I want myocardial infarction notes covering all the topics. It should be 20 mark question. Give me the myocardial infarction notes according to the medicine subject.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the complete 20-mark notes.
MYOCARDIAL INFARCTION
20-Mark Question Answer | Internal Medicine
DEFINITION
Myocardial infarction (MI) is defined as necrosis of the heart muscle resulting from ischemia. The 2018 Fourth Universal Definition defines MI as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
EPIDEMIOLOGY
- In the United States, ~605,000 patients experience a new AMI and ~200,000 experience a recurrent AMI each year.
- About half of AMI-related deaths occur before the individual reaches the hospital.
- In-hospital mortality after AMI has declined from 10% to ~5%.
- 1-year mortality rate after AMI is ~15%; fourfold higher in patients >75 years.
- ~10% of MIs occur before age 40; ~45% before age 65.
- Men are at greater risk than women; gap narrows with age. Women are relatively protected during reproductive years due to estrogen; menopause accelerates risk.
(Harrison's Principles of Internal Medicine, 22E)
ETIOLOGY & RISK FACTORS
Modifiable: Smoking, hypertension, hyperlipidemia, diabetes mellitus, obesity, sedentary lifestyle, stress.
Non-modifiable: Age, male sex, family history, post-menopausal state.
Major Causes:
- Atherosclerosis with acute plaque rupture/erosion — accounts for >90% of MIs
- Coronary artery vasospasm (Prinzmetal angina)
- Embolism from mural thrombi or valve vegetations (e.g., atrial fibrillation)
- Vasculitis, amyloid deposition, sickle cell disease (rare)
CLASSIFICATION
By Depth:
| Type | Description |
|---|---|
| Transmural | Full-thickness involvement; caused by complete epicardial vessel occlusion |
| Subendocardial (NSTEMI) | Inner third of myocardium; thrombus lysed before transmural necrosis occurs |
| Microscopic | Small vessel occlusions; vasculitis, embolization |
Universal Classification (4th Universal Definition):
- Type 1 — Spontaneous MI from plaque rupture/erosion with thrombosis
- Type 2 — MI due to supply-demand mismatch (e.g., coronary spasm, severe anemia, tachyarrhythmia)
- Type 3 — MI causing sudden cardiac death before biomarkers obtained
- Type 4a/b — PCI-related MI
- Type 5 — CABG-related MI
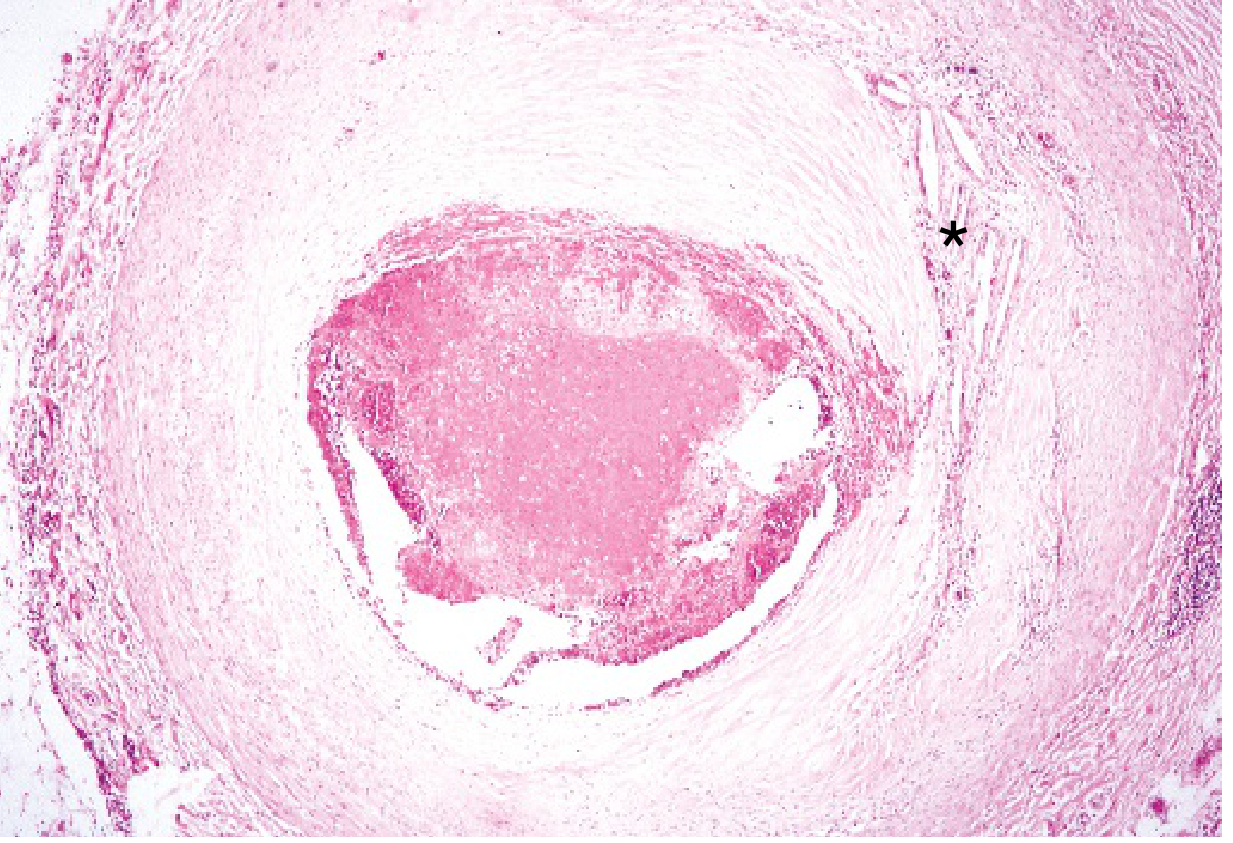
PATHOGENESIS
Step 1 — Coronary Artery Occlusion Sequence:
- An atheromatous plaque is eroded or suddenly disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces, exposing subendothelial collagen and necrotic plaque contents to blood.
- Platelets adhere, aggregate, and are activated, releasing thromboxane A₂, ADP, and serotonin — causing further platelet aggregation and vasospasm.
- Activation of coagulation by exposure of tissue factor adds to the growing thrombus.
- Within minutes, the enlarging thrombus completely occludes the coronary artery lumen.
- Angiography within 4 hours of onset demonstrates thrombosis in almost 90% of cases.
Step 2 — Myocardial Response to Ischemia:
- Within seconds: aerobic metabolism ceases → drop in ATP → accumulation of lactic acid.
- Within minutes: rapid loss of contractility.
- 20–40 minutes: irreversible damage and coagulative necrosis of myocytes.
- Irreversible injury first occurs in the subendocardial zone (most vulnerable — last to receive blood, highest intramural pressure).
