Normal labor mechanism. NWHO. Care guideline on this.
Reading File
Finding Sources
Finding Sources
Searching the Web
WHO intrapartum care guidelines 2018 normal labour mechanism recommendations
Reading File
Reading File
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK513802
Reading File
Reading File
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK513802
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I now have comprehensive data to write a detailed answer. Let me compile everything.
Normal Labor Mechanism & WHO Intrapartum Care Guidelines
The "3 Ps" - Determinants of Labor
Labor is not a passive process. Successful vaginal delivery depends on the interaction of three variables:
- Powers - uterine contractions (frequency, intensity, duration)
- Passenger - fetal size, position, and attitude (flexion/extension)
- Passage - bony pelvis dimensions, shape, and pelvic floor soft tissue resistance
- Creasy & Resnik's Maternal-Fetal Medicine, p. 817
Stages of Labor
| Stage | From | To |
|---|---|---|
| First (latent + active) | Onset of regular painful contractions + cervical change | Full cervical dilatation (10 cm) |
| Second | Full dilatation | Delivery of the baby |
| Third | Delivery of the baby | Delivery of the placenta |
| Fourth | Delivery of placenta | 1 hour postpartum |
- Textbook of Family Medicine 9e, p. 502
First Stage of Labor
Latent Phase
- Variable in length: up to 20 hours in nulliparas, 14 hours in multiparas
- Minimal cervical dilation; cervix softens, effaces, and moves anterior
- Irregular, often painless contractions
- Mean cervical dilation in last 3 days before labor: ~1.8 cm (nulliparas), 2.2 cm (multiparas)
Active Phase
- Begins at approximately 5 cm dilatation (updated from the older Friedman threshold of 3-4 cm)
- Rapid cervical dilatation phase
- Classical Friedman minimum rates: ≥1.2 cm/hr (nulliparas), ≥1.5 cm/hr (multiparas)
- Contractions: every 2-3 minutes, ~60 seconds duration, ~40 mmHg intensity
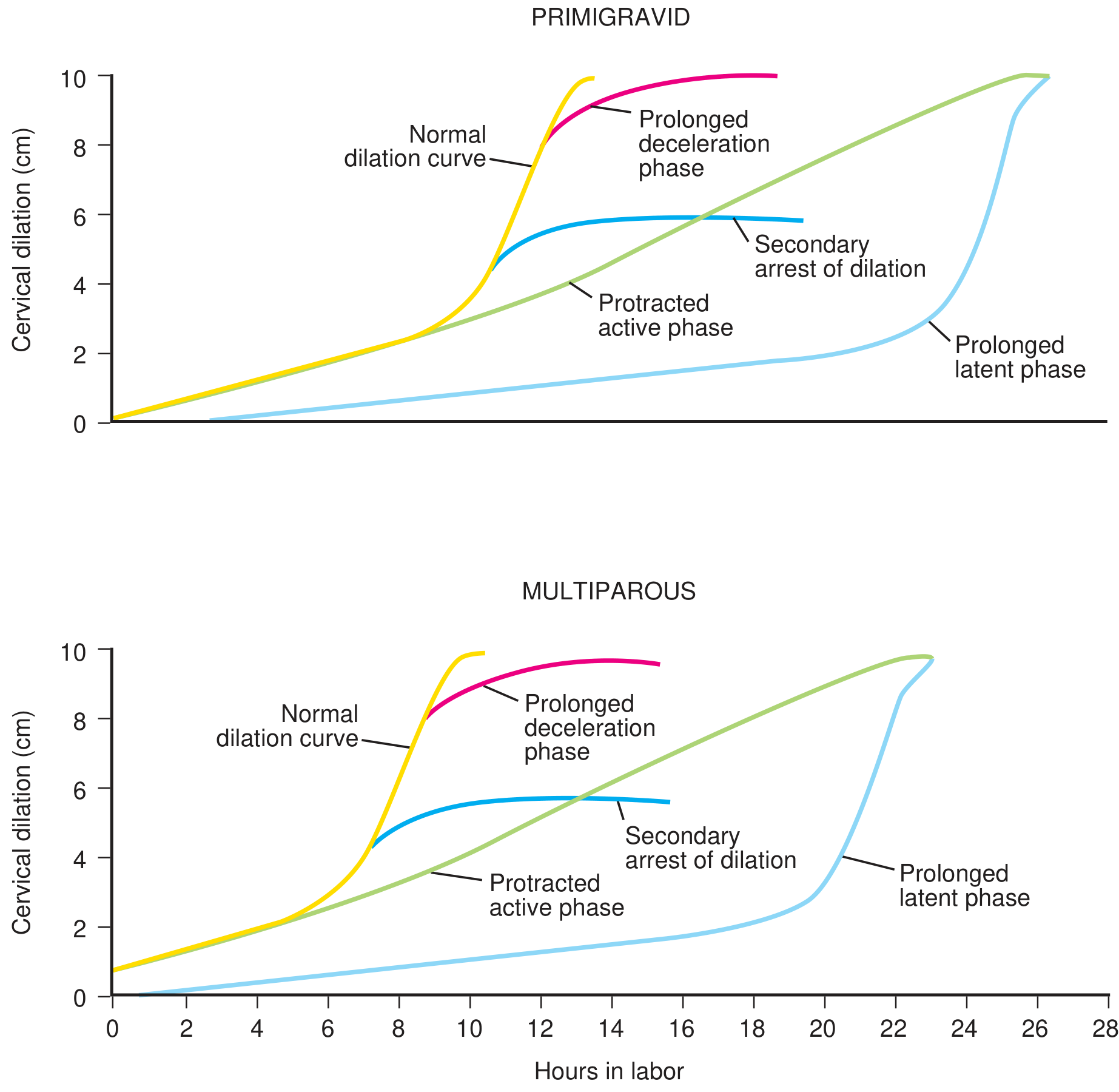
Friedman Labor Curve (Creasy & Resnik Table 40.1)
| Characteristic | Nulliparas | Multiparas |
|---|---|---|
| Latent phase duration | 6.4 ± 5.1 hr | 4.8 ± 4.9 hr |
| Active phase duration | 4.6 ± 3.6 hr | 2.4 ± 2.2 hr |
| Max active-phase dilation rate | >1.2 cm/hr | >1.5 cm/hr |
Second Stage
- From full cervical dilatation to delivery of the baby
