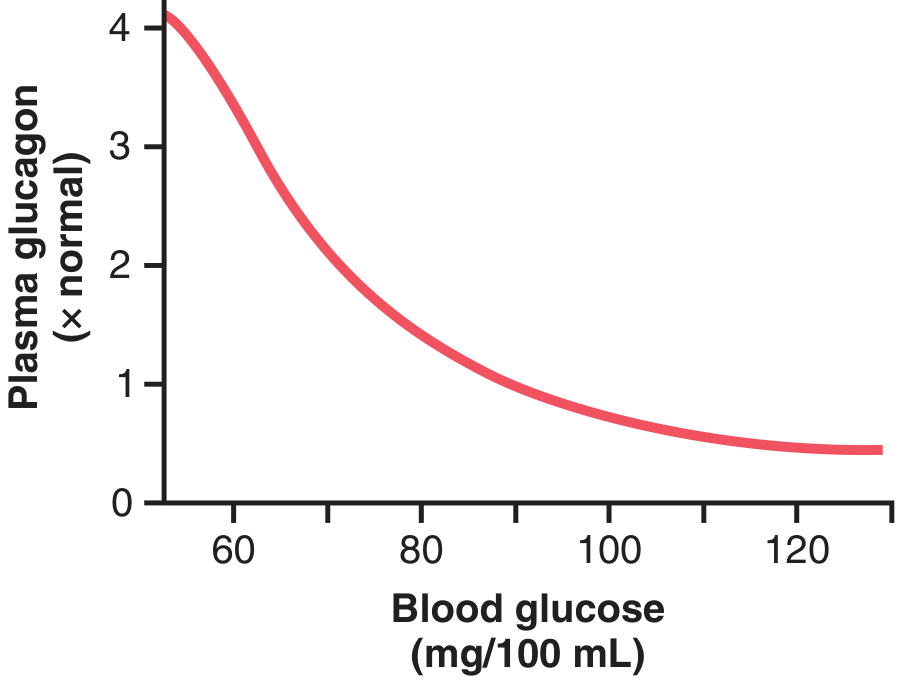
Note the inverse relationship: as blood glucose falls, glucagon rises sharply. As blood glucose rises, glucagon is suppressed.
The Glucagon Receptor — Signal Cascade
Glucagon acts through a GPCR (G Protein Coupled Receptor) → cAMP pathway:
Glucagon binds GPCR on liver cell
↓
G protein activates Adenylyl Cyclase
↓
ATP → cAMP (cyclic AMP)
↓
cAMP activates Protein Kinase A (PKA)
↓
PKA phosphorylates:
• Phosphorylase Kinase → ACTIVE
• Glycogen Phosphorylase → ACTIVE (glycogen breakdown ON)
• Glycogen Synthase → INACTIVE (glycogen synthesis OFF)
• PEPCK induced → Gluconeogenesis ON
↓
Glucose released into blood → blood glucose rises
This cascade is a million-fold amplification system — tiny amounts of glucagon produce a massive glucose response.
What Does Glucagon Do?
Primary Effects (at normal concentrations):
1. Glycogenolysis in Liver:
- Breaks down liver glycogen → releases glucose into blood
- Infusion of glucagon for 4 hours can completely deplete all liver glycogen stores
2. Gluconeogenesis in Liver:
- Even after glycogen is depleted, glucagon continues to raise blood glucose
- Stimulates amino acid uptake by liver
- Activates enzymes for gluconeogenesis, especially PEPCK (Pyruvate → PEP step)
Secondary Effects (at high concentrations):
- Activates Hormone-Sensitive Lipase in adipose tissue → releases fatty acids from fat → provides fuel for gluconeogenesis
- Inhibits triglyceride storage in liver → more fatty acids available for other tissues
- Strengthens heart contraction (pharmacological doses)
- Inhibits gastric acid secretion
SECTION 4: THE FOUR-HORMONE ORCHESTRA
At any given moment, blood glucose is controlled by the balance between four hormones:
| Hormone | Source | Raises or Lowers Glucose | Speed |
|---|---|---|---|
| Insulin | Pancreatic β cells | ⬇ LOWERS | Fast (minutes) |
| Glucagon | Pancreatic α cells | ⬆ RAISES | Fast (minutes) |
| Epinephrine (Adrenaline) | Adrenal medulla | ⬆ RAISES | Fast (minutes) |
| Cortisol | Adrenal cortex | ⬆ RAISES | Slow (hours–days) |
| Growth Hormone | Anterior pituitary | ⬆ RAISES | Slow (hours–days) |
EPINEPHRINE (Adrenaline) — Emergency Glucose Raiser
Released during: stress, exercise, hypoglycemia, shock, anxiety
How it raises glucose:
- In liver: activates glycogenolysis (same cAMP cascade as glucagon) → glucose floods into blood within minutes
- In adipose tissue: activates Hormone-Sensitive Lipase → releases fatty acids → provides fuel + reduces glucose use by other tissues
Note: Epinephrine raises BOTH blood glucose AND blood fatty acids. Glucose goes up for the brain; fatty acids go up for muscles. This is ideal for a fight-or-flight scenario.