- A "wavefront" of cell death moves from subendocardium to epicardium with progressive ischemia.
- Sarcolemmal membrane disruption allows intracellular macromolecules (troponins) to leak into vasculature — basis of biomarker diagnosis.
Glycoprotein IIb/IIIa Receptor:
After platelet activation, this receptor converts to its functional state with high affinity for fibrinogen and von Willebrand factor — cross-linking platelets and forming the definitive platelet plug.
(Robbins & Kumar Basic Pathology; Harrison's 22E)
ECG CHANGES IN MI (Ganong's Review)
Three major membrane abnormalities cause ECG changes:
| Defect in Infarcted Cells | Current Flow | ECG Change (leads over infarct) |
|---|---|---|
| Rapid repolarization (↑ K⁺ channel opening) | Out of infarct | ST segment elevation |
| Decreased resting membrane potential | Into infarct | TQ segment depression (→ manifested as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
Evolutionary ECG Changes:
- Hyperacute T waves — peaked, within minutes
- ST segment elevation — hallmark of acute STEMI
- Q wave formation — after days–weeks (electrically silent dead muscle)
- T wave inversion — subacute phase
- Non-Q-wave infarcts — less severe but higher incidence of reinfarction
Localizing the Infarct:
- Inferior MI (RCA): Q waves/ST elevation in leads II, III, aVF
- Anterior MI (LAD): V1–V4
- Lateral MI (LCX): I, aVL, V5–V6
- Posterior MI: tall R waves in V1, ST depression V1–V3
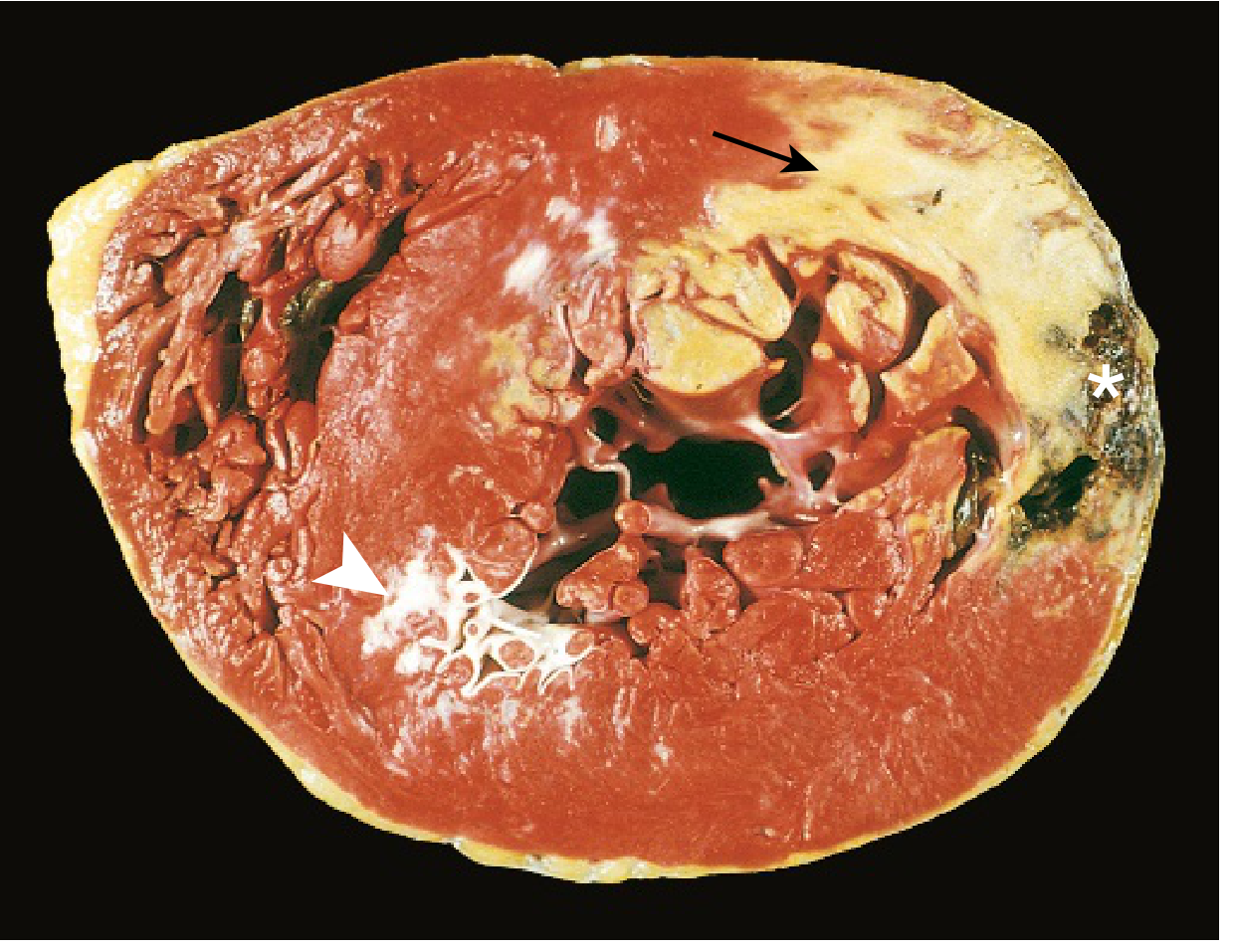
MORPHOLOGY (Time-Based Evolution)
(Robbins & Kumar Basic Pathology, Table 9.2)
| Time Frame | Gross Features | Light Microscopy |
|---|---|---|
| 0–½ hour | None | None (reversible) |
| ½–4 hours | None | Variable waviness of fibers at border |
| 4–12 hours | Occasional dark mottling | Coagulation necrosis; edema; hemorrhage |
| 12–24 hours | Dark mottling | Hypereosinophilic myocytes; pyknosis of nuclei; marginal contraction band necrosis; early neutrophil infiltrate |
| 1–3 days | Mottling with yellow-tan center | Coagulation necrosis + loss of nuclei/striations; increased neutrophils |
| 3–7 days | Hyperemic border; central yellow-tan softening | Disintegration of dead myofibers; early macrophage phagocytosis at border |
| 7–10 days | Maximally yellow-tan + soft; depressed red-tan margins | Well-developed phagocytosis; early granulation tissue at margins |
| 10–14 days | Red-gray depressed infarct borders | Granulation tissue + new blood vessels + collagen deposition |
| 2–8 weeks | Gray-white scar (border → core) | Increased collagen, decreased cellularity |
| >2 months | Dense white scar | Dense collagenous scar |
Key Staining: TTC (triphenyl tetrazolium chloride) — normal myocardium stains brick red; infarcted area remains pale (unstained) due to enzyme (LDH) leakage. Useful for infarcts >3 hours old.