- Average duration: ~50 minutes in nulliparas, ~20 minutes in multiparas
- Woman has an involuntary urge to bear down with contractions
- Maternal expulsive forces combine with uterine contractions to drive descent
Third Stage
- Delivery of the placenta
- Signs of placental separation: lengthening of the cord, gush of blood, change in uterine fundal contour
- Normally completed within 30 minutes
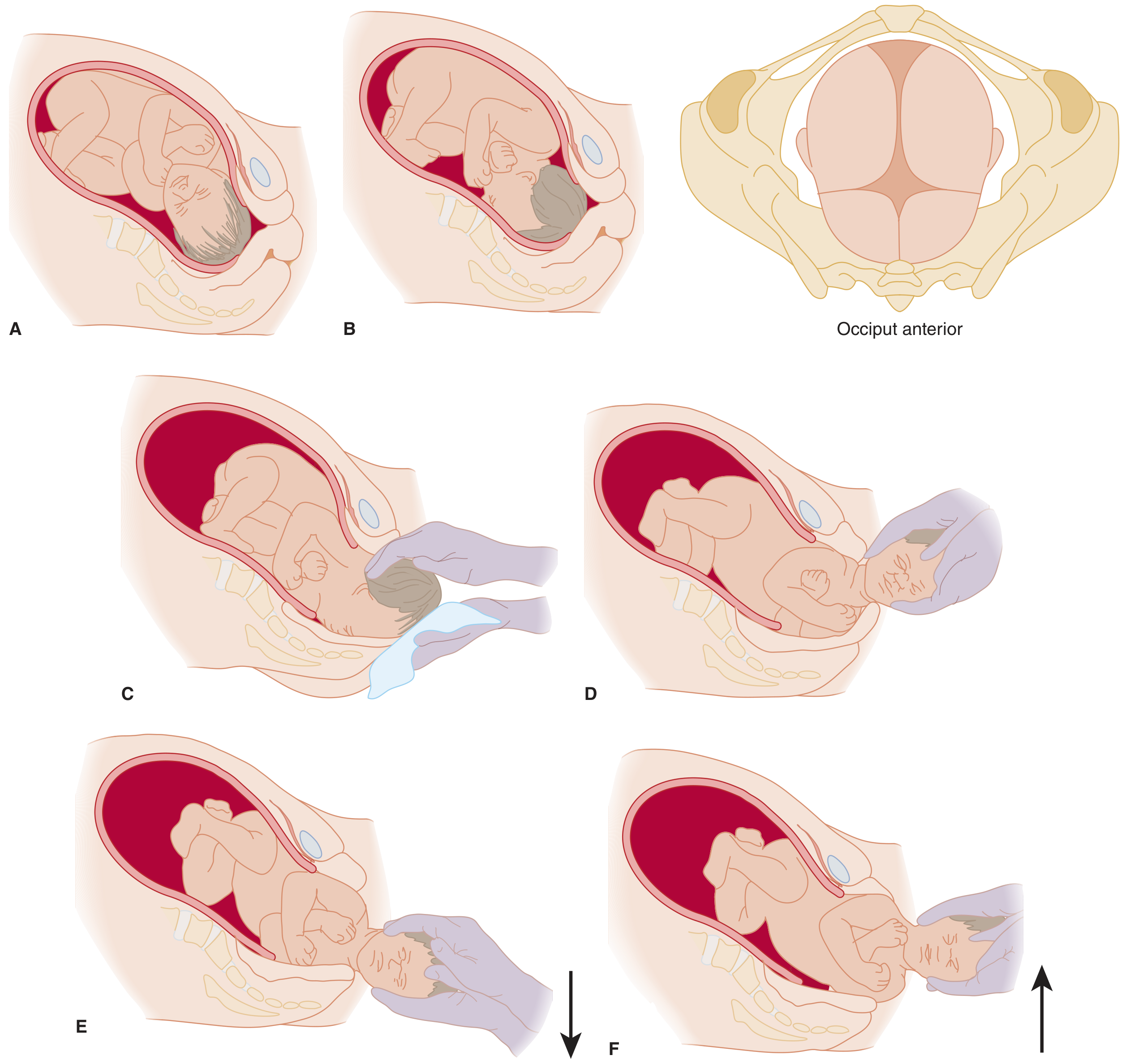
Cardinal Movements of Labor (Vertex Presentation - LOA/OA)
Because the fetal head and maternal pelvis are asymmetric, the fetus must execute a series of orchestrated rotations to negotiate the birth canal. There are 7 cardinal movements (some sources list 6 by combining certain steps):
1. Engagement
- The widest diameter of the fetal head (biparietal diameter, ~9.5 cm) descends below the plane of the pelvic inlet
- In nulliparas, often occurs 2-4 weeks before labor ("lightening")
- In multiparas, may not occur until labor begins
- Presenting diameter in well-flexed OA position is the suboccipitobregmatic (~9.5 cm)
2. Descent
- Progressive downward movement of the fetal presenting part through the pelvis
- Begins before engagement and continues throughout labor
- Driven by uterine contraction pressure, amniotic fluid pressure, and maternal bearing-down efforts
- Rate accelerates in late first stage and continues linearly into second stage
3. Flexion
- As the head meets resistance from the pelvic floor, flexion increases
- Chin tucks onto the chest
- Converts the presenting diameter from the larger occipitofrontal (~11.5 cm) to the smaller suboccipitobregmatic (~9.5 cm)
- Facilitates easier passage through the pelvis
4. Internal Rotation
- The occiput (and fetal head) rotates from the transverse or oblique position to the occiput anterior (OA) position under the pubic symphysis
- This aligns the longest fetal head diameter with the longest pelvic diameter at each level:
- Pelvic inlet: widest transversely
- Midpelvis: widest anteroposteriorly
- Driven by the levator ani and pelvic floor musculature
5. Extension
- After internal rotation, the occiput reaches the pubic symphysis
- The head extends (pivots around the subpubic arch) as the occiput, bregma, forehead, nose, mouth, and chin deliver successively over the perineum
