According to rook's book of dermatology tell me about "Acne" in detail.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Note on source: Rook's Textbook of Dermatology (Wiley-Blackwell) is not in the library database, but the library holds two closely authoritative equivalents - Dermatology, 2-Volume Set, 5th Edition (Griffiths/Barker/Bleiker - same Rook school/tradition, same publisher lineage) and Fitzpatrick's Dermatology. The detailed account below is drawn directly from both, cross-referenced throughout.
Acne Vulgaris - A Detailed Account
1. Definition and Overview
Acne vulgaris is a multifactorial chronic inflammatory disorder of the pilosebaceous unit. The clinical picture ranges widely - from mild comedonal acne to fulminant systemic disease. Most cases present with a pleomorphic array of lesions: comedones, papules, pustules, and nodules with varying extent and severity.
Although the course may be self-limited in many patients, sequelae can be lifelong - including scar formation and significant psychological impairment, especially in young people.
- Dermatology 2-Volume Set 5e, p. 717
2. Historical Note
The term "acne" was first used in the sixth century CE by Aetius Amidenus, physician to the Emperor Justinian. Its etymology is debated - it may derive from the Greek acme (peak) or may itself be the original term. It fell out of use until the 1800s, when it re-entered medical dictionaries. In 1842, Erasmus Wilson formally separated acne simplex (acne vulgaris) from acne rosacea.
- Dermatology 2-Volume Set 5e, p. 717
3. Epidemiology
-
Affects approximately 40-50 million individuals per year in the US alone, with an annual US cost of at least $2.5 billion
-
Globally, acne accounts for ~0.3% of total and ~15% of the dermatologic disease burden
-
~85% of young people aged 12-24 years are affected - it is effectively a physiological occurrence in adolescence
-
The age of puberty onset has been dropping, so preadolescent acne (ages 7-11) has become increasingly common
-
Acne commonly persists well into adulthood: 35% of women and 20% of men in their 30s report acne; 26% of women and 12% of men still affected in their 40s
-
Prevalence rates in adults: up to 64% in the 20s and 43% in the 30s
-
After age 50: 15% of women and 7% of men still have acne
-
White males have a tendency toward more severe nodulocystic disease
-
Acne is also more severe in patients with the XYY karyotype
-
Two indigenous populations - one in Papua New Guinea and one in Paraguay - have been described who do not develop acne, possibly due to the absence of a westernized diet
-
Fitzpatrick's Dermatology, p. 1421; Dermatology 2-Volume Set 5e
4. Genetic Factors
-
Family history is reported in 62.9-78% of patients
-
Those with family history tend to be male, have earlier onset, truncal involvement, and scarring
-
Twin studies: 81% of acne variation is caused by genetic factors vs. 19% environmental; up to 98% of monozygotic twins both have acne vs. 55% of dizygotic twins
-
The number, size, and activity of sebaceous glands is inherited
-
Genetic associations have been found with variants in: TNF-α, TNFR2, IL-1A, CYP17, TLR2, TLR4, and components of the TGF-β pathway and androgen metabolism regulators
-
Genome-wide association studies (GWAS) have further explored this
-
Fitzpatrick's Dermatology, pp. 1421-1422; Dermatology 2-Volume Set 5e
5. Pathogenesis
The diagram below illustrates the sequential stages of acne development:
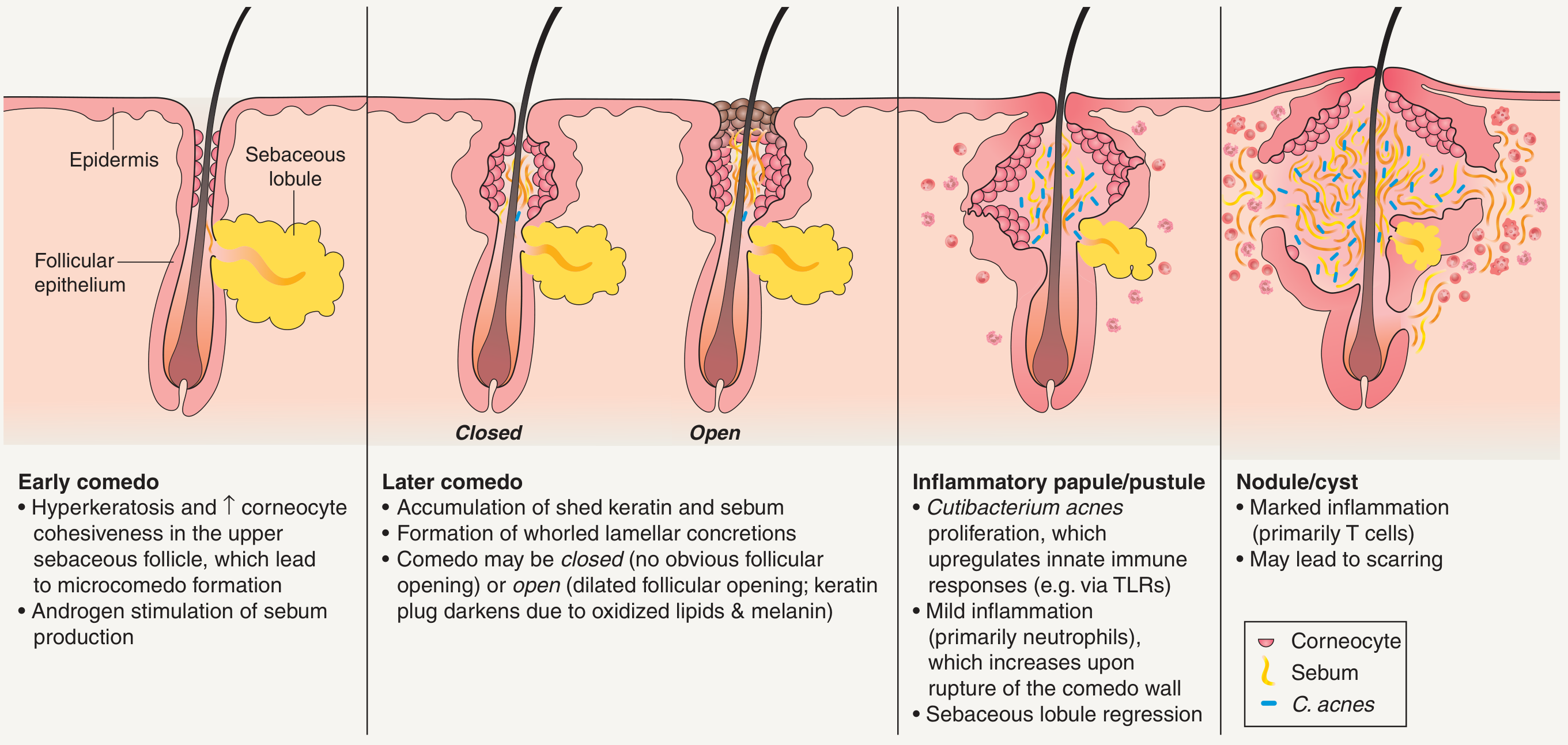
There are four key interlocking pathogenic mechanisms:
5.1 Follicular Epidermal Hyperproliferation (Microcomedo Formation)
- The earliest event is abnormal keratinization of the infundibulum - increased proliferation and retention of corneocytes (hyperkeratosis + increased corneocyte cohesiveness) in the upper sebaceous follicle
- This leads to microcomedo formation - the precursor of all acne lesions
- The infrafundibulum of acne patients responds more readily to comedogenic stimuli than in non-acne individuals
- Exogenous agents that trigger this include: halogenated cyclic hydrocarbons, tar products, some cosmetics, and EGFR inhibitors (cetuximab, gefitinib), which disturb normal follicular differentiation causing excessive follicular hyperkeratosis
5.2 Sebum Production and Androgens
- The presence of well-developed sebaceous follicles on the face, upper chest, and upper back corresponds directly to the distribution of acne
- Acne patients have larger sebaceous glands and produce more sebum than individuals without acne
- Sebum production >1.5-4.0 mg/10 cm² per 3 hours is defined as seborrhea
- Growth of sebaceous glands and increased sebum are induced by androgens, particularly DHT (dihydrotestosterone)
- In men: DHT mainly derived from testosterone
- In women: androstenedione is the main precursor
- Conversion of testosterone to DHT is 30 times higher in acne-affected skin than normal skin
- Eunuchs lacking testicular function do not develop acne
- However, increased sebum alone is insufficient - patients with Parkinson disease have marked seborrhea but no acne
- Sebaceous gland androgen receptors respond to testosterone and DHT; DHT has 5-10× greater affinity for the androgen receptor
- DHEAS (adrenal origin) rises at adrenarche (age 7-8) and is associated with initial comedonal acne development in prepubescent children
- Estrogens in sufficient systemic amounts decrease sebum production but the dose needed exceeds that required to suppress ovulation; lower-dose OCP containing 20-50 mcg ethinyl estradiol is effective by suppressing ovarian androgen production
- Sebaceous glands also express PPARs, retinoid receptors, estrogen/progesterone receptors
5.3 Cutibacterium acnes (formerly Propionibacterium acnes)
- Sebum in sebaceous glands is sterile with no free fatty acids, but the microenvironment of the infundibulum favors growth of C. acnes and S. epidermidis
- In acne patients, C. acnes is quantitatively increased in sebaceous follicles
- Bacterial lipases split di- and triglycerides → producing free fatty acids that:
- Alter the pattern of keratinization within the infundibulum