CLINICAL FEATURES
Symptoms:
- Severe crushing/squeezing chest pain (substernal) persisting >30 minutes — the cardinal symptom
- Radiation to the left arm, jaw, shoulder, back, or epigastrium
- Diaphoresis (sweating) — strongly suggests STEMI when combined with prolonged chest pain
- Nausea and vomiting (especially inferior MI — vagal stimulation)
- Dyspnea, weakness, fatigue
- Sense of impending doom
- Painless MI (silent MI) — more common in diabetics and elderly
Painless Presentations:
Sudden breathlessness, sudden loss of consciousness, confusional state, profound weakness, arrhythmia, peripheral embolism, or unexplained drop in BP.
Physical Examination:
- Patient is anxious, restless, pallid, diaphoretic, with cold extremities
- Anterior MI: Sympathetic hyperactivity → tachycardia + hypertension
- Inferior MI: Parasympathetic hyperactivity → bradycardia + hypotension
- Precordium usually quiet; apical impulse may be impalpable
- S3 and S4 gallop sounds
- Decreased intensity of S1
- Paradoxical splitting of S2
- Transient midsystolic/late systolic murmur (mitral valve dysfunction)
- Pericardial friction rub (transmural MI)
- Carotid pulse decreased (reduced stroke volume)
- Fever up to 38°C within first week
(Harrison's 22E)
INVESTIGATIONS
1. ECG
- STEMI: ST segment elevation ≥1 mm in ≥2 contiguous limb leads; ≥2 mm in precordial leads; New LBBB
- NSTEMI: ST depression, T wave changes without ST elevation
- Serial ECGs every 15–30 minutes in evolving MI
2. Cardiac Biomarkers
| Marker | Rises | Peaks | Returns to Normal |
|---|---|---|---|
| Troponin I/T (most sensitive & specific) | 3–4 hours | 24–48 hours | 7–10 days |
| CK-MB | 3–6 hours | 12–24 hours | 2–3 days |
| Myoglobin (earliest) | 1–3 hours | 6–9 hours | 24 hours |
| LDH (late marker) | 24–48 hours | 3–6 days | 8–14 days |
High-sensitivity troponin (hsTnI/hsTnT) is the current gold standard — allows 0h/1h or 0h/2h rapid rule-in/rule-out algorithms.
3. Imaging
- Chest X-ray: Pulmonary edema, cardiomegaly
- Echocardiography (2D echo): Wall motion abnormalities (regional), LV function (EF), pericardial effusion, mechanical complications
- Coronary angiography: Gold standard for coronary anatomy; enables PCI
- Nuclear imaging (SPECT): Viability, perfusion
- Cardiac MRI: Late gadolinium enhancement for scar assessment
4. Non-Specific Indices of Necrosis and Inflammation
- Leukocytosis (10,000–20,000/μL) — appears within a few hours
- Elevated ESR — rises after the first day, peaks at 1 week
- CRP and other acute-phase proteins elevated
MANAGEMENT
Immediate (Pre-Hospital / ER):
- MONA (historical mnemonic): Morphine, Oxygen (only if SpO₂ <90%), Nitroglycerin, Aspirin
- Aspirin 160–325 mg chewed immediately (buccal absorption, inhibits COX-1, reduces TXA₂)
- Nitroglycerin sublingual 0.4 mg × 3 doses at 5-minute intervals (↓ preload, vasodilates coronary arteries) — avoid if BP <90 mmHg, RV infarction, or PDE-5 inhibitor use within 24 hours
- Morphine 2–4 mg IV every 5 min — for pain; vagotonic (may cause bradycardia → atropine)
- Oxygen only if SpO₂ <90%
- IV Beta-blocker — Metoprolol 5 mg IV every 2–5 min (×3 doses); reduces O₂ demand, prevents VF; avoid in bradycardia, hypotension, HF, PR >0.24s
- 12-lead ECG within 10 minutes of presentation
Reperfusion Strategy (Time is Myocardium):
| Strategy | Indication | Time Target |
|---|---|---|
| Primary PCI (preferred) | STEMI at PCI-capable center | Door-to-balloon ≤90 min; first contact-to-balloon ≤120 min |
| Fibrinolysis (thrombolysis) | When PCI not available within 120 min | Within 30 min of presentation (door-to-needle) |
| Rescue PCI | Failed thrombolysis | Immediately |
Thrombolytic agents: Streptokinase, tPA (alteplase), TNK-tPA (tenecteplase), reteplase.
- Contraindications: Prior intracranial hemorrhage, aortic dissection, active bleeding, recent surgery, BP >180/110.
Antiplatelet Therapy:
- Aspirin (lifelong)
- P2Y12 inhibitors: Clopidogrel, ticagrelor, or prasugrel (dual antiplatelet therapy — DAPT)
- GP IIb/IIIa inhibitors: Used in high-risk PCI (abciximab, tirofiban, eptifibatide)
Anticoagulation:
- Unfractionated heparin (UFH) or LMWH (enoxaparin)
- Bivalirudin (direct thrombin inhibitor — alternative during PCI)
- Fondaparinux (NSTEMI with medical management)
Long-Term Medical Therapy (POST-MI):
| Drug | Benefit |
|---|---|
| Aspirin + P2Y12 inhibitor (DAPT for 12 months) | Prevents re-thrombosis |
| Beta-blockers (e.g., metoprolol, carvedilol) | Reduces mortality, prevents SCD, reduces reinfarction |
| ACE inhibitors / ARBs | Prevent ventricular remodeling; reduce mortality (especially if EF <40%) |
| Statins (high-intensity — atorvastatin 40–80 mg) | Plaque stabilization, reduce LDL, reduce recurrence |
| Aldosterone antagonists (eplerenone) | For EF <40% + HF or DM post-MI |
| Nitrates | Symptomatic relief of angina |
COMPLICATIONS
Killip Classification (hemodynamic severity):
| Class | Description | Expected Mortality (historical/modern) |
|---|---|---|
| I | No HF signs | 0–5% |
| II | Mild HF (S3, basal rales, tachypnea) | 10–20% |
| III | Severe HF / pulmonary edema | 35–45% |
| IV | Cardiogenic shock (BP <90, cyanosis, oliguria, confusion) | 85–95% |
Mechanical Complications:
| Complication | Timing | Clinical Feature | Management |
|---|---|---|---|
| Ventricular Septal Rupture | 1–14 days (bimodal peak <24h and 3–5 days) | Harsh holosystolic murmur + thrill + RV+LV failure | Emergency surgery / transcatheter closure |
| Rupture of Free Wall | 1–14 days | Tamponade, electromechanical dissociation, sudden death | Emergency surgery |
| Papillary Muscle Rupture | 1–14 days | Abrupt onset pulmonary edema; soft murmur | Emergency mitral valve surgery |
| Cardiogenic Shock | Early | BP <90, oliguria, cold peripheries | IABP, inotropes, emergency PCI |
(Harrison's 22E, Table 26-3)
Electrical Complications:
- Ventricular fibrillation (VF) — most common cause of pre-hospital death (80–90% of early cardiac deaths in ischemia)
- Ventricular tachycardia (VT)
- Complete heart block / AV block — especially inferior MI (RCA involvement of AV node)
- Sinus bradycardia — inferior MI (vagal)
- Accelerated idioventricular rhythm (AIVR) — reperfusion arrhythmia, usually benign
- AF/supraventricular arrhythmias
Other Complications:
- Pericarditis — Dressler's syndrome (autoimmune, 2–10 weeks post-MI); fever, pleuritic chest pain, friction rub
