Explain the pathophysiology of burns
Reading File
Finding Sources
Searching PubMed
"burns" AND "pathophysiology"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from both Rosen's Emergency Medicine and Sabiston's Textbook of Surgery. Let me now compose the full detailed answer.
Pathophysiology of Burns
Burns result from transfer of energy to body tissues - by heat (thermal), electricity, chemicals, or radiation - causing a cascade of local and systemic responses proportional to burn depth and total body surface area (TBSA) involved.
1. Mechanism of Initial Tissue Injury
Thermal injury begins when tissue temperature exceeds biologic tolerance. At temperatures as low as 41°C, cellular protein denaturation begins. As temperature rises, coagulative necrosis results - membranes disrupt, enzymes denature, and cells die. The depth of injury follows a first-order logarithmic distribution from the surface inward: the higher the temperature and the longer the exposure, the deeper the injury penetrates.
- Flame burns transfer energy by convection and radiation
- Scald burns transfer by conduction (water has thermal conductivity of 0.61 W/m/°C; cooking oil ~4.2 J/g/°C - transfers heat faster, causing deeper burns)
- Electrical burns injure membranes directly in addition to heat transfer
- Chemical burns also cause direct membrane damage alongside thermal effects
- Friction burns act through shearing forces
Very high surface temperatures (>280°F / ~138°C) in flame burns trigger a Maillard-type reaction, causing characteristic color change and consistency alteration of the eschar. Lower temperature scald burns can be deceptively deep despite a different appearance.
2. Local Changes: The Three Zones of Burn Injury
After the inciting source is removed, a classic three-zone pattern of injury develops in the skin (originally described by Jackson):
| Zone | Description | Fate |
|---|---|---|
| Zone of Coagulation (center) | Irreversible coagulative necrosis - cells are dead | Irreversible |
