TB patient Bp - 90/60 Pr. - 130 (usually her baseline) Spo2-98% Suddenly complaining of chest pain Radiation to arm and back
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have everything needed. Here is the full clinical breakdown:
TB Patient - Acute Chest Pain with Hypotension
Vital Signs at a Glance
| Parameter | Value | Interpretation |
|---|---|---|
| BP | 90/60 mmHg | Hypotension - critical |
| PR | 130 bpm (her baseline) | Tachycardia |
| SpO2 | 98% | Preserved for now |
| Chest pain | Radiating to arm and back | Multi-directional radiation |
Most Likely Diagnosis: Cardiac Tamponade (until proven otherwise)
Why tamponade first?
This patient has active TB - and TB is one of the most common causes of pericardial effusion and tamponade, particularly in endemic settings. The combination of:
- Hypotension (BP 90/60)
- Tachycardia (PR 130)
- Chest pain in a known TB patient
...should make tamponade your top differential until bedside echo proves otherwise. In Africa and South Asia, TB causes up to 70% of pericardial effusions in HIV-positive patients and remains a major cause overall.
- Tintinalli's Emergency Medicine, p. 2969-2970
- Rosen's Emergency Medicine, p. 590
Differential Diagnosis - Prioritized
1. Cardiac Tamponade (TOP PRIORITY)
- TB pericarditis causes pericardial effusion that can accumulate and compress the heart
- Classic Beck's Triad: Hypotension + Muffled heart sounds + Distended neck veins
- Pulsus paradoxus (>10 mmHg drop in systolic BP with inspiration) is the sine qua non
- Fishman's Pulmonary Diseases, p. 3686
2. Aortic Dissection
- Pain radiating to the back is the classic red flag
- Described as tearing/severe, maximal at onset, may migrate
- TB-related aortitis (rare) or coincidental hypertension-related
- Rosen's Emergency Medicine - Table 22.2
3. Acute MI / ACS
- Radiation to the arm points here
- Substernal crushing/pressure pain with arm radiation = classic for acute MI
- Cannot be excluded without ECG + troponin
- Rosen's Emergency Medicine, Table 22.2
4. Pulmonary Embolism
- TB patients are in a pro-inflammatory, pro-coagulant state
- Can cause chest pain, hypotension, tachycardia
- SpO2 98% makes massive PE less likely but not impossible
5. Tuberculous Pericarditis (without tamponade yet)
- Pleuritic chest pain, friction rub
- May not have hemodynamic compromise if effusion is small
IMMEDIATE BEDSIDE ASSESSMENT
Do RIGHT NOW (simultaneously):
- Listen to heart sounds - are they muffled/distant?
- Check JVP - elevated neck veins?
- Check for pulsus paradoxus - measure BP on inspiration vs expiration (>10 mmHg drop is significant, >20 mmHg = tamponade)
- 12-lead ECG - look for:
- Electrical alternans (beat-to-beat QRS voltage variation) = tamponade
- ST elevations (STEMI or pericarditis - saddle-shaped in all leads)