- Are chemotactic for neutrophils
- High-dose vitamin B12 supplementation increases porphyrin production by C. acnes, promoting inflammation
5.4 Inflammation and Immune Response
Innate immunity:
- C. acnes activates Toll-like receptor 2 (TLR2) and TLR4 on keratinocytes and monocytes
- This triggers production of IL-1, IL-8, IL-12, TNF-α
- Rupture of the comedo wall incites a vigorous neutrophilic inflammatory response with release of reactive oxygen species (ROS) and lysosomal enzymes
- Antimicrobial peptides histone H4 (direct microbial killing) and cathelin (interacts with β-defensins and psoriasin) are secreted locally
- Peripheral blood monocytes differentiate to CD209+ macrophages and CD1b+ dendritic cells in response to C. acnes
Adaptive immunity:
- CD4+ T cells detected in early inflammatory lesions
- Both Th1 and Th17 responses are prominent in vitro and in vivo
- Th17 cells recruit neutrophils - contributing to antibacterial activity but also tissue injury
- ROS and lysosomal enzyme levels correlate with disease severity
5.5 Scarring Mechanism
- Scar formation does not directly correlate with disease severity - it can occur even in mild-moderate acne
- C. acnes induces MMP-1 and MMP-9 (matrix metalloproteinases) → matrix degradation
- All-trans retinoic acid (ATRA) downregulates MMPs and augments TIMP-1 → shifts phenotype toward matrix preservation, explaining one mechanism by which retinoids improve scarring
- In non-scarring lesions: robust initial CD4+ T-cell response that subsides
- In scarring lesions: smaller initial CD4+ T-cell infiltrate but high proportion of skin-homing memory and effector T cells with sustained inflammation during resolution
5.6 Diet and Acne
- High glycemic load diets may exacerbate acne
- Dairy ingestion (especially skim milk and whey protein) is weakly associated with acne
- Both raise IGF-1 → possible increase in androgen activity and sebocyte modulation
- Molecular interplay of FoxO1 and mTOR-mediated nutrient signaling are implicated
- Two indigenous populations (Papua New Guinea, Paraguay) not exposed to westernized diets do not develop acne
6. Clinical Features
6.1 History Taking
Most patients report gradual onset around puberty. An abrupt onset should prompt investigation for:
- Drug-induced acne
- Androgen-secreting tumor
Hyperandrogenism should be suspected in a female with acne that is:
- Severe, jawline/lower face distribution
- Sudden onset
- Associated with hirsutism, irregular menses, deepening voice, increased libido, or acanthosis nigricans
Drug-induced acneiform eruptions (typically monomorphous - all at same stage): anabolic steroids, corticosteroids, ACTH, phenytoin, lithium, isoniazid, vitamin B complexes, halogenated compounds, EGFR inhibitors, progestin-only contraceptives, DHEA/testosterone.
Perimenstrual flares are common in acne vulgaris - 56% of adult women report worsening before menses.
6.2 Cutaneous Findings and Lesion Types
Primary sites: face (most common), back, chest, and shoulders.
| Lesion | Description |
|---|---|
| Closed comedo (whitehead) | Dilated follicle with no visible opening; keratin/sebum accumulation |
| Open comedo (blackhead) | Dilated follicular opening; dark color due to oxidized lipids + melanin (not dirt) |
| Papule | Small red inflammatory lesion without visible purulent content |
| Pustule | Visible white/yellow purulent content at the surface |
| Nodule | Deeper, larger (>5 mm), firm, painful inflammatory lesion |
| Cyst/abscess | Fluctuant, purulent, deep - may communicate |
| Scar | Atrophic (ice-pick, rolling, boxcar) or hypertrophic/keloid |
Comedones are the hallmark of acne vulgaris and their presence is required for the diagnosis.
7. Acne Variants and Subtypes
7.1 Neonatal Acne
- Presents within the first few weeks of life
- Related to maternal and neonatal androgens
- Typically self-limited
7.2 Infantile Acne
- Presents between 1-12 months of age
- Due to elevated LH stimulating testicular testosterone in infant males; also from neonatal DHEA/DHEAS
- May occasionally require treatment
7.3 Acne Fulminans
- Severe, abrupt-onset systemic form with ulcerative hemorrhagic lesions, fever, arthralgia, leukocytosis
- Can be precipitated by initiating isotretinoin (avoid by starting with low dose + concomitant oral corticosteroids)
- Treatment: isotretinoin + oral corticosteroids; TNF inhibitors, IL-1 antagonists, immunosuppressives (azathioprine, cyclosporine); dapsone if associated erythema nodosum
7.4 Acne Conglobata
- Severe nodulocystic form with coalescent purulent nodules - no systemic manifestations
- Part of the follicular occlusion tetrad: acne conglobata + dissecting cellulitis of scalp + hidradenitis suppurativa + pilonidal sinus
- Associated with PAPA syndrome (pyogenic arthritis, pyoderma gangrenosum, acne conglobata) - autosomal dominant, PSTPIP1 mutations
- Also PAPASH and PASH syndromes
- Treatment: prednisone + low-dose isotretinoin initially
7.5 Solid Facial Edema (Morbihan Disease)
- Unusual complication: woody induration and midline facial/cheek swelling from impaired lymphatic drainage + fibrosis (mast cell-mediated)
- Does not resolve spontaneously
- Treatment: isotretinoin 0.2-1 mg/kg/day for 4-6 months (often 9-24 months required) ± ketotifen or prednisone
7.6 Occupational Acne / Oil Acne / Tar Acne
- Caused by occupational exposure to mineral oils, cutting fluids, or tar products causing comedone formation
8. Grading / Severity Classification
The Global Alliance to Improve Outcomes in Acne proposed a severity grading scheme used as a framework for treatment selection:
| Grade | Description |
|---|---|
| Mild | Predominantly comedonal; few papules/pustules; limited to face |
| Moderate | Mix of comedones, papules, pustules; may involve face + trunk |
| Severe | Many papules/pustules, nodules; extensive; ± trunk involvement |
| Very Severe / Nodulocystic | Nodules, cysts, sinus tracts, scarring; may be systemic |
9. Diagnosis and Laboratory Workup
- Diagnosis is clinical - based on history and physical examination
- Laboratory workup is indicated when hyperandrogenism is suspected:
- Especially in children aged 1-7 (midchildhood acne)
- Serum androgens, LH/FSH ratio, DHEAS, free testosterone
- In females with signs of hyperandrogenism: rule out PCOS, congenital adrenal hyperplasia, adrenal/ovarian tumor
- Bacterial culture if antibiotic-resistant acne or gram-negative folliculitis suspected
10. Treatment
10.1 Cleansing
- Twice-daily washing with a gentle cleanser (syndet preferred - maintains normal skin pH)
- Avoid harsh alkaline soaps that disrupt the cutaneous lipid barrier
- Medicated cleansers (benzoyl peroxide, salicylic acid, sulfur) are useful for hard-to-reach areas (back)
10.2 Topical Medications
Retinoids
- Mechanism: normalize differentiation and proliferation of follicular epithelium → loosen and unseat microcomedones (comedolytic) + anti-inflammatory
- Should be applied to entire acne-prone area once daily; tretinoin applied in the evening (photolabile)
- Beneficial effects not evident for 6-8 weeks or longer; initial apparent exacerbation may occur (externalization of deeper lesions)
| Agent | Key Points |
|---|---|
| Tretinoin | Prototype; available as 0.025%, 0.05%, 0.1% cream/gel; inactivated by UV and benzoyl peroxide (apply separately at night); microsphere formulation (Retin-A Micro) reduces irritancy |
| Adapalene | Synthetic; targets RARγ; photostable; can be used with BPO; 0.1% and 0.3% gels; greater tolerability; 0.1% is OTC-approved for age ≥12 |
| Tazarotene | Potent; 0.1% cream/gel/foam; more effective than tretinoin 0.025% but more irritating; short-contact therapy minimizes irritation; avoid in pregnancy |
| Trifarotene | Newer; comparable efficacy; improved tolerability |
| Topical isotretinoin | Not available in US; works via intraepithelial isomerization to tretinoin; does NOT suppress sebum; less irritating, slightly less effective than tretinoin |
Benzoyl Peroxide (BPO)
- Powerful antimicrobial via free oxygen radical release - reduces C. acnes burden
- Mild comedolytic properties
- Available 2.5-10% in creams, gels, washes, foams
- Key advantage: bacteria cannot develop resistance to BPO → ideal for combination with topical/oral antibiotics
- Can bleach clothing and hair; may cause contact irritation
Topical Antibiotics
- Clindamycin and erythromycin are the most used; erythromycin now limited due to high resistance (~62% global resistance by 1996)
- Always combine with BPO to prevent resistance development
- Topical dapsone 5% and 7.5% gel: alternative with anti-inflammatory properties
Salicylic Acid
- Keratolytic; milder comedolytic; available OTC in washes and leave-on products
10.3 Systemic (Oral) Medications
Oral Antibiotics
- Tetracyclines (doxycycline, minocycline, sarecycline) - first-line systemic antibiotics
- Macrolides (azithromycin, erythromycin) - second-line; increasing resistance
- Trimethoprim-sulfamethoxazole - third-line for resistant cases
- Principles: always combine with topical BPO; limit duration to minimize resistance; not for use as monotherapy; antibiotic resistance in C. acnes is a growing problem
Isotretinoin (Oral)
- Gold standard for severe nodulocystic or recalcitrant acne
- Mechanism: reduces sebaceous gland size and sebum production, normalizes keratinization, reduces C. acnes colonization, anti-inflammatory
- Dose: typically 0.5-1 mg/kg/day; cumulative dose of 120-150 mg/kg often cited for durable remission
- Key adverse effects: teratogenicity (requires iPLEDGE program in US), dry lips/skin/eyes, elevated liver enzymes, hypertriglyceridemia, possible mood effects
- Risk of acne fulminans flare on initiation: start low dose + concomitant corticosteroids in high-risk patients
- ATRA modulates MMP/TIMP balance → matrix preservation (mechanism of scar improvement)
Hormonal Therapy (Women)
- Combined oral contraceptives (OCPs) containing 20-50 mcg ethinyl estradiol: suppress ovarian androgen production via ovulation suppression
- Spironolactone (anti-androgen): blocks androgen receptor in the sebaceous gland; effective for adult female acne
- Cyproterone acetate (available outside US): anti-androgen
10.4 Light and Laser Therapies
- Blue light (415 nm): targets porphyrins produced by C. acnes → bacterial killing
- Red light (633 nm): anti-inflammatory
- PDT (photodynamic therapy) with aminolevulinic acid: targets sebaceous glands
- Lasers (pulsed dye, Nd:YAG): anti-inflammatory, sebaceous gland targeting
- Also used for post-acne scar treatment: CO2 laser, fractional laser resurfacing
10.5 Treatment Algorithm (Summary - Global Alliance Framework)
| Severity | First-Line | Second-Line / Adjuncts |
|---|---|---|
| Mild comedonal | Topical retinoid | Salicylic acid |
| Mild-moderate papulopustular | Topical retinoid + BPO ± topical antibiotic | Oral antibiotic if extensive |
| Moderate-severe papulopustular | Oral antibiotic + topical retinoid + BPO | Switch antibiotic; hormonal therapy in women |
| Severe nodular/conglobate | Oral isotretinoin | Oral corticosteroids for fulminans; hormonal therapy |
| Maintenance | Topical retinoid ± BPO | - |
11. Psychosocial Impact
Acne has an undeniable psychosocial burden. Affected individuals have an increased likelihood of:
- Self-consciousness and social isolation
- Anxiety disorders and depression
- Suicidal ideation
Early, effective treatment is therefore not cosmetic but medically and psychologically necessary.
- Dermatology 2-Volume Set 5e, p. 717
12. Complications
| Complication | Details |
|---|---|
| Scarring | Atrophic (ice-pick, rolling, boxcar) - most common; hypertrophic/keloid in predisposed individuals (more common in darker skin) |
| Post-inflammatory hyperpigmentation (PIH) | Especially common in patients with darker skin tones |
| Solid facial edema (Morbihan disease) | Woody midline facial induration - rare but disfiguring |
| Sinus tracts | In severe conglobata |
| Psychological sequelae | Depression, anxiety, suicidal ideation |
Sources:
- Dermatology, 2-Volume Set, 5th Edition (Griffiths, Barker, Bleiker et al.) - Chapters 35, 36, 126
- Fitzpatrick's Dermatology, Editors Volume 1 & 2 - Chapter 78
Type 4 hypersensitivity