- The suboccipital region becomes the fulcrum against the pubic arch
6. External Rotation (Restitution)
- Immediately after the head is born, it rotates back to its natural alignment with the fetal shoulders (which are still in the oblique pelvic diameter)
- Restitution: the head turns to the side it was originally facing
- Full external rotation: the occiput turns further toward the maternal thigh, bringing the shoulders into the AP diameter
7. Expulsion
-
With the next contraction, the anterior shoulder delivers under the pubic symphysis with gentle downward traction
-
Then the posterior shoulder follows with gentle upward traction
-
The body follows rapidly with the next contraction
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 3449-3474
-
Tintinalli's Emergency Medicine, p. 2011-2014
WHO Intrapartum Care Guidelines 2018 (Key Recommendations)
The WHO 2018 Intrapartum Care Guidelines contain 56 evidence-based recommendations organized by stage of labor.
Care Throughout Labor and Birth
| Recommendation | Classification |
|---|---|
| Respectful maternity care - every woman has the right to dignified, respectful care | Recommended |
| Effective communication (clear info, informed consent, emotional support) | Recommended |
| Companion of choice during labor and birth | Recommended |
| Pain relief: offer oral analgesia, breathing techniques, relaxation, warm compresses, bath/shower | Recommended |
First Stage - Assessment and Progress
| # | Recommendation | Classification |
|---|---|---|
| 7 | The 1 cm/hr partograph alert line is inaccurate to identify women at risk of adverse outcomes - not recommended for this purpose | Not recommended |
| 8 | A minimum dilation rate of 1 cm/hr is unrealistically fast for some women; slower rate alone should not be a routine indication for obstetric intervention | Not recommended |
| 9 | Labor may not naturally accelerate until 5 cm dilatation - medical interventions before 5 cm should not be routinely used | Recommended |
| 16 | Digital vaginal examination every 4 hours is recommended for routine assessment of active first stage in low-risk women | Recommended |
| 17 | Continuous CTG (cardiotocography) is NOT recommended for fetal assessment in healthy women in spontaneous labor | Not recommended |
| 18 | Intermittent auscultation (Doppler or Pinard) is recommended for healthy women in labor | Recommended |