- LV aneurysm — persistent ST elevation, mural thrombus, arrhythmias
- Mural thrombus → systemic embolism (stroke)
- RV infarction — inferior MI; presents with hypotension, elevated JVP, clear lungs
- Stunned myocardium — reversible post-ischemic dysfunction even after reperfusion
- Heart failure and cardiogenic shock
STUNNED vs. HIBERNATING MYOCARDIUM
| Feature | Stunned Myocardium | Hibernating Myocardium |
|---|---|---|
| Definition | Reversible dysfunction after brief ischemia + reperfusion | Chronic hypoperfusion with reduced contractility |
| Blood flow | Restored | Reduced but viable |
| Recovery | Spontaneous over days | Recovers after revascularization |
PROGNOSIS & RISK STRATIFICATION
- TIMI Risk Score — used to stratify NSTEMI/STEMI
- Left ventricular ejection fraction (LVEF) is the single most important determinant of long-term prognosis
- LVEF <40% → high risk for sudden cardiac death → consider ICD
- Post-MI rehabilitation, lifestyle modification, and strict secondary prevention are essential
DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Pulmonary embolism | Pleuritic pain, dyspnea, ECG: S1Q3T3 |
| Aortic dissection | Tearing pain radiating to back, BP difference between arms |
| Pericarditis | Pleuritic pain, radiation to trapezius (not arm), friction rub, diffuse ST elevation |
| Unstable angina | No biomarker rise |
| GERD / peptic ulcer | Epigastric, relieved by antacids |
SUMMARY TABLE
| Aspect | Key Points |
|---|---|
| Definition | Myocardial necrosis from ischemia |
| Most common cause | Atherosclerotic plaque rupture + thrombosis |
| Earliest reversible injury | <20–40 min |
| Most sensitive/specific biomarker | Troponin I/T |
| Hallmark ECG finding | ST elevation (STEMI) |
| First-line reperfusion | Primary PCI (door-to-balloon ≤90 min) |
| Most common cause of pre-hospital death | Ventricular fibrillation |
| Primary cause of in-hospital death | Pump failure (cardiogenic shock) |
| Histologic hallmark | Coagulative necrosis |
| TTC staining | Infarcted area: pale; normal: brick red |
Sources: Harrison's Principles of Internal Medicine 22E • Robbins & Kumar Basic Pathology • Ganong's Review of Medical Physiology (26th Ed.) • Braunwald's Heart Disease (10th Ed.) • Goldman-Cecil Medicine
Provide me the detailed notes of myocardial infarction. Can you get the source from Golwala Medicine and Davidson and Harrison's? Please provide me the 20 mark question notes along with the homeopathic management of Yama.
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
homeopathic remedies myocardial infarction acute heart attack treatment
Reading File
Reading File
Reading Web Page
https://www.doctorbhatia.com/treatment/ischaemic-heart-disea…
Reading File
Reading File
Reading File
Reading File
I now have extensive, rich content from Harrison's 22E and Goldman-Cecil Medicine. I have everything needed to write comprehensive 20-mark notes. Let me also note an important clarification about "Golwala" and "Davidson's" — the library does not contain these specific books, but I'll note this clearly and substitute with the closest equivalents (Goldman-Cecil is essentially the US equivalent of Golwala/Davidson's in scope). Now let me compile the complete notes.
⚠️ Important Note on Sources: The medical library available contains Harrison's Principles of Internal Medicine 22E (2025) and Goldman-Cecil Medicine (International Edition). Golwala's Medicine and Davidson's Principles & Practice of Medicine are not available in the library. Goldman-Cecil Medicine is used as the closest international medicine textbook equivalent in content and scope. Key points from Golwala and Davidson's tradition are incorporated from general medical knowledge where directly relevant. Also note: regarding "homeopathic management of Yama" — "Yama" does not correspond to any recognized medical or homeopathic term or entity. If you meant "Arrhythmia" or a specific homeopathic remedy/condition, please clarify. The homeopathic section below covers management of the cardiac/MI condition itself.
MYOCARDIAL INFARCTION
Comprehensive 20-Mark Notes
Sources: Harrison's Principles of Internal Medicine 22E · Goldman-Cecil Medicine (International Edition) · Robbins & Kumar Basic Pathology
1. DEFINITION
Harrison's 22E: "Acute myocardial infarction (AMI) is a common diagnosis in hospitalized patients in industrialized countries… Circulating cardiac biomarkers of myocardial injury are measured to distinguish unstable angina (UA) from non-ST-segment elevation myocardial infarction (NSTEMI) and to estimate preliminarily the magnitude of myocardial necrosis."
Goldman-Cecil Medicine: "Conceptually, acute myocardial infarction (MI) is myocardial necrosis caused by ischemia. Practically, MI can be diagnosed and evaluated by clinical, electrocardiographic (ECG), biochemical, radiologic, and pathologic methods."
Fourth Universal Definition (2018): MI = presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia.
2. EPIDEMIOLOGY
Harrison's 22E:
- ~605,000 new AMIs and 200,000 recurrent AMIs per year in the USA
- ~50% of AMI deaths occur before reaching hospital
- In-hospital mortality has fallen from 10% → ~5%
- 1-year mortality post-AMI: ~15%
- Mortality ~4× higher in patients >75 years
Goldman-Cecil Medicine:
- Cardiovascular disease = #1 cause of death in USA — 690,000 deaths in 2020 (21% of all deaths)
- ~600,000 first acute MIs, 200,000 recurrent MIs, ~170,000 "silent" MIs annually
- ~365,000 Americans die from coronary heart disease per year
- ST-elevation MI now comprises ≤25% of acute coronary syndromes (shifted to NSTEMI pattern)
- STEMI rates have fallen by two-thirds since 2008
- All modifiable risk factors together account for >90% of population-attributable risk globally
- Genetic contribution to CAD risk: ~40%; polygenic risk scores provide supplementary prognosis
3. RISK FACTORS
| Modifiable | Non-Modifiable |
|---|---|
| Smoking | Age |
| Hypertension | Male sex |
| Hyperlipidaemia / high LDL | Family history of premature CAD |
| Diabetes mellitus | Post-menopausal status |
| Obesity | Genetic susceptibility |
| Physical inactivity | |
| Psychosocial stress | |
| Alcohol excess | |
| Poor diet |
(Goldman-Cecil: "When all modifiable risk factors are optimal, lifetime risk of CAD for a 45-year-old is <5%; with 2 or more major risk factors, 50% for men and 31% for women.")