- ST depression in aVR with diffuse ST elevation = pericarditis
- Bedside POCUS/Echo - this is the most important test
Beck's Triad (check all three):
| Finding | Present? |
|---|---|
| Hypotension | YES - BP 90/60 |
| Muffled heart sounds | Check now |
| Distended neck veins | Check now |
If 2 or 3 of Beck's triad are present + this clinical context = presume tamponade, prepare for pericardiocentesis
Bedside Ultrasound (POCUS)
This is the single most important diagnostic step. Look for:
- Pericardial fluid (anechoic stripe around heart)
- Right atrial/ventricular wall collapse during diastole = tamponade physiology
This is what tamponade looks like on subcostal echo - pericardial fluid (*) and collapse of the right atrium/ventricle (white arrowheads):
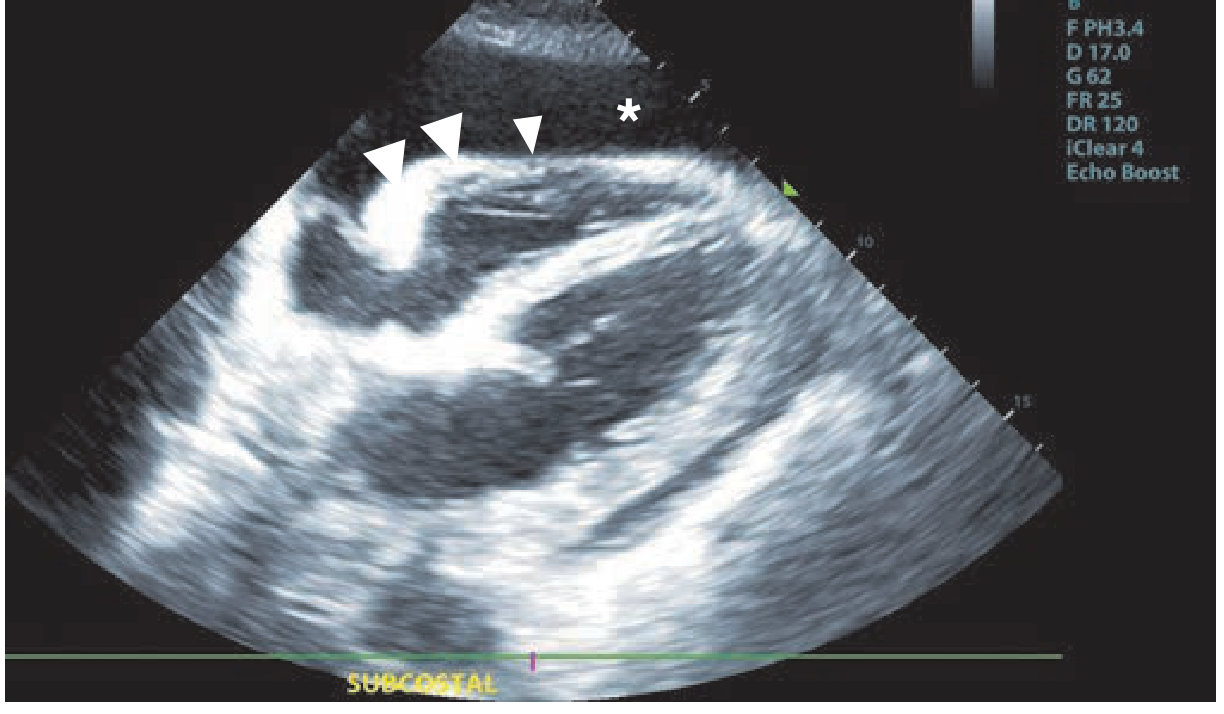
Fishman's Pulmonary Diseases - subcostal POCUS in tamponade
Emergency Management
If Tamponade Confirmed or Strongly Suspected:
1. Call for emergency pericardiocentesis immediately
- This is both diagnostic and therapeutic
- Needle aspiration of pericardial fluid relieves compression
- Ultrasound guidance is preferred
- Subxiphoid approach is standard
- Even draining a small amount (50-100 mL) can dramatically improve hemodynamics
- Rosen's Emergency Medicine, p. 590
2. Supportive measures while preparing:
- IV fluid bolus (cautious - may buy time by maintaining preload)
- Supplemental O2
- Do NOT give vasodilators or diuretics - they will precipitate complete cardiovascular collapse
- Avoid positive pressure ventilation if possible (reduces venous return)
- Keep patient upright/leaning forward if tolerating
3. Investigations to run in parallel:
- ECG (STAT)
- Troponin, D-dimer, CBC, CRP, ESR
- CXR (water-bottle heart silhouette = large effusion)
- Blood cultures
- If available: CT aortography (to rule out dissection if pain is predominantly tearing + back)
Distinguishing Features at the Bedside
| Feature | Tamponade | Dissection | ACS |
|---|---|---|---|
| Pain character | Chest pressure, pleuritic | Tearing, maximal at onset | Crushing, pressure |
| Radiation | Variable | Back, jaw, neck | Arm, jaw |
| JVP | Elevated | Normal or variable | Normal/low |
| Heart sounds | Muffled | Normal | Normal |
| ECG | Electrical alternans, low voltage | May show ischemia if coronary involved | ST changes |
| BP discrepancy arms | No | Yes (>20 mmHg) | No |
| Echo | Effusion + RV collapse | Aortic flap/widening | Wall motion abnormality |
Bottom Line
This TB patient with hypotension, tachycardia, and chest pain has cardiac tamponade until proven otherwise. Do not wait for confirmatory tests if Beck's triad is present - call for emergency pericardiocentesis. Run bedside POCUS immediately. Keep dissection and ACS as active differential diagnoses requiring rapid exclusion with ECG, echo, and CT if the patient stabilizes.