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, well-sourced content from Robbins Pathology, Roitt's Essential Immunology, Goldman-Cecil Medicine, and Cellular & Molecular Immunology - plus two excellent clinical/mechanism diagrams. Let me now compile the full, detailed answer.
Type IV Hypersensitivity (Delayed-Type Hypersensitivity)
1. Definition and Overview
Type IV hypersensitivity - also called delayed-type hypersensitivity (DTH) or cell-mediated hypersensitivity - is the only hypersensitivity type that is not antibody-mediated. It is mediated entirely by antigen-specific T lymphocytes (both CD4+ and CD8+). Because antigen-specific T cells need time to proliferate and secrete cytokines (unlike preformed antibodies), the reaction develops 24-72 hours after antigen exposure in a previously sensitized individual - hence the term "delayed."
The reaction represents an exaggerated interaction between antigen and the normal cell-mediated immune (CMI) mechanism, resulting in tissue-damaging inflammation.
- Roitt's Essential Immunology; Robbins, Cotran & Kumar - Pathologic Basis of Disease
2. Historical Context - The Gell and Coombs Classification
The four hypersensitivity types were classified by Gell and Coombs (1963):
| Type | Name | Mediator | Onset |
|---|---|---|---|
| I | Immediate / Anaphylactic | IgE + mast cells | Minutes |
| II | Cytotoxic / Antibody-dependent | IgG/IgM + complement/ADCC | Hours |
| III | Immune complex | IgG/IgM immune complexes | 6-12 hours |
| IV | Delayed / Cell-mediated | T cells + cytokines | 24-72 hours |
3. Phases of Type IV Hypersensitivity
Type IV reactions occur in two phases:
Phase 1 - Sensitization (Induction Phase)
- On first exposure to an antigen, APCs (dendritic cells, macrophages, Langerhans cells) process and present antigen peptides on MHC class II to naive CD4+ T cells
- The cytokine environment at the time of activation determines T-cell differentiation:
- APCs producing IL-12 → differentiation to Th1 subset
- APCs producing IL-1, IL-6, IL-23 → differentiation to Th17 subset
- IL-2 secreted by activated T cells functions as an autocrine growth factor → T-cell proliferation
- Differentiated effector cells enter the circulation and persist as long-lived memory T cells (years)
Phase 2 - Elicitation (Effector Phase)
-
On re-exposure to the same antigen, memory T cells recognize it and mount a rapid, amplified response
-
This phase develops over 24-72 hours
-
Antigen-specific effector T cells (scarce and taking time to arrive) secrete chemokines that recruit macrophages and other leukocytes to the site
-
The result: tissue inflammation, induration, and potential tissue damage
-
Cellular & Molecular Immunology (Abbas); Robbins Pathology
4. Mechanisms of Tissue Injury
There are three distinct pathways by which Type IV reactions cause tissue damage:
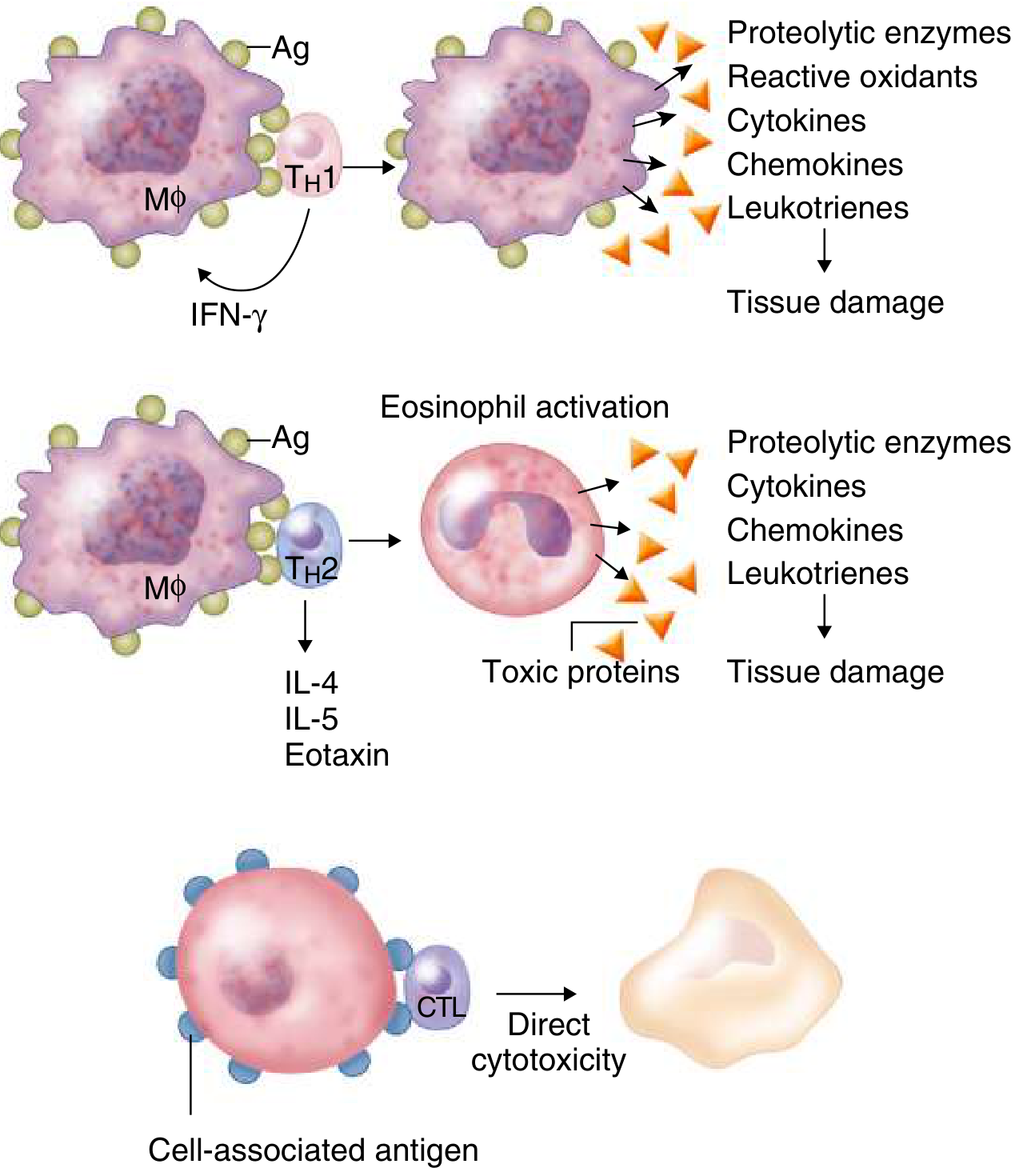
4.1 Th1-Mediated Inflammation (CD4+ - Classic DTH)
The predominant pathway in most type IV reactions:
- Th1 cells recognizing antigen secrete IFN-γ as the primary effector cytokine
- IFN-γ classically activates macrophages ("M1 macrophages"), which:
- Markedly augment phagocytosis and microbial killing
- Express more MHC class II molecules → further antigen presentation
- Produce TNF-α, proteolytic enzymes, reactive oxidants, and leukotrienes
- TNF-α and TNF-β activate endothelial cells, enhance vascular permeability, and damage local tissue
- The result: macrophage-dominated chronic inflammation with potential granuloma formation
4.2 Th17-Mediated Inflammation
- Th17 cells produce IL-17 family cytokines, plus IL-21, IL-22, and GM-CSF
- These cytokines recruit neutrophils (dominant effectors in Th17 responses)
- Orchestrate local inflammation through: pro-inflammatory cytokine/chemokine release, proliferation of effector cells, amplification of Th2-mediated inflammation
- Important in: psoriasis, inflammatory bowel disease, rheumatoid arthritis, multiple sclerosis, SLE, atopic dermatitis, chronic transplant rejection
4.3 Th2-Mediated Inflammation
- Th2 cells produce IL-4, IL-5, and eotaxin
- These recruit and activate eosinophils → eosinophil degranulation → release of toxic proteins, proteolytic enzymes, cytokines, chemokines, and leukotrienes → tissue damage
- The dominant mechanism in chronic asthma and some allergic diseases
4.4 CD8+ T Cell-Mediated Cytotoxicity (CTL Pathway)
- CD8+ cytotoxic T lymphocytes (CTLs) recognize antigen (in context of MHC class I) on target cells
- Destroy target cells via direct cytotoxicity: perforin/granzyme pathway and Fas-FasL pathway
- CD8+ cells also secrete IFN-γ
- Dominant mechanism in: viral infections, drug hypersensitivity reactions (e.g., Stevens-Johnson syndrome/TEN), some autoimmune diseases
5. Timeline of DTH Reaction
| Time After Antigen Challenge | Events |
|---|---|
| 0-4 hours | Initial neutrophil accumulation around postcapillary venules |
| ~12 hours | T cells and blood monocytes infiltrate, organized in perivenular distribution; endothelial cells enlarge; plasma macromolecules leak |
| ~18 hours | Fibrinogen escapes → converts to fibrin; tissue begins to swell and become firm (induration detectable) |
| 24-48 hours | Peak reaction - maximal induration; predominantly mononuclear cell infiltrate (lymphocytes + monocyte-macrophage series) |
| >48-72 hours | Neutrophils migrate out; reaction subsides (in most cases) |
The characteristic histology - perivascular mononuclear cuffing with lymphocytes and macrophages - contrasts sharply with the neutrophil-dominated Arthus reaction (Type III).
- Cellular & Molecular Immunology; Roitt's Essential Immunology
6. Granuloma Formation
When the DTH response is chronic (antigen persists and cannot be cleared, e.g., mycobacteria), activated macrophages accumulate around the antigen and form a granuloma:
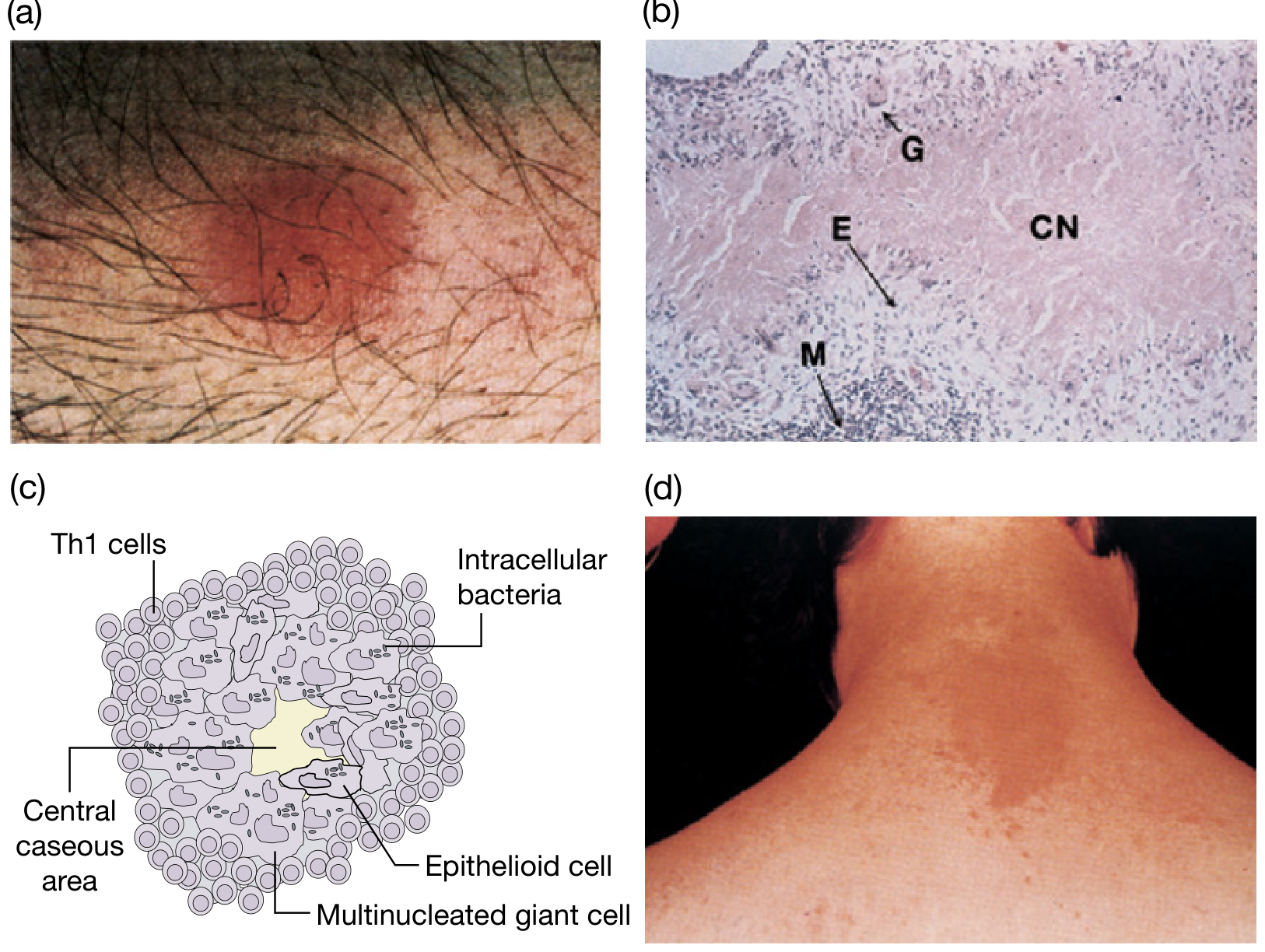
(a) Mantoux test with erythema and induration. (b) Histology of tuberculous granuloma showing caseous necrosis (CN), epithelioid cells (E), giant cells (G), mononuclear cells (M). (c) Granuloma diagram with Th1 cells, epithelioid cells, multinucleated giant cells, central caseous necrosis. (d) Contact dermatitis to nickel.)