| Zone of Stasis (intermediate) | Ischemia from microvascular damage; cells are injured but potentially viable | Potentially reversible with treatment |
| Zone of Hyperemia (periphery) | Increased blood flow, inflammation, minimal cell injury | Spontaneously reversible |
The cellular mechanisms in these zones involve necrosis/necroptosis (causing significant inflammation), autophagy (potentially protective), and early or delayed apoptosis (less inflammatory, but still causes cellular loss). Without proper management, the zone of stasis can convert to coagulation - meaning the burn "deepens."
3. Burn Depth Classification
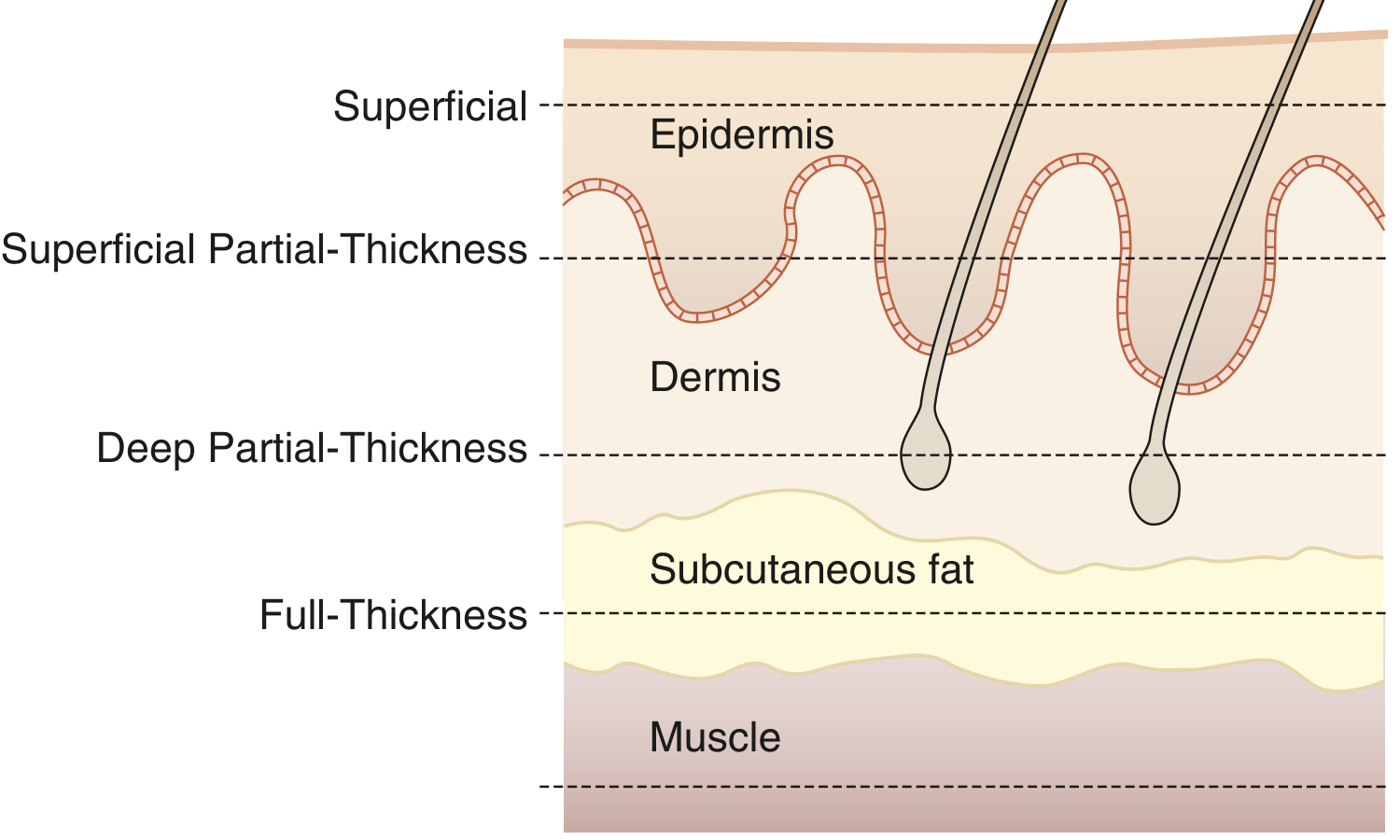
Depths of a burn. Superficial burns are confined to the epidermis. Superficial partial-thickness burns extend into the papillary dermis. Deep partial-thickness burns reach the reticular dermis. Full-thickness burns extend through both layers into subcutaneous fat and beyond. - Sabiston Textbook of Surgery, p. 852
| Depth | Structures Involved | Appearance | Sensation | Healing |
|---|---|---|---|---|
| Superficial (1st degree) | Epidermis only | Erythematous, blanches, dry | Painful | 7 days, no scar |
| Superficial partial-thickness (2nd degree, shallow) | Epidermis + papillary dermis | Red, blisters, blanches, wet | Painful | 7-14 days, minimal scar |
| Deep partial-thickness (2nd degree, deep) | Epidermis + reticular dermis | Pale, mottled, non-blanching | Painful to pinprick | 15-21 days, severe scarring |
| Full-thickness (3rd degree) | Entire epidermis and dermis | Leathery eschar, white/black/cherry red | Insensate | Cannot self-heal; requires grafting |
| Deep full-thickness (4th degree) | Into muscle, tendon, bone | Charred | Insensate | Major reconstruction needed |
Superficial partial-thickness burns re-epithelialize from retained rete ridges and follicular keratinocytes. Full-thickness burns have no residual keratinocytes and must heal from wound edges - hence the need for surgical excision and skin grafting.