Clinical: Beta-blockers (propranolol) block epinephrine's effect → can mask hypoglycemia symptoms (palpitations, tremor) in diabetic patients on insulin. Important drug interaction to know.
CORTISOL — Slow but Sustained Glucose Raiser
Released during: prolonged stress, fasting, illness, Cushing syndrome
How it raises glucose:
- Promotes gluconeogenesis — induces PEPCK and other gluconeogenic enzymes in the liver
- Promotes protein breakdown in muscle → amino acids released as gluconeogenic precursors
- Inhibits glucose uptake by peripheral tissues (anti-insulin effect)
- Promotes fat breakdown — provides glycerol for gluconeogenesis
Clinical: Long-term steroid treatment (prednisolone, dexamethasone) → iatrogenic Cushing's syndrome → steroid-induced diabetes. Patients on chronic steroids must have blood glucose monitored.
GROWTH HORMONE — The Other Slow Glucose Raiser
Released during: sleep, exercise, hypoglycemia, puberty
How it raises glucose:
- Inhibits glucose uptake and utilization by peripheral tissues → cells switch to fat burning instead
- Promotes lipolysis → fatty acids become the preferred fuel
- These effects develop over hours, not minutes
Clinical: Acromegaly (excess GH in adults) → persistent glucose-raising effects → diabetes mellitus in up to 25% of acromegaly patients. Similarly, gigantism in children. Somogyi effect: Overnight growth hormone surge can cause early morning hyperglycemia in insulin-treated diabetics.
SOMATOSTATIN — The Brake Pedal
- Released from delta (δ) cells of pancreatic islets
- Inhibits BOTH insulin AND glucagon secretion
- Also inhibits GH secretion from pituitary
- Acts as a paracrine regulator — fine-tunes the insulin-glucagon balance locally within the islet
- Pharmacological analogs: Octreotide — used to treat acromegaly, glucagonoma, carcinoid syndrome, and some types of severe hypoglycemia (e.g., insulinoma)
SECTION 5: WHAT HAPPENS AT DIFFERENT PHYSIOLOGICAL STATES
Fed State (After a Meal)
Blood glucose rises → Insulin rises → Glucagon falls
| Organ | What Happens |
|---|---|
| Pancreas β cells | Secrete insulin (10–25x basal levels) |
| Liver | Takes up glucose → makes glycogen + fat; stops gluconeogenesis |
| Muscle | GLUT-4 inserted → glucose enters → glycogen and protein synthesis |
| Adipose | GLUT-4 inserted → glucose enters → fat synthesis; lipolysis stopped |
| Brain | Continues to use glucose (GLUT-1 and GLUT-3, always active) |
Fasting State (4–12 Hours Without Food)
Blood glucose starts falling → Insulin falls → Glucagon rises
| Organ | What Happens |
|---|---|
| Liver | Glycogenolysis begins → releases glucose to maintain 80 mg/dL |
| Adipose | Lipolysis begins (HSL activated) → fatty acids released |
| Muscle | Uses fatty acids and ketones for energy instead of glucose |
| Brain | Still uses glucose (liver supplying it) |
| Pancreas α cells | Glucagon secretion rises → drives liver glycogenolysis |
Prolonged Fasting / Starvation (24–48+ Hours)
Liver glycogen is depleted → Gluconeogenesis is the ONLY source of blood glucose
| Source | What Provides |
|---|---|
| Muscle protein | Amino acids (esp. Alanine) → liver → glucose |
| Adipose fat | Glycerol → liver → glucose; Fatty acids → liver → ketone bodies |
| Kidney cortex | Also contributes to gluconeogenesis |
The brain eventually adapts to use ketone bodies (acetoacetate, β-hydroxybutyrate) — this reduces the brain's demand for glucose and spares muscle protein from being broken down.