Granuloma Structure:
- Central caseous necrosis (in TB; other granulomas may be non-caseating)
- Epithelioid cells - activated, fused macrophages with abundant pale cytoplasm (resemble epithelial cells)
- Langhans/multinucleated giant cells - formed by fusion of epithelioid cells; nuclei arranged in horseshoe or peripheral ring pattern
- Surrounding rim of Th1 lymphocytes
- Outer zone of fibrosis
Granulomas occur in: tuberculosis, leprosy, sarcoidosis, Crohn's disease, fungal infections (histoplasmosis), schistosomiasis, foreign body reactions.
7. Subtypes and Variants
7.1 Classic DTH (Tuberculin-Type)
- Prototype: Mantoux/PPD test (tuberculin skin test)
- Injection of PPD (purified protein derivative of M. tuberculosis) into a previously sensitized individual
- Reaction: erythema + induration appearing after several hours, maximal at 24-48 hours, then subsiding
- A positive test indicates previous or active TB exposure (cell-mediated immunity established)
- Loss of DTH responses to ubiquitous antigens (e.g., Candida, Trichophyton) = anergy → indicator of deficient T-cell function (as in HIV/AIDS)
7.2 Contact Hypersensitivity (Contact Dermatitis)
- Caused by haptens - small chemicals that bind covalently to skin proteins → form complete antigens
- Common sensitizers: nickel, chromium, cobalt (metals), poison ivy/oak (urushiol), rubber chemicals, fragrances, formaldehyde, paraphenylenediamine (hair dye)
- Langerhans cells in the epidermis are the key APCs - they take up the hapten-protein complex and present it to T cells in regional lymph nodes
- Clinical: erythematous, pruritic, vesicular rash at site of contact; may spread beyond contact site
- Jones-Mote (cutaneous basophil) hypersensitivity - a variant with a high proportion of basophils infiltrating the skin lesion (seen with soluble proteins + incomplete Freund's adjuvant; shorter-lasting)
7.3 Granulomatous Hypersensitivity
- Chronic form of DTH due to persistent, non-degradable antigens or poorly soluble particles
- Macrophage activation and fusion → epithelioid cell granulomas
- Examples: TB, leprosy (tuberculoid type), sarcoidosis, Crohn's disease, fungal infections
8. Clinical Examples and Associated Diseases
| Disease / Condition | Antigen Specificity | Mechanism | Key Features |
|---|---|---|---|
| Tuberculin skin test | PPD (M. tuberculosis) | Th1, DTH | Diagnostic test; induration ≥10 mm = positive |
| Contact dermatitis | Nickel, poison ivy, rubber, etc. | Th1/CTL, haptens | Pruritic vesicular eczema at contact site |
| Type 1 Diabetes Mellitus | Pancreatic β-cell antigens (insulin, GAD) | CTL + Th1 | β-cell destruction → insulin deficiency |
| Multiple Sclerosis | Myelin basic protein, other myelin antigens | Th1 + Th17 | Demyelination; relapsing-remitting course |
| Rheumatoid Arthritis | Collagen? Citrullinated proteins? | Th17 + Th1 ± antibodies | Synovial inflammation, joint destruction |
| Inflammatory Bowel Disease | Commensal enteric antigens? Self antigens? | Th17 ± Th1 | Crohn's (transmural, granulomas) or UC |
| Psoriasis | Skin keratinocyte antigens | Th17, IL-17/IL-22 | Plaques with silver scale; Munro microabscesses |
| Transplant rejection | Donor MHC alloantigens | CTL + Th1 | Acute and chronic rejection |
| Graft-vs-Host Disease | Host tissue antigens | Donor T cells (CTL + Th1) | Skin, GI, liver damage after allogeneic BMT |
| Drug hypersensitivity (SJS/TEN) | Drug-modified peptides | CTL-dominant | Widespread keratinocyte apoptosis, mucosal involvement |
| Lepromatous/Tuberculoid leprosy | M. leprae antigens | Th1 (tuberculoid) vs anergy (lepromatous) | Cell-mediated vs humoral response determines type |
| Hashimoto's thyroiditis | Thyroid peroxidase, thyroglobulin | Th1, CTL | Lymphocytic thyroiditis → hypothyroidism |
| Celiac disease | Gliadin (wheat) | Th1 | Villous atrophy in small intestine |
| Sarcoidosis | Unknown antigen | Th1, non-caseating granulomas | Multi-organ; elevated ACE |
- Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goldman-Cecil Medicine; Cellular & Molecular Immunology
9. Key Cytokines in Type IV Hypersensitivity
| Cytokine | Source | Key Function |
|---|---|---|
| IFN-γ | Th1, NK cells, CD8+ | Classical macrophage activation; key DTH mediator |
| TNF-α, TNF-β (LT-α) | Th1, macrophages | Endothelial activation, vascular permeability, local tissue damage |
| IL-2 | Activated T cells | Autocrine T-cell proliferation |
| IL-12 | DCs, macrophages | Drives Th1 differentiation |
| IL-17A/F | Th17 | Neutrophil recruitment; pro-inflammatory |
| IL-21, IL-22 | Th17 | Amplify inflammation; epithelial effects |
| GM-CSF | Th17, T cells | Myeloid cell activation and expansion |
| IL-4, IL-5 | Th2 | Eosinophil recruitment/activation (Th2 variant) |
| Eotaxin | Th2, tissue cells | Eosinophil chemotaxis |
| IL-23 | DCs, macrophages | Maintains Th17 phenotype |
| MCP-1 (CCL2) | Various | Monocyte/macrophage recruitment |
10. Comparison with Other Hypersensitivity Types
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Mediator | IgE | IgG/IgM | Immune complexes | T cells |
| Onset | Minutes | Hours | 6-12 hours | 24-72 hours |
| Complement? | No | Yes | Yes | No |
| Key cell | Mast cell, basophil | NK cells, phagocytes | Neutrophils | Macrophages, T cells, eosinophils |
| Transfer | Serum | Serum | Serum | Cells (not serum) |
| Example | Anaphylaxis | Hemolytic anemia | Serum sickness | Tuberculin test, contact dermatitis |
A key experimental distinction: Type IV hypersensitivity can be transferred passively only with T cells (not serum), whereas Types I-III can be transferred with serum.
11. Diagnosis and Testing
| Test | What It Detects | Example |
|---|---|---|
| Intradermal skin test (Mantoux/PPD) | Prior sensitization to M. tuberculosis | Read at 48-72 hours; induration ≥10 mm positive |
| Patch test | Contact sensitizers (haptens) | Applied for 48 hours; read at 48-96 hours |
| Lymphocyte transformation test (LTT) | Drug-specific T-cell proliferation | In vitro test for drug hypersensitivity |
| Loss of DTH (anergy panel) | T-cell immunodeficiency | Candida, Trichophyton, mumps antigens |
| Skin biopsy | Histology: mononuclear perivascular infiltrate vs neutrophils | Distinguish from Type III (Arthus) |
12. Clinical Significance of Anergy
Loss of DTH responses (anergy) is seen in:
- HIV/AIDS - declining CD4+ T-cell count → loss of recall antigen responses
- Severe malnutrition
- Sarcoidosis (paradoxically - despite systemic granulomas)
- Lymphoma
- Immunosuppressive therapy
Clinically used as a marker of cell-mediated immune competence.