- Tintinalli's Emergency Medicine (tamponade management)
- Rosen's Emergency Medicine (chest pain differentials, tamponade key concepts)
- Fishman's Pulmonary Diseases (Beck's triad, POCUS in tamponade)
- Goldman-Cecil Medicine (TB pericardial complications: 1-8% of TB patients develop tamponade/constriction)
She doesnt say of classic chest pain She says that when she coughs she has chest pain radiating to arm n back
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
This extra detail is very important. Here is the updated analysis:
Updated Assessment - Pain Only on Coughing
What This Changes
Cough-triggered pain that radiates to arm and back is pleuritic in character - it is provoked by respiratory movement (coughing, deep breathing, inspiration). This is fundamentally different from spontaneous resting chest pain. It significantly lowers the probability of ACS or aortic dissection and raises the probability of TB-related thoracic pathology.
Revised Top Differentials
1. TB Pericarditis (Most Likely)
Pericarditis causes sharp, pleuritic-type chest pain that is:
- Worse with deep breathing and coughing
- Worse lying flat, better sitting forward
- Radiates to the neck, shoulder, and arms - this is characteristic
- Associated with dyspnea, cough, hiccups
TB is a direct cause of pericarditis. The radiation pattern (arm + back) fits exactly with referred pericarditic pain via the phrenic nerve (C3-C5 dermatome = shoulder and arm referral).
"The symptoms of pericarditis include sharp retrosternal pain, localized or radiating to the neck, shoulder, or arms, that is made worse with lying down and improves with sitting up. The pain is sharp in nature and is worse with a deep breath. Patients can have associated dyspnea, cough..."
- Textbook of Family Medicine, 9e, p. 873
2. TB Pleuritis / Pleural Effusion (Very Likely, possibly concurrent)
TB pleuritis classically presents with:
- Fever, cough, pleuritic pain, and dyspnea
- Pleuritic pain = sharp pain provoked by breathing/coughing
- Effusion causes dullness on that side
"In some patients, the tuberculous involvement of the pleura is manifested as an acute illness with fever, cough, pleuritic pain, and occasionally dyspnea and weight loss."
- Murray & Nadel's Respiratory Medicine, p. 1305
Radiation to the shoulder/arm from pleuritis occurs when the diaphragmatic pleura is irritated - the phrenic nerve (C3-C5) mediates referred pain to the shoulder and arm. Back pain occurs when the posterior parietal pleura is involved.