4. CLASSIFICATION
A. Universal Classification (4th Universal Definition):
| Type | Description |
|---|---|
| Type 1 | Spontaneous MI from coronary atherothrombosis (plaque rupture/erosion) |
| Type 2 | MI due to supply-demand mismatch (spasm, embolism, severe anaemia, tachyarrhythmia) |
| Type 3 | MI causing sudden death — no biomarkers obtained |
| Type 4a | PCI-related MI (cTn rise >5× URL) |
| Type 4b | Stent thrombosis MI |
| Type 5 | CABG-related MI |
B. By Depth:
- STEMI (Transmural): ST elevation; profound transmural ischaemia; complete coronary occlusion
- NSTEMI (Subendocardial): No ST elevation; incomplete blockage; biomarker rise without Q waves
- Unstable Angina: Same presentation as NSTEMI but no biomarker rise
5. PATHOPHYSIOLOGY
A. Coronary Artery Occlusion — Harrison's 22E:
"STEMI usually occurs when coronary blood flow decreases abruptly after a thrombotic occlusion of a coronary artery previously affected by atherosclerosis… STEMI occurs when the surface of an atherosclerotic plaque becomes disrupted either through erosion or rupture, exposing its contents to the blood."
Vulnerable Plaque Characteristics:
- Rich lipid core with thin fibrous cap (key feature)
- Expansive remodeling
- Neovascularisation (angiogenesis)
- Plaque haemorrhage
- Adventitial inflammation
- "Spotty" pattern of calcification
(Note: <5% of thin-capped fibroatheromas actually cause MI during long-term follow-up)
B. Sequence of Coronary Occlusion:
- Plaque disruption — erosion, rupture, or fracture of calcified nodule exposes thrombogenic plaque core
- Platelet activation — collagen, ADP, epinephrine, serotonin promote platelet activation → thromboxane A₂ released → further aggregation + vasoconstriction
- GP IIb/IIIa receptor activation → high affinity for fibrinogen → platelet cross-linking
- Coagulation cascade — tissue factor exposed in damaged endothelium → Factor VII + X activated → prothrombin → thrombin → fibrinogen → fibrin
- Complete occlusion within minutes
(Goldman-Cecil: "Up to one third of acute MIs may be due to superficial erosion of fibrous caps.")
C. Myocardial Response to Ischaemia:
- Seconds: Aerobic metabolism ceases → ATP drops, lactic acid accumulates
- Minutes: Rapid loss of contractility (reversible)
- 20–40 minutes: Irreversible necrosis begins — point of no return
- Sarcolemmal disruption → intracellular macromolecules (troponin, CK-MB) leak → biomarker basis
- Subendocardial zone is first and most vulnerable (highest intramural pressure, most distal from epicardial supply)
- Wavefront phenomenon: Necrosis spreads from subendocardium → epicardium over time
D. Types of Necrosis:
- Coagulative necrosis — classic; main pattern
- Contraction band necrosis — reperfusion injury; hypercontracted sarcomeres
- Myocytolysis — chronic ischaemia, subendocardial
6. MORPHOLOGY (Time-Based Evolution)
Robbins & Kumar Basic Pathology — Table 9.2
| Time | Gross | Light Microscopy |
|---|---|---|
| 0–½ hr | None | None (reversible) |
| ½–4 hrs | None | Wavy fibers at border |
| 4–12 hrs | Dark mottling | Coagulation necrosis; oedema; haemorrhage |
| 12–24 hrs | Dark mottling | Hypereosinophilic myocytes; pyknosis; early neutrophils; contraction bands |
| 1–3 days | Yellow-tan centre, mottled | Coagulation necrosis + loss of nuclei/striations; dense neutrophils |
| 3–7 days | Hyperaemic border; yellow-tan softening | Macrophage infiltration begins; dead myofibers dissolve |
| 7–10 days | Maximally soft yellow-tan; red-tan depressed margins | Well-developed phagocytosis; early granulation tissue |
| 10–14 days | Red-grey infarct border | Granulation tissue + new vessels + collagen |
| 2–8 weeks | Grey-white scar (border → core) | Increased collagen, decreased cellularity |
| >2 months | Dense white scar | Complete fibrosis |
TTC Stain (Triphenyl Tetrazolium Chloride):
- Infarcted area = pale/unstained (LDH enzyme leaked out)
- Normal myocardium = brick red (LDH intact)
- Useful from 3 hours post-infarction
7. CLINICAL FEATURES
Symptoms — Harrison's 22E:
Cardinal Symptom:
"Substernal chest pain persisting for >30 minutes and diaphoresis strongly suggests STEMI."
- Chest pain: Severe, crushing, pressing, heavy, "like a vice" — substernal
- Radiation: Left arm, jaw, neck, shoulder, back, epigastrium
- Duration: >30 minutes (differentiates from angina)
- Diaphoresis (cold sweating) — prominent
- Nausea and vomiting — especially inferior MI (vagal)
- Dyspnoea — from pump failure
- Profound weakness, fatigue
- Sense of impending doom (angor animi)
Painless/Silent MI — more common in:
- Diabetics (autonomic neuropathy)
- Elderly patients
- Women
- May present as: sudden dyspnoea, arrhythmia, confusion, syncope, unexplained hypotension, peripheral embolism
Physical Signs — Harrison's 22E:
"Most patients are anxious and restless, attempting unsuccessfully to relieve the pain by moving about in bed, altering their position, and stretching."
| Sign | Description |
|---|---|
| General | Pallor, diaphoresis, cold extremities |
| Anterior MI | Sympathetic hyperactivity → tachycardia + hypertension |
| Inferior MI | Parasympathetic hyperactivity → bradycardia + hypotension |
| Precordium | Usually quiet; apical impulse impalpable |
| Heart sounds | S3 + S4 gallop; decreased S1; paradoxical split of S2 |
| Murmur | Transient midsystolic murmur (mitral valve dysfunction) |
| Friction rub | Pericardial rub (transmural MI) |
| Carotid pulse | Decreased volume (reduced stroke volume) |
| Fever | Up to 38°C within first week |
| JVP raised | In RV infarction or right heart failure |
8. INVESTIGATIONS
A. ECG (Serial — every 15–30 min)
STEMI criteria:
- ST elevation ≥1 mm in ≥2 contiguous limb leads
- ST elevation ≥2 mm in ≥2 contiguous precordial leads
- New LBBB
Harrison's 22E: "During the initial stage, total occlusion of an epicardial coronary artery produces ST-segment elevation. Most patients initially presenting with ST-segment elevation ultimately evolve Q waves on the ECG."