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (p. 206)
- Cellular and Molecular Immunology (Abbas) - Chapter 19
- Roitt's Essential Immunology - Chapter 14
- Goldman-Cecil Medicine - Chapter 36
Psoriasis and lichen planus
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content for both conditions. Let me compile the detailed answer.
Psoriasis and Lichen Planus
PART I — PSORIASIS
1. Definition
Psoriasis is a common, chronic, recalcitrant inflammatory skin disease characterized by discrete plaques with adherent micaceous (silvery) scales occurring at sites of predilection, particularly sites of minor skin trauma. It is a T-cell mediated, immune-driven disease with both genetic and environmental contributors, and is now recognized as a systemic disease in which skin inflammation is the most dramatic manifestation but cardiovascular, metabolic, and articular involvement also occur.
The WHO (2014) recognized psoriasis as a "chronic, noncommunicable, painful, disfiguring and disabling disease for which there is no cure."
- Dermatology 2-Volume Set 5e; Fitzpatrick's Dermatology
2. Historical Note
- Hippocrates grouped dry scaly eruptions under "lopoi" (probably including psoriasis and leprosy)
- The word "psora" was first used by Galen (129-99 BCE) for a scaly skin condition (though this was likely eczema)
- Robert Willan (1809) gave the first accurate description of psoriasis
- Ferdinand Hebra (1841) definitively separated psoriasis from leprosy
- Heinrich Koebner (1879) described development of psoriatic plaques at sites of skin injury - the Koebner phenomenon
3. Epidemiology
-
Prevalence: ~2% of the world's population; in the US and Canada as high as 4.6-4.7%
-
Lower prevalence (0.4-0.7%) in Africans, African-Americans, Norwegian Lapps, and Asians
-
Onset can occur at any age (infancy to eighth decade)
-
Two peaks of onset: 20-30 years (Type I) and 50-60 years (Type II)
-
In ~75% of patients, onset is before age 40; in 35-50%, before age 20
-
Age of onset earlier in women than men; natural history similar - chronic with intermittent remissions
-
Remissions lasting ≥5 years reported in ~15% of patients
-
Psoriatic arthritis affects 5-30% of patients with cutaneous psoriasis
-
73% have mild-moderate disease; 27% severe involvement
-
79% of patients have nail changes
-
Dermatology 2-Volume Set 5e, p. 166; Robbins Pathology
4. Genetic Factors
- Positive family history reported in 35-90% of patients
- Type I psoriasis: onset before age 40, HLA-Cw6 association, more severe, familial
- Type II psoriasis: onset after age 40, no strong HLA association, less severe
- GWAS have linked psoriasis risk to polymorphisms in HLA loci and genes encoding proteins involved in:
- Adaptive immunity
- TNF signaling
- Skin barrier function
- Several loci also associated with psoriatic arthritis
- The concordance among identical twins is high, confirming strong genetic predisposition
5. Pathogenesis
Psoriasis is a T cell-mediated inflammatory disease, presumed to be autoimmune in origin (though the initiating antigens are not defined - may be self antigens, environmental antigens, or both).
The IL-23/Th17 Axis - central to psoriasis:
- Antigen presentation: Dendritic cells (DCs) in the dermis process and present antigens to T cells
- DC activation: Dermal plasmacytoid DCs and myeloid DCs produce TNF-α and IL-23
- IL-23 (heterodimer of IL-23-specific p19 + p40 shared with IL-12) drives Th17 cell development
- Th17 cells produce IL-17, which promotes:
- Neutrophil-predominant inflammation
- Keratinocyte hyperproliferation
- Antimicrobial peptide production (defensins, S100 proteins)
- Th1 cells produce IFN-γ → macrophage activation → further inflammation
- Neutrophils are recruited into the epidermis → form Munro microabscesses in the stratum corneum
- Chemokines (IL-8/CXCL8, CTACK, TARC, MCP-1, RANTES) regulate the complex recruitment of both neutrophils (forming Munro abscesses) and lymphocytes via attachment to endothelial cells and epidermotropism
Evidence for immune origin:
-
Cyclosporine (calcineurin inhibitor) is highly effective → proves T-cell centrality
-
Anti-IL-17 biologics and anti-IL-23 biologics are highly effective
-
Anti-TNF-α antibodies (infliximab) clear psoriasis
-
Fitzpatrick's Dermatology; Robbins Pathology, p. 206; Dermatology 2-Volume Set 5e
6. Triggering Factors
| Trigger | Mechanism |
|---|---|
| Koebner phenomenon | Psoriatic plaques develop at sites of local trauma (scratch, surgery, tattoo) |
| Streptococcal throat infection | Classically triggers guttate psoriasis |
| Stress | Psychogenic exacerbation |
| Medications | Beta-blockers, lithium, antimalarials, NSAIDs, IFN-α, abrupt withdrawal of corticosteroids, TNF-inhibitor discontinuation |
| HIV infection | Paradoxically severe psoriasis |
| Alcohol and smoking | Exacerbate disease |
| Sunburn | Isomorphic response (Koebner) |
7. Clinical Features
7.1 Primary Lesion
The classic lesion is a well-demarcated, erythematous plaque covered by loosely adherent, silvery-white (micaceous) scales.
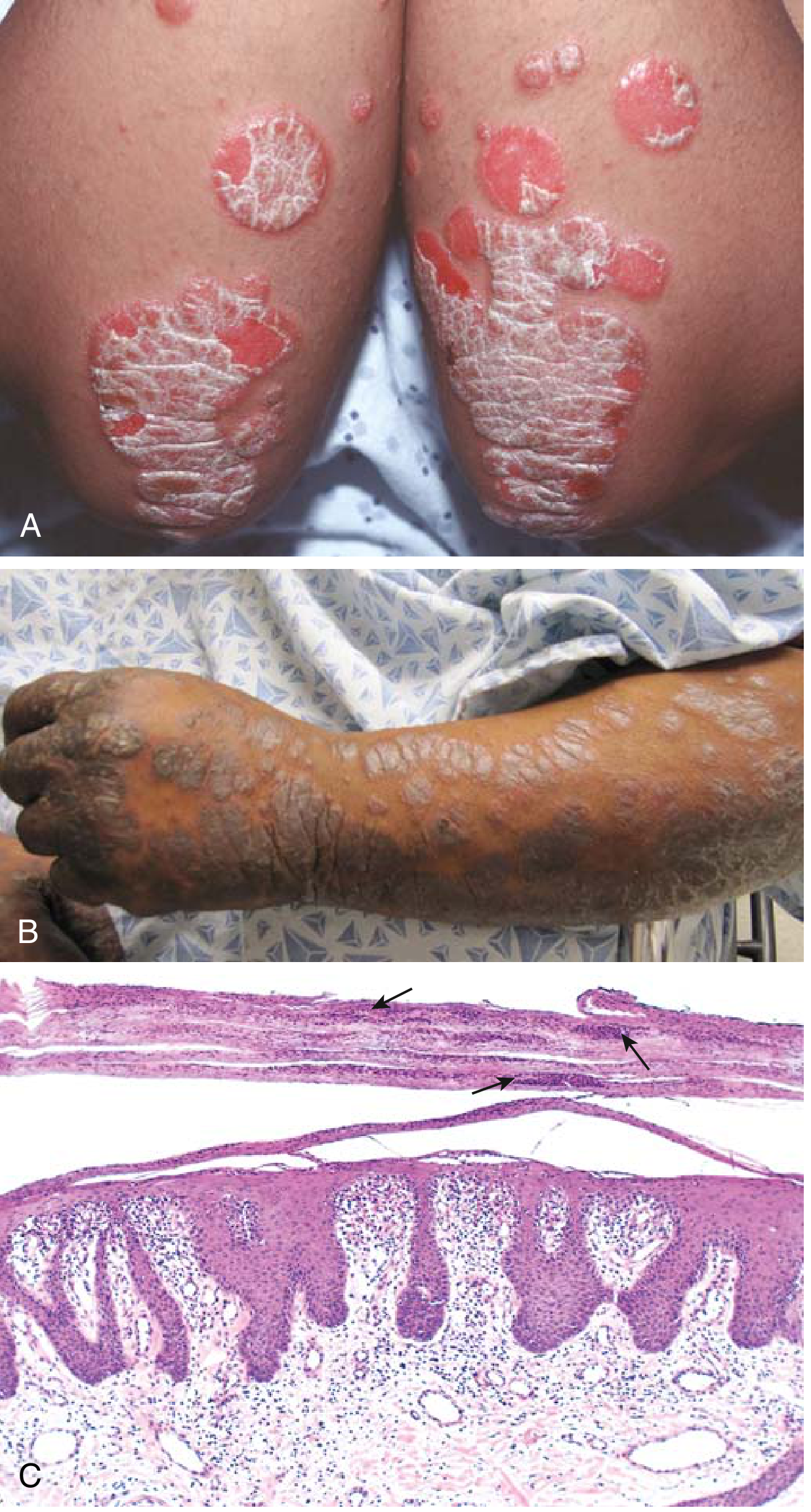
(A) Erythematous psoriatic plaques with silvery-white scale on lighter skin. (B) In darker skin, plaques range from salmon-colored to hyperpigmented with gray scale. (C) Histology showing psoriasiform hyperplasia, parakeratosis, and Munro microabscesses (arrows).