First Stage - Interventions
| Recommendation | Classification |
|---|---|
| Use of the partograph (new WHO model) to monitor labor progress | Recommended |
| Amniotomy + early oxytocin NOT recommended to prevent prolonged labor in healthy women in spontaneous labor | Not recommended |
| Oral fluids and food are allowed during labor | Recommended |
| Upright positions and mobility encouraged throughout labor | Recommended |
| Epidural analgesia is available on request | Recommended |
Second Stage
| # | Recommendation | Classification |
|---|---|
| 33 | Second stage: normally completed within 3 hours in nulliparas, 2 hours in multiparas | Recommended |
| 34 | Women should be allowed to follow their own urge to push ("physiological pushing") | Recommended |
| 35 | Directed pushing (Valsalva/sustained breath-holding) not recommended when woman has epidural | Not recommended |
| 36 | Upright position or position of woman's choice during pushing | Recommended |
| 37 | With epidural analgesia, delay pushing 1-2 hours after full dilatation (passive second stage) | Context-specific |
| 38 | Perineal massage, warm compresses, and "hands-on" guarding of the perineum to reduce trauma | Recommended |
| 39 | Routine/liberal episiotomy is NOT recommended for spontaneous vaginal birth | Not recommended |
| 40 | Fundal pressure is NOT recommended to facilitate birth | Not recommended |
Third Stage
| # | Recommendation | Classification |
|---|---|
| 41 | Prophylactic uterotonics (oxytocin) for all births to prevent PPH | Recommended |
| 42 | Oxytocin 10 IU IM/IV is the first-line uterotonic | Recommended |
| 43 | If oxytocin unavailable: ergometrine, oxytocin+ergometrine, or oral misoprostol 600 mcg | Recommended |
| 44 | Delayed cord clamping (not earlier than 1 minute after birth) | Recommended |
| 45 | Controlled cord traction (CCT) for vaginal births where skilled attendants are available | Recommended |
| 46 | Sustained uterine massage is NOT recommended after prophylactic oxytocin | Not recommended |
Summary: Key WHO Paradigm Shifts (2018)
- Active phase now begins at 5 cm - not 3-4 cm (Friedman era). Slow progress before 5 cm should not prompt intervention.
- 1 cm/hr progress rule is abandoned as the sole criterion for normal labor - do not intervene on this alone.