4. Systemic Pathophysiology: Burn Shock
Burns exceeding ~15-20% TBSA trigger major systemic responses. The clinical course passes through two well-defined phases:
Phase 1: Hypodynamic (Ebb) Phase - 0 to 24-72 hours
- Massive release of inflammatory mediators and cytokines (TNF-α, IL-1, IL-6, histamine, serotonin, bradykinin, prostaglandins, thromboxane A2) both locally and into the systemic circulation
- Reactive oxygen species (ROS) are generated, causing endothelial damage
- Microvascular permeability increases dramatically - fluid, proteins, and electrolytes shift from the intravascular to interstitial space (capillary leak)
- Result: massive edema, hypoproteinemia, and reduced circulating volume
- Decreased cardiac output with increased systemic vascular resistance
- Transmembrane potential disruption across cells throughout the body
- The leak follows either a biphasic pattern (peak at 1 hour and again at 12-24 hours) or a single peak in the first 8 hours with gradual reduction over the following 16 hours
- Imbalance between oncotic and hydrostatic forces develops due to hypoproteinemia and capillary leak - this is what drives the aggressive fluid resuscitation requirement
Phase 2: Hyperdynamic (Flow) Phase - begins 24-72 hours post-burn
- Vascular permeability and SVR drop
- Heart rate and cardiac output increase markedly
- Metabolic rate rises 2-3 fold (hypermetabolism) - one of the most pronounced hypermetabolic states in medicine
- Catecholamine and cortisol surges drive this response
5. Systemic Inflammatory and Immunological Effects
- Immune dysfunction: both cellular and humoral immunity are impaired, predisposing to sepsis
- Neutrophil dysfunction: neutrophils are activated systemically but have impaired chemotaxis and killing ability
- Massive inflammatory cytokine release causes systemic inflammatory response syndrome (SIRS) which can progress to multiorgan dysfunction
6. Metabolic and Endocrine Effects
The hypermetabolic state in large burns involves:
- Insulin resistance and hyperglycemia
- Muscle wasting (protein catabolism)
- Elevated serum triglycerides and free fatty acids
- Bowel mucosa degradation with reduced absorptive capacity (gut barrier failure contributes to bacterial translocation)
- Hormonal changes: reduced growth hormone, TSH, T3, T4, and testosterone
- Negative nitrogen balance from catabolism
7. Cardiovascular Effects
- Initial burn shock: reduced preload (from fluid shifts and hypovolemia), impaired myocardial function (from circulating myocardial depressant factors and cytokines), increased afterload
- Later: hyperdynamic circulation with elevated cardiac output
- Myocardial dysfunction can occur even without direct cardiac injury, particularly in large burns
8. Renal Effects
- Reduced renal perfusion in the ebb phase leads to acute tubular necrosis (ATN)
- In electrical burns, massive myoglobinuria from rhabdomyolysis causes pigment nephropathy and tubular obstruction
- Adequate fluid resuscitation is the cornerstone of renal protection
9. Inhalation Injury
Inhalation injury occurs in ~6% of all burns (up to 60% in large facial burns) and is the third most important predictor of mortality after age and TBSA - it nearly triples mortality and decreases LD-50 by 25%.
- Upper airway (thermal injury): Direct heat causes inflammation, edema, and ischemia-reperfusion injury. Progressive airway edema can threaten patency within hours. The glottic closure reflex can cause rapid asphyxiation.
- Lower airway (chemical injury): Inhaled combustion products cause bronchospasm, mucosal ulceration, pseudomembrane formation, surfactant loss, and impaired ciliary transport. Consequences include V/Q mismatch, decreased lung compliance, increased dead space, and infection risk.
- Systemic toxicity: Carbon monoxide (CO) binds hemoglobin with 200x the affinity of O2, causing cellular hypoxia. Cyanide from burning plastics/synthetics inhibits cytochrome c oxidase (mitochondrial electron transport), causing histotoxic hypoxia.
10. Wound Healing Phases
Following the acute injury, burn wound healing proceeds through three phases, all of which can be disrupted:
- Inflammatory phase: Neutrophil and macrophage infiltration, debridement of necrotic tissue, cytokine signaling
- Proliferative phase: Fibroblast migration, collagen deposition, angiogenesis, re-epithelialization
- Remodeling phase: Collagen cross-linking, scar maturation - can last 1-2 years; hypertrophic scarring and contracture are major complications
Summary
Burns produce injury through a combination of direct thermal (or chemical/electrical) tissue destruction and a self-amplifying inflammatory cascade. Locally, irreversible necrosis at the burn center is surrounded by potentially salvageable ischemic tissue whose fate depends on resuscitation quality. Systemically, the initial hypodynamic phase of capillary leak and shock gives way to a hypermetabolic flow state that stresses virtually every organ system. Inhalation injury, infection, and multiorgan failure are the main drivers of mortality in large burns.
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, pp. 831-832
- Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, pp. 852-853
- Recent review: Dobson GP et al. "Pathophysiology of Severe Burn Injuries: New Therapeutic Opportunities From a Systems Perspective." J Burn Care Res, 2024 [PMID: 38517382]
This is a shared conversation. Sign in to Orris to start your own chat.