Exercise
During exercise: muscle consumes glucose rapidly → blood glucose tends to fall
| Response | Mechanism |
|---|---|
| Glucagon rises | Drives liver glycogenolysis |
| Epinephrine rises | Fast glycogenolysis + lipolysis |
| Muscle glycogen breakdown | AMP rises in muscle (low ATP) → activates glycogen phosphorylase |
| Liver gluconeogenesis | Lactate from muscle → Cori cycle → liver → glucose |
| Insulin falls | GLUT-4 still inserted by muscle contractions (insulin-independent mechanism during exercise) |
SECTION 6: THE INSULIN/GLUCAGON RATIO — THE MASTER SWITCH
The body does not respond to either hormone alone. What matters is the ratio:
High Insulin / Low Glucagon = Fed State = BUILD and STORE
Low Insulin / High Glucagon = Fasting State = BREAK DOWN and RELEASE
This ratio controls 4 hepatic processes simultaneously:
| Ratio | Glycolysis | Gluconeogenesis | Glycogenesis | Glycogenolysis |
|---|---|---|---|---|
| High Insulin:Glucagon (fed) | ON | OFF | ON | OFF |
| Low Insulin:Glucagon (fasting) | OFF | ON | OFF | ON |
The molecular switch is Fructose-2,6-bisphosphate (F2,6-bisP):
- Insulin → activates PFK-2 → increases F2,6-bisP → activates PFK-1 → glycolysis ON; FBPase-1 OFF → gluconeogenesis OFF
- Glucagon → activates PKA → phosphorylates PFK-2/FBPase bifunctional enzyme → F2,6-bisP falls → PFK-1 OFF; FBPase-1 ON → gluconeogenesis ON
SECTION 7: WHAT HAPPENS WHEN REGULATION FAILS
Hypoglycemia (Blood Glucose < 70 mg/dL)
Causes:
- Too much insulin (diabetic taking excess dose)
- Insulinoma (insulin-secreting tumor)
- Alcohol (blocks gluconeogenesis)
- Addison's disease (no cortisol)
- Prolonged starvation
Body's counter-regulatory response (in order):
- Insulin secretion stops (first and fastest)
- Glucagon rises (within minutes)
- Epinephrine rises (triggers: glucose < 60 mg/dL) → causes sweating, tremor, palpitations, anxiety
- Cortisol and GH rise (glucose < 55 mg/dL) → slower, sustained response
- Hypothalamus detects low glucose → activates sympathetic nervous system → hunger, sweating
Symptoms of hypoglycemia:
- Adrenergic (from epinephrine): Sweating, palpitations, tremor, anxiety, pallor
- Neuroglycopenic (brain starved of glucose): Confusion, headache, seizures, coma
Whipple's Triad (classic criteria for true hypoglycemia):
- Symptoms of hypoglycemia
- Blood glucose < 55 mg/dL at time of symptoms
- Symptoms relieved by giving glucose
Hyperglycemia (Blood Glucose > 126 mg/dL fasting)
Causes: Diabetes mellitus (Type 1 or Type 2), steroids, Cushing's, acromegaly, stress, pancreatitis
Consequences of uncontrolled hyperglycemia:
- Osmotic effects: Cellular dehydration, glycosuria, polyuria (osmotic diuresis), polydipsia
- Non-enzymatic glycation: Glucose attaches to proteins non-enzymatically → HbA1c (diagnostic marker), glycated LDL, glycated basement membranes
- Diabetic complications: Microangiopathy (retinopathy, nephropathy, neuropathy), macroangiopathy (heart attack, stroke)
- DKA (Type 1): No insulin → no glucose uptake → fat burned → ketone bodies → metabolic acidosis, Kussmaul breathing, acetone breath
- HHS (Type 2): Extreme hyperglycemia → severe dehydration → coma without significant ketosis (some residual insulin prevents ketogenesis)
SECTION 8: GLUCOSE DIAGNOSTIC THRESHOLDS
| Test | Normal | Pre-Diabetes | Diabetes |
|---|---|---|---|
| Fasting blood glucose | < 100 mg/dL | 100–125 mg/dL | ≥ 126 mg/dL |
| 2-hour OGTT (75g glucose) | < 140 mg/dL | 140–199 mg/dL | ≥ 200 mg/dL |
| HbA1c | < 5.7% | 5.7–6.4% | ≥ 6.5% |
| Random glucose | — | — | ≥ 200 + symptoms |
HbA1c: Reflects average blood glucose over the past 2–3 months (lifespan of RBC). Used for diagnosis and monitoring of diabetes. Falsely low in hemolytic anemia (RBCs die fast, not enough time to glycate). Falsely high in iron deficiency (RBCs live longer than normal).