- Intermittent auscultation over continuous CTG in healthy, low-risk laboring women.
- No routine episiotomy, no fundal pressure, no amniotomy purely to shorten labor.
- Woman-centred care: choice of position, companion, mobility, oral intake, pain relief options are all rights-based recommendations.
- Delayed cord clamping ≥1 minute is standard care for all births.
Sources: WHO Intrapartum Care 2018 - NCBI Bookshelf | Creasy & Resnik's Maternal-Fetal Medicine, p. 2888-2928 | Textbook of Family Medicine 9e, p. 502-503 | Tintinalli's Emergency Medicine, p. 2011-2014
Open c section wound care
Reading File
Finding Sources
Finding Sources
Searching the Web
open cesarean section wound care management dehiscence guidelines 2023 2024
Reading File
Finding Sources
Finding Sources
Reading Web Page
https://www.exxcellence.org/list-of-pearls/management-of-wou…
Finding Sources
Finding Sources
Searching PubMed
"cesarean" AND "wound dehiscence" AND "management"
Reading File
Reading File
Finding Sources
Loading Image
I have all the content I need. Here is the comprehensive answer.
Open Cesarean Section Wound Care
An "open" cesarean wound typically refers to a wound that has been deliberately opened or has spontaneously dehisced (separated), and is now being managed without primary closure - allowed to heal by secondary intention or prepared for delayed primary closure. This is one of the most common postoperative wound complications after cesarean delivery.
1. Background: Why C-Section Wounds Break Down
Wound complications (infection, seroma, hematoma, dehiscence) occur in 3-15% of cesarean deliveries. Risk factors include:
| Risk Factor | Comments |
|---|---|
| Obesity (BMI >30) | Single greatest risk factor; wound separation rates up to 34.6% in BMI >35 |
| Diabetes mellitus | Impairs neutrophil function and collagen synthesis |
| Second-stage cesarean | Greater contamination, more tissue trauma |
| Emergency vs. elective | More contamination, less prep time |
| Vertical incision | Higher wound complication rate vs. Pfannenstiel |
| Subcutaneous depth >3 cm | Risk of seroma/hematoma collection |
| Corticosteroid use | Impairs wound healing |
| Anemia / malnutrition | Reduces healing capacity |
| Chorioamnionitis | Bacterial contamination of wound |
25-30% of wound infections are caused by Staphylococcus aureus (from skin flora, not endometrial contamination).