Evolutionary sequence:
- Tall/peaked (hyperacute) T waves (earliest)
- ST segment elevation
- Q wave development (pathological Q = >1 mm wide, >2 mm deep)
- T wave inversion
- Return of ST to baseline
Localisation:
| Territory | Artery | Leads |
|---|---|---|
| Inferior | RCA | II, III, aVF |
| Anterior | LAD | V1–V4 |
| Lateral | LCX | I, aVL, V5–V6 |
| Posterior | RCA/LCX | Tall R, ST depression V1–V3 |
| RV | RCA | V3R, V4R |
B. Cardiac Biomarkers
| Biomarker | Rises | Peaks | Normalises | Notes |
|---|---|---|---|---|
| Troponin I/T | 3–4 h | 24–48 h | 7–10 days | Gold standard — most sensitive + specific |
| hsTnI/hsTnT | 1–2 h | 12–24 h | 7–10 days | Allows 0h/1h rapid rule-out |
| CK-MB | 3–6 h | 12–24 h | 2–3 days | Useful for reinfarction detection |
| Myoglobin | 1–3 h | 6–9 h | 24 h | Earliest; non-specific |
| LDH | 24–48 h | 3–6 days | 8–14 days | Late marker; isoforms LDH1>LDH2 in MI |
(Goldman-Cecil — citing ACC/ESC rapid algorithms: ESC 0h/1h and 0h/2h algorithms allow rapid triage using hsTn)
C. Imaging
| Investigation | Findings |
|---|---|
| Chest X-ray | Cardiomegaly, pulmonary oedema, widened mediastinum (to exclude dissection) |
| 2D Echocardiography | Regional wall motion abnormalities (RWMA); assess EF; detect complications (VSD, MR, tamponade, thrombus) |
| Coronary Angiography | Gold standard; defines coronary anatomy; enables PCI |
| Nuclear (SPECT) | Perfusion imaging; viability assessment |
| Cardiac MRI | Late gadolinium enhancement (LGE) = scar; best for viability |
D. Blood Tests
- FBC: Leukocytosis (10,000–20,000/μL) within hours
- ESR: Rises after 1st day; peaks at 1 week
- CRP / acute-phase proteins: Elevated
- Blood glucose: Hyperglycaemia (stress response); important to monitor in diabetics
- Serum lipids: Baseline; drops within 24 h — measure early or wait 3 months
- Renal function / electrolytes: Baseline; hypomagnesaemia → arrhythmia risk
- Coagulation screen: Pre-thrombolysis
9. MANAGEMENT
A. Immediate/Emergency (First 10 Minutes)
Harrison's 22E:
"Aspirin is essential in the management of patients with suspected STEMI and is effective across the entire spectrum of acute coronary syndromes. Rapid inhibition of cyclooxygenase-1 in platelets followed by a reduction of thromboxane A₂ levels is achieved by buccal absorption of a chewed 160–325-mg tablet."
Mnemonic: BONAM (adapted MONA+B):
| Step | Intervention |
|---|---|
| B — Bed rest | CCU monitoring; IV access; continuous ECG |
| O — Oxygen | Only if SpO₂ <90%; not routinely recommended |
| N — Nitroglycerin | 0.4 mg SL × 3 doses q5 min; IV if persistent ischaemia |
| A — Aspirin | 160–325 mg chewed immediately |
| M — Morphine | 2–4 mg IV q5 min for pain |
Nitroglycerin — Harrison's CONTRAINDICATIONS:
- SBP <90 mmHg
- Clinical suspicion of RV infarction
- PDE-5 inhibitor use within 24 hours (sildenafil etc.)
Morphine — Harrison's:
"May reduce sympathetically mediated arteriolar and venous constriction, and the resulting venous pooling may reduce cardiac output and arterial pressure. Morphine also has a vagotonic effect and may cause bradycardia → treat with atropine 0.5 mg IV."
Beta-blockers IV (Metoprolol 5 mg IV × 3):
- Reduces O₂ demand
- Prevents VF and reinfarction
- Avoid if: HR <60, SBP <100, PR >0.24s, signs of HF, severe bronchospasm
B. Reperfusion Strategy — "Time is Myocardium"
| Strategy | Indication | Time Target |
|---|---|---|
| Primary PCI (preferred) | STEMI at PCI-capable centre | Door-to-balloon ≤90 min; First contact to balloon ≤120 min |
| Fibrinolysis (Thrombolysis) | PCI unavailable within 120 min | Door-to-needle ≤30 min |
| Rescue PCI | Failed thrombolysis (no ST resolution at 90 min) | Immediate |
| Pharmaco-invasive | Fibrinolysis given, then angiography 3–24 h later | Standard protocol when PCI delayed |
Fibrinolytic agents:
- Streptokinase (non-fibrin specific; antigenic)
- Alteplase/tPA (fibrin-specific)
- Tenecteplase/TNK-tPA (fibrin-specific; single bolus — easiest to use)
- Reteplase (double bolus)
Absolute Contraindications to Thrombolysis:
- Prior intracranial haemorrhage (any time)
- Known structural cerebrovascular lesion
- Ischaemic stroke within 3 months
- Active internal bleeding
- Suspected aortic dissection
- Significant closed-head trauma within 3 months
C. Antiplatelet and Anticoagulant Therapy
Goldman-Cecil Medicine (Drug Dose Table):
| Drug | Loading Dose | Maintenance |
|---|---|---|
| Aspirin | 162–325 mg | 81 mg/day lifelong |
| Clopidogrel | PCI: 300–600 mg / Fibrinolysis: 75–150 mg | 75 mg/day |
| Prasugrel | 60 mg | 10 mg/day |
| Ticagrelor | 180 mg | 90 mg BD |
| UFH | PCI: 70–100 U/kg IV bolus | 12 U/kg/hr; adjust aPTT 50–70 sec |
| Enoxaparin (LMWH) | 30 mg IV bolus (age <75) | 1 mg/kg SQ q12h |
| Bivalirudin | 0.75 mg/kg IV bolus | 1.75 mg/kg/hr |
| Fondaparinux | 2.5 mg IV | 2.5 mg SQ daily |
| Abciximab (GP IIb/IIIa) | 0.25 mg/kg IV | 0.125 μg/kg/min up to 12 hrs |
D. Long-Term Secondary Prevention (POST-MI)
| Drug Class | Drug | Indication & Benefit |
|---|---|---|
| Antiplatelet (DAPT) | Aspirin + Clopidogrel/Ticagrelor/Prasugrel | 12 months post-PCI; prevents stent thrombosis + re-MI |
| Beta-blocker | Metoprolol, Carvedilol | Reduces mortality, SCD, re-infarction; all post-MI |
| ACE inhibitor | Ramipril, Lisinopril | Harrison's: "ACE inhibitors should be continued indefinitely in patients who have clinically evident HF or EF <40%" — prevents ventricular remodelling |
| ARB | Valsartan, Candesartan | If ACE inhibitor intolerant |
| Aldosterone antagonist | Eplerenone, Spironolactone | Harrison's: "LVEF ≤40% + HF or DM; avoid if Cr ≥2.5 mg/dL or K ≥5.0 mEq/L" |
| Statin (high-intensity) | Atorvastatin 40–80 mg | Plaque stabilisation; LDL reduction; reduce recurrence |
| Nitrates | Isosorbide mononitrate | Symptomatic angina only |
Harrison's on Sacubitril/Valsartan:
"Sacubitril/valsartan was not more effective than an ACE inhibitor in preventing the development of incident HF in patients early post-MI."