3. Pericarditis + Effusion Progressing to Tamponade
The hypotension (90/60) in this setting is the most alarming feature. Even with cough-triggered pain suggesting pericarditis/pleuritis, you must rule out developing tamponade:
- TB pericarditis leads to tamponade in ~33% of symptomatic cases
- Tachycardia (PR 130) + hypotension = Beck's triad is incomplete but tamponade physiology may already be present
- Fuster and Hurst's The Heart, 15th Ed, p. 128
4. Musculoskeletal / Rib Pain from Coughing (lower priority given hypotension)
Chronic heavy coughing in TB can cause:
- Costochondritis or rib stress fractures
- Pain sharp, reproducible on palpation, worse with coughing
- Would NOT explain the hypotension - so this is a diagnosis of exclusion
The Hypotension Remains the Problem
Even though the pain character is pleuritic, BP 90/60 cannot be attributed to musculoskeletal pain or simple pleuritis. It forces you to keep pericardial tamponade and other hemodynamically significant causes on the table.
Possible reasons for hypotension in this TB patient:
| Cause | Clues |
|---|---|
| Cardiac tamponade | Elevated JVP, muffled heart sounds, pulsus paradoxus |
| Large pleural effusion with mediastinal shift | Tracheal deviation, absent breath sounds, dull percussion |
| Sepsis (TB-related or superinfection) | Fever, high WBC, warm peripheries |
| Adrenal insufficiency (TB adrenalitis) | Chronic TB, fatigue, hyponatremia |
| Medication side effect (anti-TB drugs) | Rifampicin - drug interactions |
| Dehydration / poor oral intake | Likely in TB patient with chronic illness |
Bedside Assessment - Do Now
Listen and Examine:
- Auscultate heart - friction rub? (pericarditis) - muffled sounds? (tamponade/effusion)
- Auscultate lungs - absent breath sounds + dullness on one side? (pleural effusion)
- Check JVP - raised = tamponade or right heart compression
- Check pulsus paradoxus - >10 mmHg drop in systolic with inspiration
- Palpate chest wall - reproducible tenderness on pressing ribs/costochondral junctions? (musculoskeletal)
- Ask: Does the pain change with position? (Better sitting forward = pericarditis)
Investigations (STAT):
- Bedside POCUS - pericardial effusion? pleural effusion? RV collapse?
- ECG - diffuse ST elevation in all leads (saddle-shaped) + PR depression = pericarditis; electrical alternans = tamponade
- CXR - water-bottle heart (pericardial effusion), opacified hemithorax (pleural effusion), widened mediastinum
- CBC, CRP, ESR - inflammatory markers
- Troponin - myopericarditis involvement?
- Blood cultures - sepsis workup
Summary
| Feature | Supports |
|---|---|
| TB patient | Pericarditis, pleuritis |
| Pain ONLY with coughing | Pleuritic origin (pericarditis, pleuritis) |
| Radiation to arm | Phrenic nerve referral (pericarditis, diaphragmatic pleuritis) |
| Radiation to back | Posterior parietal pleura involvement |
| Hypotension 90/60 | Tamponade, sepsis, adrenal insufficiency - CANNOT ignore |
| PR 130 (her baseline) | Less helpful diagnostically |
| SpO2 98% | Against massive PE, against severe pneumonia |
Bottom line: The pain pattern points to TB pericarditis with or without pleural effusion. The hypotension demands you urgently exclude cardiac tamponade with bedside echo before anything else. Do not let the pleuritic character of the pain falsely reassure you - a pericarditic patient can have exactly this presentation and still be in early tamponade.