EXAM HIGH-YIELD TABLE
| Fact | Answer |
|---|---|
| Normal fasting blood glucose | 70–100 mg/dL |
| Insulin made by | Pancreatic β cells |
| Glucagon made by | Pancreatic α cells |
| Somatostatin made by | Pancreatic δ cells |
| Insulin receptor type | Receptor Tyrosine Kinase (RTK) |
| Glucagon receptor type | GPCR → cAMP → PKA |
| Insulin's most potent stimulator | Blood glucose (direct) |
| Most potent activator of PFK-1 | Fructose-2,6-bisphosphate |
| Hormone that drives GLUT-4 insertion | Insulin |
| Glucose transporter in brain | GLUT-1, GLUT-3 (insulin-independent) |
| Glucose transporter in pancreas | GLUT-2 (glucose sensor) |
| Organ that can release free glucose | Liver and kidney (have G6Pase) |
| Organ that CANNOT release free glucose | Muscle (no G6Pase) |
| Incretins (potentiate insulin) | GLP-1 and GIP |
| Drug that mimics GLP-1 | Semaglutide, Liraglutide |
| Drug that blocks sympathetic hypoglycemia symptoms | Beta-blockers |
| Insulin + glucose → treat | Hyperkalemia |
| Whipple's Triad | Hypoglycemia symptoms + low glucose on test + relief with glucose |
| HbA1c reflects | Average glucose over 2–3 months |
| Counter-regulatory hormones | Glucagon, Epinephrine, Cortisol, GH (all raise glucose) |
ONE-PAGE VISUAL SUMMARY
BLOOD GLUCOSE CONTROL
HIGH GLUCOSE LOW GLUCOSE
(After meal) (Fasting/starvation)
↓ ↓
β cells secrete α cells secrete
INSULIN GLUCAGON
↓ ↓
Liver: stores glucose as Liver: breaks down glycogen
glycogen, stops gluco- and makes new glucose via
neogenesis gluconeogenesis
↓ ↓
Muscle: GLUT-4 inserts → Muscle: uses fatty acids
takes up glucose and ketones instead
↓ ↓
Adipose: stores fat, Adipose: releases fatty
stops lipolysis acids (HSL activated)
↓ ↓
Blood glucose FALLS ←──────── If still low ──────────→
Epinephrine released
(glycogenolysis + lipolysis)
If persistent:
Cortisol + GH released
(reduces peripheral glucose use)
Sources: Guyton and Hall Textbook of Medical Physiology (pp. 2777–2937) | Costanzo Physiology 7e (pp. 463–510) | Basic Medical Biochemistry 6e (pp. 1582–1584)
This covers the full topic — normal values, insulin mechanism, glucagon mechanism, all counter-regulatory hormones, fed vs fasting states, hypoglycemia, hyperglycemia, and exam MCQ points. Want to continue with Lipid Metabolism, Diabetes in detail, or Hormones of the Pancreas next?
This is a shared conversation. Sign in to Orris to start your own chat.