Key clinical signs:
- Auspitz sign: Removal of silvery scales reveals a glistening wet surface with characteristic pinpoint bleeding - this reflects elongated capillary loops in the dermal papillae plus thin suprapapillary epidermis
- Koebner phenomenon (isomorphic response): New plaques appear at sites of skin trauma
- Woronoff's ring: A pale blanching ring surrounding psoriatic lesions
7.2 Sites of Predilection
- Elbows (extensor aspect) - classic
- Knees (extensor aspect) - classic
- Scalp (posterior)
- Lumbosacral area / intergluteal cleft
- Genitalia (up to 45% of patients)
- Palms and soles; nails; umbilicus
7.3 Subtypes / Clinical Forms
| Subtype | Description |
|---|---|
| Chronic plaque psoriasis (psoriasis vulgaris) | Most common (80-90%); symmetric, sharply defined erythematous scaly plaques; chronic and stable |
| Guttate psoriasis | Small (0.5-1.5 cm), drop-like papules scattered over trunk; often in children/young adults post-streptococcal infection; acute onset |
| Inverse (flexural) psoriasis | Smooth, shiny erythematous plaques WITHOUT scale in body folds (axillae, inframammary, groin, intergluteal); scale absent due to moisture |
| Pustular psoriasis | Sterile pustules on erythematous base; generalized (von Zumbusch) = fever, systemic illness; localized (palmoplantar) |
| Erythrodermic psoriasis | Generalized erythema and scaling affecting >90% BSA; medical emergency (thermoregulatory failure, hemodynamic instability) |
| Nail psoriasis | Pitting (most common), onycholysis, oil-drop sign, subungual hyperkeratosis, splinter hemorrhages; in ~79% of patients |
| Scalp psoriasis | Thick adherent scale, often extending beyond hairline ("crown of thorns") |
7.4 Psoriatic Arthritis
Occurs in 5-30% of cutaneous psoriasis patients; in 10-15%, arthritis precedes skin disease.
Five major types (Moll and Wright classification):
| Type | Features |
|---|---|
| Mono/asymmetric oligoarthritis (most common) | DIP and PIP joints; "sausage digit" (dactylitis) from DIP+PIP involvement of one digit |
| DIP joint arthritis | Classic but uncommon; exclusive DIP involvement |
| Rheumatoid arthritis-like | Symmetric polyarthritis; distinguish from RA by RF negativity |
| Arthritis mutilans | Severe, destructive; "pencil-in-cup" deformity; telescoping digits |
| Spondylitis/sacroiliitis | Axial disease; often asymmetric |
Key distinction from RA: Psoriatic arthritis is seronegative (RF usually negative); involves DIPs; associated with nail changes; asymmetric distribution.
8. Histopathology
Three phases - initial, active, and stable:
Initial lesion
- Superficial perivascular lymphocyte/histiocyte infiltrate; papillary edema; dilated capillaries
- Mild acanthosis without parakeratosis; no neutrophils yet
Active lesion (diagnostic)
- Spongiform pustule of Kogoj: Collection of neutrophils within the upper stratum spinosum
- Munro microabscess: Neutrophils/remnants in the stratum corneum surrounded by parakeratosis
- These two are pathognomonic for psoriasis (and AGEP)
- Tortuous, increased capillaries in papillary dermis; edema at papillary tips
- Mixed perivascular infiltrate of lymphocytes, histiocytes, neutrophils
- Parakeratosis (retained nuclei in stratum corneum); absent granular layer (hypogranulosis)
Stable/Chronic lesion
-
Psoriasiform hyperplasia: Marked acanthosis with regular downward elongation of rete ridges ("test tubes in a rack" pattern, "squared-off" rete ridges)
-
Elongated club-shaped dermal papillae with dilated tortuous capillaries extending superficially
-
Thin suprapapillary plate (explains Auspitz sign)
-
Parakeratosis + remnants of Munro microabscess
-
Hypogranulosis (absent granular layer)
-
Predominantly lymphocytic infiltrate
-
Dermatology 2-Volume Set 5e, p. 172; Robbins Pathology
9. Severity Assessment
PASI (Psoriasis Area and Severity Index): Combines body surface area involved (in 4 regions: head, upper extremities, trunk, lower extremities) with clinical grading of erythema, induration, and scaling in each region.
- Mild: PASI <10
- Moderate-Severe: PASI ≥10
10. Treatment
Topical (Mild disease)
| Agent | Mechanism / Notes |
|---|---|
| Corticosteroids | First-line; reduce inflammation; classes I-VII used based on site |
| Vitamin D analogues (calcipotriol/calcitriol) | Inhibit keratinocyte proliferation; combination with corticosteroids synergistic |
| Tazarotene (topical retinoid) | Normalizes keratinocyte differentiation; reduces scale |
| Calcineurin inhibitors (tacrolimus, pimecrolimus) | For sensitive areas (face, flexures); steroid-sparing |
| Anthralin (dithranol) | Historical; anti-proliferative; stains clothing |
| Coal tar | Anti-inflammatory, anti-proliferative; Goeckerman regimen |
| Salicylic acid | Keratolytic; removes scale to enhance penetration of other agents |
Phototherapy (Moderate disease)
- Narrowband UVB (NB-UVB, 311-313 nm): First-line phototherapy; immunosuppressive
- PUVA (psoralen + UVA): More effective than NB-UVB; higher risk of skin cancer
- Excimer laser (308 nm): For localized plaques
Systemic Conventional (Moderate-Severe)
| Drug | Notes |
|---|---|
| Methotrexate | Antifolate; anti-inflammatory; weekly dosing; monitor liver (fibrosis risk); contraindicated in pregnancy |
| Cyclosporine | Calcineurin inhibitor; rapid onset; monitor BP and renal function; limited to short courses |
| Acitretin | Oral retinoid; especially effective for pustular/erythrodermic psoriasis; highly teratogenic |
| Apremilast | PDE4 inhibitor; oral; well-tolerated; modest efficacy |
Biologic Therapies (Moderate-Severe / refractory)
| Drug | Target | Notes |
|---|---|---|
| Infliximab, adalimumab, certolizumab, etanercept | TNF-α | Effective; screen for TB before use |
| Secukinumab, ixekizumab | IL-17A | Highly effective (PASI 90/100 rates); fast onset |
| Bimekizumab | IL-17A + IL-17F | Newer; very high efficacy |
| Ustekinumab | IL-12/23 (p40) | Moderate-high efficacy; q12-weekly dosing |
| Guselkumab, risankizumab, tildrakizumab | IL-23 (p19) | Very high efficacy; selective IL-23 blockade |
JAK Inhibitors (Oral targeted therapy)
- Deucravacitinib (TYK2 inhibitor): FDA-approved for moderate-severe psoriasis
- Brepocitinib (TYK2/JAK1): Under evaluation
PART II — LICHEN PLANUS
1. Definition and Synonym
Lichen planus (LP) (synonym: Lichen ruber planus) is an idiopathic, chronic inflammatory disease of the skin, mucous membranes, hair follicles, and nails. It is the prototype of lichenoid dermatoses - a group of conditions sharing a characteristic lichenoid tissue reaction histologically.
It is a T-cell mediated autoimmune disorder in which CD8+ T cells induce basal keratinocyte apoptosis, with CD4+ Th1 cells driving the inflammatory response.
The term was introduced by Erasmus Wilson in 1869 (previously named "leichen ruber" by Hebra).