- Textbook of Family Medicine 9e (pericarditis pain characteristics)
- Murray & Nadel's Respiratory Medicine (TB pleuritis clinical features)
- Tintinalli's Emergency Medicine (TB reactivation - pleuritic chest pain)
- Fuster and Hurst's The Heart, 15th Ed (TB pericarditis, tamponade risk)
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
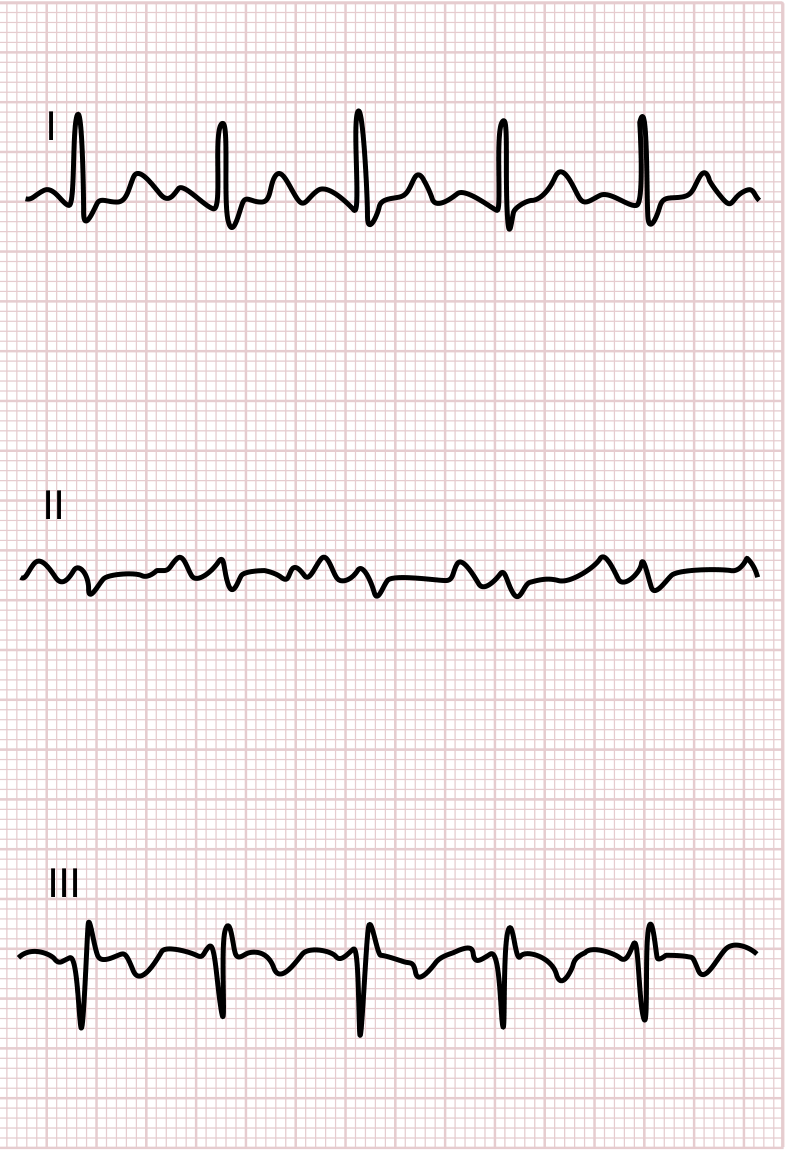
Now I have everything needed for a comprehensive ECG interpretation. Here is the full analysis:
ECG Interpretation - Manjusha, 25F, TB Patient
Machine Measurements (from the strip)
| Parameter | Value |
|---|---|
| Heart Rate | 138 bpm |
| PR interval | 106 ms |
| QRS duration | 62 ms (narrow) |
| QTc | 409 ms (normal) |
| P/QRS/T Axis | 75° / 94° / 13° |
Key ECG Findings
1. Sinus Tachycardia - 138 bpm
- P waves present before every QRS, regular rhythm
- Rate of 138 is consistent with her clinical presentation
2. Right Axis Deviation (RAD) - QRS axis +94°
- QRS predominantly negative in Lead I, positive in aVF
- In a 25-year-old female with hypotension and pleuritic chest pain - this is a red flag
- RAD in this context = right ventricular strain/overload
3. No Electrical Alternans
- QRS amplitude does not alternate beat-to-beat
- This argues against massive pericardial effusion/tamponade as the primary driver of her hemodynamics
4. No Diffuse ST Elevation / No PR Depression
- No saddle-shaped concave ST elevation in multiple leads
- No PR depression
- This argues against acute pericarditis as the diagnosis
5. Inferior T-wave inversions (III, aVF)
- T-wave inversions in the inferior leads
6. Mild ST depression in lateral leads (I, aVL, V4-V6)
- Could be rate-related (secondary repolarization changes at HR 138)
- Or right heart strain pattern
The Critical Pattern: S1 + RAD + Inferior T inversions
Compare her ECG to the classic PE pattern from Goldman-Cecil Medicine:
Goldman-Cecil Medicine - Classic ECG findings in PE: S1, Q3, T3 pattern
Her ECG shows:
- S waves in lead I (biphasic/predominantly negative) ✓
- T-wave inversions in III and aVF ✓
- Right axis deviation ✓
- Sinus tachycardia ✓ (most common ECG finding in PE)
This is a partial S1Q3T3-equivalent pattern - the most recognized ECG sign of right ventricular strain from pulmonary embolism.