- Creasy & Resnik's Maternal-Fetal Medicine, p. 3771
2. Initial Assessment of the Open/Dehisced Wound
Evaluate for:
- Extent of separation - probe the wound edges with a sterile swab to determine depth and width
- Fascial integrity - most important step. Is fascia intact? Complete fascial disruption = surgical emergency
- Signs of infection: erythema, warmth, induration, purulent discharge, fever, malodor
- Devitalized/necrotic tissue requiring debridement
- Seromas/hematomas - may extend further subcutaneously than the visible opening
- Necrotizing fasciitis - rapidly spreading cellulitis with systemic toxicity; immediate surgical debridement required
Probing the wound: A sterile Q-tip can assess how far the cavity extends and confirm fascial integrity. Seromas and hematomas can be deceptively large under an apparently small skin opening.
3. Management Algorithm
Open C-section wound
|
├──> Fascial disruption? → YES → Surgical emergency: explore + repair fascia
| (skin may be left open or closed)
|
└──> Fascia intact? → Proceed with conservative wound management
|
├──> Infected? → Cultures + broad-spectrum antibiotics
| + debridement + irrigation + open packing
|
├──> Seroma/Hematoma? → Open/drain if large; observe if small
|
└──> Clean open wound → Moist wound healing
→ NPWT if large/deep
→ Delayed primary closure when ready
4. Step-by-Step Wound Care
Step 1: Open and Explore
- Remove sutures or staples along the separation
- Open the wound sufficiently to allow inspection and treatment
- Drain any collection (seroma, hematoma, pus)
- Obtain wound swab for culture and sensitivity
Step 2: Debridement
- Remove all devitalized, necrotic, and sloughy tissue
- Sharp debridement (forceps + scissors/scalpel) is the gold standard
- Enzymatic debridement (e.g., collagenase ointment) can supplement for persistent slough
- Autolytic debridement occurs under moist dressings (slower but suitable for shallow wounds)
- Goal: a clean wound base with healthy granulation tissue
Step 3: Irrigation
- Irrigate with warm saline or clean water at low pressure
- Reduces bacterial load effectively
- Do NOT use hydrogen peroxide, povidone-iodine, or hypochlorite solutions in open wounds - these damage granulation tissue and delay healing
- Repeat irrigation at every dressing change
- Showering is equally effective and should be encouraged
Step 4: Dressing Selection by Wound Stage
| Wound Stage | Characteristics | Recommended Dressing |
|---|---|---|
| Infected / heavily exuding | Purulent discharge, slough | Saline-moistened gauze packing; silver-containing dressings (e.g. Aquacel Ag) |
| Sloughy / fibrinous | Yellow/brown devitalized tissue | Hydrogel (rehydrates and autolytically debrides) |
| Granulating | Red, beefy tissue forming | Foam dressing (absorbs exudate, non-adherent) |
| Epithelializing | Pink/white new skin at edges | Hydrocolloid or thin film dressing; keep moist |
| Deep cavity wounds | Wide, deep open wound | Alginate rope packing or NPWT |
Key dressing principles:
- Moist wound environment promotes faster re-epithelialization (vs. dry gauze)
- Non-adherent layers prevent trauma at dressing change
- Change frequency depends on exudate level - heavily exuding wounds: every 24-48 hrs; granulating wounds: every 2-3 days
Step 5: Antibiotics (if infected)
- Broad-spectrum coverage required - organisms can originate from skin, genitourinary tract, or GI tract
- Typical empirical regimen: amoxicillin-clavulanate OR cephalexin + metronidazole
- If MRSA suspected (hospital-acquired, prior MRSA): add trimethoprim-sulfamethoxazole or doxycycline
- Adjust based on culture results
- Duration: 5-7 days for superficial SSI; longer for deep infections
5. Negative Pressure Wound Therapy (NPWT / VAC)
NPWT uses continuous or intermittent negative pressure (up to -125 mmHg) through a sealed foam dressing to:
- Stimulate granulation tissue formation
- Reduce local oedema and tissue exudate
- Reduce bacterial load
- Draw wound edges together

Indications for NPWT in open C-section wounds:
- Large or deep wounds not amenable to simple packing
- Wounds with significant dead space
- Obese patients with pannus (particularly high risk for wound breakdown)
- Wounds failing to granulate with conventional dressing
NPWT in obese patients (prophylactic use): Some studies show benefit in high-risk patients (BMI >35), but a retrospective study of women with BMI ≥50 found no difference vs. standard wound care. Prophylactic NPWT is therefore not universally recommended and should be reserved for high-risk cases.