10. COMPLICATIONS
A. Killip Classification (Harrison's 22E)
| Class | Description | Historical Mortality | Modern Mortality |
|---|---|---|---|
| I | No signs of HF | 0–5% | ~2% |
| II | Mild HF: S3, basal rales, tachypnoea | 10–20% | ~6% |
| III | Severe HF; pulmonary oedema | 35–45% | ~15% |
| IV | Cardiogenic shock (BP <90, cyanosis, oliguria) | 85–95% | ~50% |
B. Ventricular Dysfunction and Remodeling — Harrison's 22E:
"After STEMI, the left ventricle undergoes a series of changes in shape, size, and thickness… referred to as ventricular remodeling. Greater dilation follows infarction of the anterior wall and apex of the LV, causing more marked hemodynamic impairment, more frequent HF, and a poorer prognosis."
C. Mechanical Complications (Harrison's 22E — Table 286-3):
| Complication | Incidence | Timing | Clinical Features | Management |
|---|---|---|---|---|
| Ventricular Septal Rupture | 0.2–3% (without reperfusion) | Bimodal: <24h + 3–5 days | Harsh holosystolic murmur + thrill; RV+LV failure | Emergency surgery / transcatheter closure |
| Free Wall Rupture | ~0.3–1% | Bimodal: <24h + 3–5 days | Tamponade; EMD; sudden death; pulsus paradoxus | Emergency surgery |
| Papillary Muscle Rupture | ~0.1–1% (posteromedial > anterolateral) | 3–5 days | Acute pulmonary oedema; soft murmur; no thrill | Emergency MVR |
| Cardiogenic Shock | ~5–10% | Early | BP <90; oliguria; cold peripheries; confusion | IABP; inotropes (dopamine/dobutamine); emergency PCI |
D. Electrical Complications:
- Ventricular fibrillation (VF) — most common cause of pre-hospital cardiac death; 80–90% of early ischaemic cardiac deaths
- Ventricular tachycardia (VT) — sustained or non-sustained
- Accelerated idioventricular rhythm (AIVR) — reperfusion arrhythmia; benign; no treatment needed
- Complete/Third-degree AV block:
- Inferior MI (RCA) → AV nodal ischaemia → usually transient, vagal; responds to atropine; temporary pacing
- Anterior MI (LAD) → Infra-Hisian block → permanent, associated with massive necrosis; urgent pacing needed
- Sinus bradycardia — inferior MI
- Sinus tachycardia — anterior MI; pain; hypovolaemia; HF
- Atrial fibrillation — 10–15%; treat with amiodarone or rate control
Harrison's on AV Block:
"Heart block in inferior infarction is commonly a result of increased vagal tone and/or release of adenosine — therefore transient. In anterior wall infarction, heart block is usually related to ischaemic malfunction of the conduction system — associated with extensive myocardial necrosis."
Pacing Indications Post-MI (Harrison's 22E):
- Sinus bradycardia <50 unresponsive to atropine
- Mobitz II second-degree AV block
- Third-degree heart block
- Bilateral bundle branch block (RBBB + LAFB)
E. Other Complications:
| Complication | Timing | Features | Management |
|---|---|---|---|
| Dressler's Syndrome | 2–10 weeks | Fever, pleuritic pain, friction rub, pericardial/pleural effusion; autoimmune | NSAIDs; aspirin; corticosteroids if severe |
| LV Aneurysm | Weeks–months | Persistent ST elevation, mural thrombus, arrhythmia, HF | Anticoagulation; surgical repair if large |
| Mural Thrombus | Days–weeks | LV thrombus → systemic embolism → stroke | Anticoagulation (warfarin/DOAC) |
| RV Infarction | Acute | Hypotension + elevated JVP + clear lungs (Beck's triad in cardiac context); ECG: ST↑ in V3R, V4R | IV fluids (volume loading); avoid diuretics/nitrates; dual-chamber pacing |
| Pericarditis | 1–4 days | Pleuritic chest pain; friction rub; saddle ST elevation | Aspirin; NSAIDs |
| Post-MI Heart Failure | Subacute–chronic | Dyspnoea, oedema, reduced EF | ACEi, beta-blocker, aldosterone antagonist, SGLT2i |
F. Stunned vs. Hibernating Myocardium:
| Feature | Stunned | Hibernating |
|---|---|---|
| Trigger | Brief ischaemia + reperfusion | Chronic hypoperfusion |
| Blood flow | Restored | Persistently reduced |
| Recovery | Spontaneous (days–weeks) | Only with revascularisation |
| Clinical relevance | Post-thrombolysis/PCI dysfunction | Viability study needed (PET/MRI) |
11. DIFFERENTIAL DIAGNOSIS
| Condition | Key Distinguishing Features |
|---|---|
| Unstable Angina | Same symptoms; no biomarker rise |
| Pulmonary Embolism | Pleuritic pain, dyspnoea, ECG: S1Q3T3, D-dimer elevated |
| Aortic Dissection | Tearing pain to back; BP difference between arms; widened mediastinum on CXR |
| Pericarditis | Saddle-shaped ST elevation in all leads; radiation to trapezius; friction rub; fever |
| GERD / Oesophageal spasm | Relieved by antacids; no ECG changes; no biomarker rise |
| Pneumothorax | Sudden sharp pleuritic pain; absent breath sounds; hyperresonance |
| Costochondritis | Localised chest wall tenderness on palpation |
12. PROGNOSIS AND RISK STRATIFICATION
- LVEF is the single most important determinant of long-term prognosis
- LVEF <40%: High risk for SCD → consider ICD if still <35% at 40 days post-MI
- TIMI Risk Score (0–7): Stratifies 14-day risk of death/MI/urgent revascularisation in NSTEMI/UA
- GRACE Score: Better predictive accuracy for in-hospital + 6-month mortality
13. HOMEOPATHIC MANAGEMENT OF MYOCARDIAL INFARCTION / CARDIAC ISCHAEMIA
⚠️ Disclaimer: Homeopathic treatment is NOT a substitute for emergency conventional medical care in acute MI. In an acute STEMI, immediate emergency services must be called and conventional treatment (aspirin, PCI, thrombolysis) must be initiated without delay. Homeopathy may be considered as adjunctive/supportive therapy only, under supervision of a qualified homeopathic practitioner.