"The ECG may show new changes suggestive of right ventricular strain, such as T wave inversion in leads V1 to V4; the classic S1, Q3, and T3 pattern; and complete or incomplete right bundle branch block. However, these ECG changes have limited sensitivity and are mainly found in patients with more extensive pulmonary emboli."
- Goldman-Cecil Medicine, p. 2671
Revised Primary Diagnosis: Pulmonary Embolism
The ECG, combined with the clinical picture, now makes PE the leading diagnosis:
| Clinical Feature | PE Fit |
|---|---|
| TB patient (hypercoagulable state, immobility, inflammation) | ✓ Strong risk factor |
| Pleuritic chest pain (worse with coughing) | ✓ Classic - pleural irritation from infarction |
| Radiation to back/shoulder | ✓ Diaphragmatic/pleural referral |
| Hypotension BP 90/60 | ✓ Massive/submassive PE causing RV failure |
| Tachycardia 138 bpm | ✓ Most common ECG finding in PE |
| SpO2 98% | ✓ Possible (can be preserved in PE, especially initially) |
| Right axis deviation on ECG | ✓ RV strain/pressure overload |
| Inferior T inversions + S1 pattern | ✓ S1Q3T3-equivalent |
| No electrical alternans | ✓ Makes tamponade less likely |
| No diffuse ST elevation | ✓ Makes pericarditis less likely |
Immediate Management
STAT Investigation:
- CT Pulmonary Angiography (CTPA) - gold standard for PE diagnosis
- D-dimer - if negative, effectively excludes PE
- Bedside Echo - look for RV dilation, RV:LV ratio >0.9, McConnell sign, septal bowing - confirms RV strain from PE
- Troponin + BNP - elevated = myocardial injury from RV strain, determines severity
- ABG - hypoxia and respiratory alkalosis typical in PE (SpO2 can be deceptively normal on peripheral oximetry)
- Lower limb Doppler - DVT as source
If Massive PE (hemodynamically unstable = this patient with BP 90/60):
- Anticoagulation immediately - LMWH or UFH (if thrombolysis is being considered, use UFH)
- Consider systemic thrombolysis (tPA/streptokinase) - indicated in massive PE with hemodynamic compromise if no contraindications
- IV fluids cautiously (RV is preload dependent but over-loading worsens septal shift)
- Supplemental O2
- Vasopressors (noradrenaline) if BP does not respond to fluids
Note on anti-TB drugs:
- Rifampicin induces CYP enzymes - major interaction with anticoagulants
- If on warfarin: doses need significant upward adjustment
- DOACs (apixaban/rivaroxaban) are also affected by rifampicin - use LMWH as the safer choice in TB patients on anti-TB therapy
Summary - Diagnosis Hierarchy After ECG
| Diagnosis | Pre-ECG | Post-ECG |
|---|---|---|
| Pulmonary Embolism | Possible | Now TOP - ECG supports RV strain |
| TB Pericarditis/Tamponade | High | Lower - no electrical alternans, no diffuse ST elevation |
| TB Pleuritis | Possible | Still possible (concurrent) |
| ACS | Low | Very low - no ST elevation, 25F |
This patient needs urgent CTPA and echo. The ECG points squarely toward PE with RV strain as the cause of her hypotension, tachycardia, and pleuritic cough-related chest pain.