- Bailey and Love's Short Practice of Surgery 28e, p. 2851
- Creasy & Resnik's Maternal-Fetal Medicine, p. 4056
6. Closure Options
Secondary Intention (Healing Naturally)
- The wound is left open and granulates progressively from the base upward
- Suitable for small, shallow wounds or heavily infected wounds
- Requires daily dressing changes over weeks
- Results in wider scar but avoids re-infection risk
Delayed Primary Closure (DPC)
- Open packing for 3-5 days until wound is clean and granulating
- Then close the wound with sutures/staples
- Shown to significantly reduce wound infection rates and mean healing time
- Suitable for contaminated but not infected wounds once bacterial load is reduced
Secondary Closure (Late Suturing)
- After full granulation tissue has formed (weeks later)
- Used for larger wounds where simple DPC is not possible
- May require a minor procedure under local anesthesia
7. Monitoring and Follow-Up
| Timepoint | Assessment |
|---|---|
| Daily (inpatient) | Vital signs, wound inspection, dressing change, exudate amount/character |
| Every 3-5 days (outpatient) | Wound dimensions (length x width x depth), photograph wound progress |
| Weekly | Review culture results, adjust antibiotics, assess granulation progress |
| Red flags - escalate urgently | Spreading erythema >2 cm beyond wound edge, crepitus (gas gangrene/NF), systemic sepsis, fever >38.5°C, failure to improve at 2 weeks |
Necrotizing fasciitis must always be excluded in wounds that look disproportionately severe or where the patient is systemically unwell. It is a surgical emergency requiring aggressive debridement + broad-spectrum IV antibiotics (piperacillin-tazobactam + vancomycin).
8. Promoting Healing: General Measures
| Intervention | Rationale |
|---|---|
| Nutritional support | Protein 1.2-1.5 g/kg/day; Vitamin C and zinc support collagen synthesis |
| Glycaemic control | Target glucose <10 mmol/L; hyperglycaemia impairs phagocytosis |
| Anaemia correction | Haemoglobin >80 g/L for tissue oxygenation |
| Pressure relief | Avoid wound compression; encourage mobility |
| Breastfeeding/skin-to-skin | Promotes oxytocin-mediated uterine involution (reduces pelvic congestion) |
| Smoking cessation | Nicotine causes vasoconstriction and impairs wound healing |
9. Summary Table - Quick Reference
| Scenario | Management |
|---|---|
| Small seroma/hematoma, no infection | Observe; may reabsorb spontaneously |
| Superficial wound separation, clean | Irrigate + moist dressings + secondary intention |
| Infected wound | Open, culture, debride, irrigate, broad-spectrum antibiotics |
| Large/deep infected cavity | NPWT + antibiotics; DPC when clean |
| Fascial disruption | Surgical emergency - operative repair |
| Necrotizing fasciitis | Emergency debridement + ICU + IV broad-spectrum antibiotics |
Sources: Management of Wound Complications of Cesarean Delivery - Exxcellence | Creasy & Resnik's Maternal-Fetal Medicine, p. 3771, 4056 | Bailey and Love's Short Practice of Surgery 28e, p. 2841-2860 | Fischer's Mastery of Surgery 8e | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.