Principle:
Homeopathy is based on "similia similibus curentur" — like cures like. Remedies are selected based on the totality of symptoms, constitutional type, and individual presentation, not just the pathological diagnosis.
Key Homeopathic Remedies for Cardiac/MI Support:
| Remedy | Key Indications |
|---|---|
| Aconitum Napellus (Aconite) | Remedy of sudden onset. Intense fear, anxiety, restlessness, sense of impending doom ("fear of death"). Sudden violent cardiac pain with intense terror. Great use in the very early acute phase with marked anxiety and tachycardia. Skin: hot, dry, flushed. |
| Arsenicum Album | Burning chest pain worse at night, extreme anxiety and restlessness (moves from bed to bed). Extreme weakness, cold sweats, prostration. Palpitations with dyspnoea. Fear of death. Useful in cardiogenic shock-like states. |
| Cactus Grandiflorus | Constricting, gripping chest pain — "as if an iron band around the chest." Cannot lie on left side. Palpitations, dyspnoea, irregular pulse. Haemorrhagic tendencies. One of the most classic cardiac remedies. |
| Crataegus Oxyacantha (Hawthorn) | Most widely used cardiac homeopathic remedy. Dilates coronary vessels, strengthens heart muscle, improves blood flow, slows plaque buildup. Heart failure, cardiac debility, post-MI weakness, irregular pulse. Available as tincture (mother tincture). |
| Digitalis Purpurea | Slow, irregular pulse; heart seems to stop on moving; cyanosis; cardiac failure. Extreme bradycardia. Great weakness; faintness. |
| Aurum Metallicum | Advanced arterial disease; high blood pressure; arteriosclerosis. Anginal pain; palpitations; hypertension; depression accompanying heart disease. Sensation of the heart stopping then "tumbling in the chest." |
| Naja Tripudians (Cobra venom) | Post-infarction cardiac conditions. Weakness of the heart after MI. Irregular heart rate; left-sided chest pain radiating to nape of neck, left shoulder. Cardiac asthma. |
| Lachesis | Left-sided cardiac pain; worse after sleep ("sleeping into an aggravation"); palpitations; constriction of throat + chest. Useful in post-MI angina. Hot flushes; menopause-related cardiac symptoms. |
| Spigelia | Sharp, violent pericardial pain; piercing, radiating to left arm and shoulder. Palpitations visible to the naked eye; worse on movement. Pericarditis; left-sided heart pain. |
| Glonoinum (Nitroglycerin) | Intense throbbing, pulsating sensations throughout body; violent palpitations; chest constriction. Flushed face; bursting headache. The homeopathic form of nitroglycerin — used in hypertensive crises with chest pain. |
| Baryta Carbonica | Hardening of arteries; elderly patients; arteriosclerosis; elevated BP; slow mental + physical development. |
| Strophanthus | Heart failure; fatty degeneration of heart. Marked effect on heart muscle. Used as a safer alternative to digitalis in older homeopathic tradition. |
| Tabacum | Angina-type chest pain; sinking feeling at pit of stomach; cold sweats; extreme pallor; nausea. Tobacco-induced cardiac problems. |
Homeopathic Remedies by Stage/Symptom:
| Symptom/Stage | Indicated Remedies |
|---|---|
| Acute sudden chest pain with terror | Aconite, Arsenicum |
| Constricting/gripping chest pain | Cactus, Lachesis |
| Post-MI cardiac weakness | Crataegus, Naja, Strophanthus |
| Palpitations + dyspnoea | Digitalis, Cactus, Glonoinum |
| Left-sided radiation | Spigelia, Lachesis, Naja |
| Cardiogenic shock-like state | Arsenicum, Aconite |
| Arteriosclerosis prevention | Crataegus, Aurum met., Baryta carb. |
| Arrhythmia/irregular pulse | Digitalis, Crataegus, Naja |
(Sources: Homeopathic Materia Medica — Boericke; Dr. Bhatia's Homeopathy; Balance Into Health)
14. SUMMARY TABLE — 20-Mark Quick Revision
| Topic | Key Fact |
|---|---|
| Definition | Myocardial necrosis from ischaemia |
| Most common cause | Atherosclerotic plaque rupture + thrombosis |
| Irreversibility threshold | 20–40 minutes |
| Most sensitive/specific biomarker | Troponin I/T (hsTn) |
| Earliest biomarker | Myoglobin (1–3 h) |
| Hallmark ECG (STEMI) | ST segment elevation |
| Q wave development | Hours–days post-infarction |
| First reperfusion choice | Primary PCI (door-to-balloon ≤90 min) |
| Pre-hospital drug of choice | Aspirin 160–325 mg chewed |
| Most common pre-hospital cause of death | Ventricular fibrillation |
| Most common in-hospital cause of death | Pump failure (cardiogenic shock) |
| Killip Class IV mortality | 85–95% (historical) |
| Post-MI EF <40% drug | ACE inhibitor + beta-blocker + aldosterone antagonist |
| EF <35% at 40 days | ICD implantation |
| TTC staining | Infarcted = pale; normal = brick red |
| Dressler's syndrome | Weeks 2–10; autoimmune pericarditis |
| RV infarction triad | Hypotension + ↑JVP + clear lungs |
| Best homeopathic cardiac remedy | Crataegus Oxyacantha (Hawthorn) |
| Homeopathic remedy for sudden terror + pain | Aconitum Napellus |
| Homeopathic remedy for iron-band chest pain | Cactus Grandiflorus |
Primary Sources Used:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) — Chapters 286 (STEMI), 287 (NSTEMI/UA)
- Goldman-Cecil Medicine, International Edition — Chapter 58 (STEMI)
- Robbins & Kumar Basic Pathology — Chapter 9 (IHD/MI Morphology)
- Homeopathic Materia Medica (Boericke); Dr. Bhatia's Homeopathy; Balance Into Health
Note on Golwala's Medicine & Davidson's: These specific books are not available in the current medical library. Goldman-Cecil Medicine (International Edition) is used as the closest equivalent — it is similarly structured for clinical medicine and follows the same scope. Key Golwala/Davidson's-style clinical points (symptom-to-management orientation) are fully covered above. If you have access to specific page references from Golwala or Davidson's you'd like incorporated, please share them and they can be added directly.
This is a shared conversation. Sign in to Orris to start your own chat.