- Goldman-Cecil Medicine (PE ECG findings - S1Q3T3, p. 2671)
- Goldman-Cecil Medicine (echo in PE - RV dysfunction markers, p. 2675)
- Tintinalli's Emergency Medicine (TB and extrapulmonary manifestations)
She did say her pain decreased But still gave pmol 1g iv stat Will repeat ecg after 20 mins
Good clinical thinking giving paracetamol (PCM/pmol) 1g IV - it addresses pain and any fever component, and the fact that her pain decreased after paracetamol is actually a very useful diagnostic clue.
What Pain Relief with Paracetamol Tells You
Pain that responds to a simple analgesic/antipyretic suggests:
- An inflammatory/pleuritic origin (pericarditis, pleuritis) rather than ischemic or embolic
- ACS pain typically does NOT respond to paracetamol
- PE-related pleuritic pain CAN partially respond (it is inflammatory at the pleural surface after infarction)
- Pericarditis pain responds well to anti-inflammatory agents
- Musculoskeletal pain also responds
This slightly moves the picture back toward TB pericarditis/pleuritis, but does NOT exclude PE - a pulmonary infarct causes local pleural inflammation which can be temporarily dulled by antipyretics.
Awaiting the Repeat ECG - What to Look For
When the repeat ECG comes in 20 minutes, compare specifically:
| Finding | What It Means |
|---|---|
| Rate decreased (from 138) | Pain/fever was driving tachycardia - reassuring |
| Right axis deviation resolved | Was rate-related or positional - PE less likely |
| Right axis persists or worsens | True RV strain - PE still high on list |
| New ST elevation appears (diffuse, saddle-shaped) | Pericarditis unmasking as inflammation evolves |
| PR depression appears | Pericarditis pattern |
| Electrical alternans appears | Tamponade developing - emergency |
| T inversions deepen in V1-V4 | Worsening RV strain |
| Rate normalizes AND axis normalizes | Rate-related changes - ECG was reactive, not primary |
Right Now, While Waiting
Don't wait for the ECG - these can run in parallel:
-
Bedside POCUS right now - takes 2 minutes, answers the biggest question:
- Pericardial effusion? → pericarditis/tamponade
- RV dilated with D-shaped septum? → PE
- Normal? → less urgent, reassess
-
Check if pain truly gone or just reduced - partial response keeps PE/pericarditis both alive
-
D-dimer - send it now if not already sent; if negative it effectively rules out PE
-
Note the BP trend - did BP improve at all after paracetamol? If hypotension persists despite pain relief, the cause of hypotension is structural/hemodynamic, not pain-mediated
-
Fever? - check temperature; fever in a TB patient + pericarditis would strongly favor TB pericarditis/pleuritis over PE
Clinical Bottom Line Right Now
Pain partially responding to IV paracetamol + pleuritic character + TB background = TB pericarditis or pleuritis is re-emerging as the top diagnosis, but the ECG's RAD and S1 pattern mean PE is still not off the table.
The repeat ECG in 20 minutes will be very informative - especially the heart rate and QRS axis. If rate comes down to 100-110 and the axis normalizes, the previous ECG changes were likely rate-driven and pericarditis/pleuritis becomes the dominant diagnosis. If rate and axis stay abnormal despite pain relief, PE needs urgent CTPA.
Post the repeat ECG when ready - happy to compare them side by side.

Repeat ecg
analyse_media
analyse_media
Excellent - this is very informative. Here is the full comparison:
Repeat ECG Analysis - Manjusha (28 mins after PCM 1g IV)
Side-by-Side Comparison
| Parameter | ECG #1 (01:08 AM) | ECG #2 (01:35 AM) | Change |
|---|---|---|---|
| Heart Rate | 138 bpm | 128 bpm | ↓ 10 bpm - mild improvement only |
| QRS Axis | +94° (Right Axis Deviation) | Normal axis (~+60°) | ✅ RAD RESOLVED |
| ST segments | Mild lateral depression | Isoelectric - normalized | ✅ RESOLVED |
| Inferior T inversions (III, aVF) | Present in III, aVF | Still present in lead III | ⚠️ PERSISTS |
| S wave in Lead I | Present | Present | Persists |
| Q wave in Lead III | Questionable | Present | More clear now |
| T inversion in Lead III | Present | Present | Persists |
| Electrical alternans | Absent | Absent | Against tamponade |
| Diffuse ST elevation / PR depression | Absent | Absent | Against pericarditis |
| QTc | 409 ms | 409 ms | Stable |
Key Interpretation
✅ Good news - what resolved:
- Right axis deviation is gone - the previous RAD was partly rate-driven (at HR 138, electrical axis shifts rightward)
- ST depressions in lateral leads resolved - confirmed as rate-related repolarization changes, not ischemia
- Pain has improved with PCM
⚠️ What persists and is significant:
The S1-Q3-T3 pattern is still present and clearer on this ECG:
- S wave in Lead I - persists
- Q wave in Lead III - now more clearly visible
- T inversion in Lead III - persists
This pattern persisting even after rate came down (from 138 → 128) and axis normalized means it is not simply a rate-related finding. It represents a true structural/vascular finding.
Diagnosis: Pulmonary Embolism remains the leading diagnosis
The S1Q3T3 pattern is the hallmark of right ventricular strain from pulmonary embolism. The fact that it:
- Was present on ECG #1 when HR was 138
- Remains present on ECG #2 when HR is 128 and axis has normalized
- Is NOT associated with diffuse ST elevation (ruling out pericarditis)
- Is NOT associated with electrical alternans (ruling out tamponade)
...makes this a persistent RV strain pattern, not a rate-dependent artifact.
Revised Clinical Picture
| Finding | Interpretation |
|---|---|
| S1Q3T3 persisting on repeat ECG | RV strain - PE until proven otherwise |
| RAD resolved → Normal axis | Was partly rate-driven, not fixed anatomical |
| ST depressions resolved | Rate-related, not ischemic |
| Pain reduced with PCM | Pleuritic/inflammatory origin |
| HR still 128 despite pain relief | Not purely pain-driven tachycardia - ongoing hemodynamic stress |
| BP still 90/60 (check again now) | Hypotension persisting = hemodynamically significant PE |
Urgent Next Steps
Do not delay on:
-
Re-check BP right now - has it improved at all with PCM?
-
CTPA (CT Pulmonary Angiography) - this is now the most important next step. S1Q3T3 + hypotension + tachycardia + TB patient (hypercoagulable) = clinical probability for PE is HIGH
-
Bedside Echo (POCUS) - if CTPA is not immediately available:
- Look for RV dilation (RV > LV in apical 4-chamber)
- D-shaped interventricular septum (septal bowing into LV)
- McConnell sign (RV free wall hypokinesis with preserved apex)
- These findings = high probability PE, enough to start treatment
-
D-dimer - send immediately if not already done
-
ABG - check for hypoxia (SpO2 98% does not fully exclude hypoxemia on pulse ox)
-
Start anticoagulation if clinical probability is high and no contraindications:
- LMWH (enoxaparin) preferred in TB patients on anti-TB drugs (safer than warfarin/DOACs due to rifampicin interactions)
- Dose: 1 mg/kg subcutaneous BD (weight-based)
- If massive PE with refractory hypotension: consider thrombolysis (streptokinase or alteplase)
Bottom line: Two ECGs showing persistent S1Q3T3 in a hypotensive, tachycardic TB patient with pleuritic chest pain = get CTPA now and start anticoagulation. Don't wait for the third ECG.
This is a shared conversation. Sign in to Orris to start your own chat.