- Dermatology 2-Volume Set 5e; Andrews' Diseases of the Skin; Robbins Pathology
2. Epidemiology
- Affects 0.2-1% of the adult population (cutaneous); oral LP up to 1-4%
- Cutaneous LP: 0.3% of men, 0.1% of women; Oral LP: 1.5% of men, 2.3% of women
- No overt racial predisposition; HLA associations include HLA-DR/DQ, HLA-A3
- Gene associations: MTHFR mutations; TNF-α, NRP2, IGFBP4 polymorphisms
- In Europeans: onset primarily after age 20, peak 40-70 years; very rare after age 80
- Childhood LP: 5% or less in Europeans; 10-20% in Indian subcontinent, Arab countries, Mexico
- In the UK, Indians account for 80% of childhood LP
- May be familial in rare cases
3. Etiology and Associations
LP is idiopathic but associated with multiple triggers:
| Association | Notes |
|---|---|
| Hepatitis C virus (HCV) | Strong association; LP may clear with HCV treatment (some conflicting results with newer antivirals) |
| Hepatitis B vaccination | Associated with LP onset; lesions typically appear ~1 month after 2nd vaccine dose |
| Medications (lichenoid drug eruptions) | ACE inhibitors, thiazide diuretics, antimalarials, quinine, gold, NSAIDs, beta-blockers; some with photodistribution |
| Dental materials | Amalgam restorations associated with oral LP |
| Chronic GVHD | LP-like lesions due to alloreactive T cells |
| Immune checkpoint inhibitors (ICIs) | Lichenoid eruptions; managed with topical corticosteroids ± brief drug holiday |
| Thyroid autoimmunity | Personal/family history in up to 30% of vulvar LP; up to 40% have autoantibodies |
| Dyslipidemia / T2DM | LP associated with elevated triglycerides, LDL, insulin resistance, frank T2DM |
4. Pathogenesis
LP is characterized by a Th1 immunologic reaction with CD8+ T-cell predominance at the dermoepidermal junction:
- Basal keratinocytes express altered self-antigens (modified by viral or drug antigens) on their surface
- CD8+ cytotoxic T cells (CTLs) recognize these antigens → induce keratinocyte apoptosis
- CD4+ Th1 cells contribute: increased Th1 cytokine expression (IFN-γ, TNF-α)
- Memory T cells recognize antigen peptides on Langerhans cells or dermal dendritic cells → proliferation and cytokine release
- Th1 cytokines attract and activate macrophages
- Th2 cytokines attract eosinophils (in some variants)
- The LP-like lesions in chronic GVHD (where alloreactive T cells recognize foreign MHC) support the autoimmune hypothesis
5. Clinical Features
5.1 The 6 Ps - Classic Description
"Pruritic, Purple (violaceous), Polygonal, Planar (flat-topped) Papules and Plaques"
5.2 Primary Lesion
- Small, flat-topped, polygonal violaceous papules - almost pathognomonic
- Initial lesions are erythematous; well-developed = violaceous; resolving = hyperpigmented (especially in darker skin)
- Surface: glistening and dry with scant adherent scales
- Wickham striae: Gray or white puncta or streaks on the surface (more easily seen with dermoscopy); represent focal hypergranulosis
- Lesions range from pinpoint papules to 0.5-1.5 cm plaques
5.3 Sites of Predilection
- Flexor wrists (classic)
- Medial thighs, shins, dorsal hands
- Trunk and presacral area
- Genitalia (glans penis - annular lesions; vulva)
- Face: rarely involved (confined to eyelids and lips when present)
- Palms and soles (small papules or hyperkeratotic plaques)
- Lesions are bilateral and relatively symmetric
5.4 Koebner Phenomenon
LP shows the Koebner (isomorphic) phenomenon - new lesions develop at sites of skin injury, similar to psoriasis and vitiligo.
5.5 Pruritus
- Pruritus is often prominent and may precede skin lesions
- May be disproportionately severe relative to the amount of skin involvement
- Patients tend to rub rather than scratch, so scratch marks are usually absent
- Linear LP papules can indicate prior scratching and Koebnerization
5.6 Nail Involvement
Occurs in 5-10% of patients; fingernails > toenails; may be the initial manifestation (especially in children).
- Longitudinal ridging and splitting (most common - 90% of nail LP)
- Onycholysis and subungual debris
- Red lunulae (in ~30%)
- Complete matrix involvement → obliteration of nail plate (anonychia)
- Pterygium unguis - obliteration of the proximal nail fold with forward growth of cuticle fusing with the nail plate; pathognomonic of nail LP
5.7 Oral Mucosa
- Involved in ~70% of cases
- Manifests as white papules with reticulate (netlike/lacelike) pattern - often called "oral Wickham striae"
- Erosive/atrophic and bullous variants also occur
- Oral lesions tend to be chronic and may persist even after skin lesions resolve
- May interfere with food intake in severe cases
5.8 Natural History
- Two-thirds of patients with skin lesions clear within 1 year; many spontaneously clear in the 2nd year
- Hypertrophic and mucosal disease is more chronic
- Recurrences are common, particularly in older patients and those with comorbidities
6. Clinical Variants
| Variant | Key Features |
|---|---|
| Linear LP | Follows lines of Blaschko (not dermatomes as originally thought); more common in children; <1% in Europeans, up to 10% in Japan |
| Annular LP | 3-7% of LP; more common in men (90%); favors axilla, penis/scrotum, groin; ringed lesions ~1 cm; often asymptomatic |
| Hypertrophic LP | Verrucous plaques; anterior shins (most common site); chronic and recalcitrant; "igneous rock sign"; risk of SCC transformation |
| Bullous LP | Vesicles/bullae within LP lesions; distinguish from pemphigoid |
| Ulcerative LP | Painful ulcers on feet (rare); may be associated with cicatricial alopecia |
| Actinic/Subtropical LP | Photo-distributed; upper extremities and face; especially in Middle East, India, Africa |
| LP Pigmentosus | Diffuse dark brown macular pigmentation without typical papules; common in darker skin types |
| Lichen Planopilaris (LPP) | LP of hair follicles → cicatricial (scarring) alopecia; perifollicular erythema and scale; Frontal Fibrosing Alopecia is a variant |
| Vulvovaginal-Gingival LP | Erosive, symptomatic involvement of vulva + vagina + gingival mucosa; risk of scarring/fusion; high SCC risk |
| Blaschkoid LP | Follows Blaschko lines; mosaic pattern |
7. Histopathology
LP is the prototype of interface (lichenoid) dermatitis - inflammation concentrated at the dermoepidermal junction.
Key histological features:
- Dense, band-like (lichenoid) infiltrate of lymphocytes along the dermoepidermal junction - "hugging" the basal layer
- Vacuolar degeneration / liquefaction degeneration of basal keratinocytes
- Colloid bodies (Civatte bodies / cytoid bodies): Anucleate, eosinophilic necrotic basal cells (apoptotic keratinocytes) that drop into the papillary dermis; PAS-positive
- Saw-tooth pattern of rete ridges: The chronic basal cell damage causes the rete ridges to assume an angulated, zigzag contour
- Squamatization of basal layer: Damaged basal cells take on the appearance of spinous layer cells (response to injury)
- Hypergranulosis: Prominent granular layer (in contrast to psoriasis, which shows hypogranulosis)
- Hyperkeratosis (without parakeratosis - in contrast to psoriasis)
- Epidermal hyperplasia (acanthosis) - chronic changes
- "Max Joseph spaces": Small clefts between epidermis and dermis at the tips of some rete ridges
| Feature | Psoriasis | Lichen Planus |
|---|---|---|
| Infiltrate | Neutrophils + T cells, perivascular | Lymphocytic, band-like at DEJ |
| Granular layer | Absent (hypogranulosis) | Prominent (hypergranulosis) |
| Stratum corneum | Parakeratosis (nuclei retained) | Orthokeratosis (no nuclei) |
| Rete ridges | Regular elongation ("test tubes in rack") | Saw-tooth / zigzag |
| Microabscesses | Munro (SC) + Kogoj (spinous) | Civatte bodies (DEJ) |
| Basal layer | Preserved | Vacuolar degeneration |
8. Cancer Risk
- Cutaneous LP alone: Not considered to carry increased cancer risk
- Oral LP: ~1% risk of oral SCC; higher in smokers, alcoholics, HCV-positive patients; occurs in erosive/ulcerative LP, not reticulate
- Majority of oral LP patients who develop SCC develop multiple cancers - close vigilance required
- Vulvar LP: SCC risk up to 3%; regular biopsy of fixed erosive lesions essential
- Hypertrophic LP: Rare SCC on lower legs
- Calcineurin inhibitor use in oral/vulvar LP associated with SCC occurrence (causality not proven; monitoring essential)
9. Treatment
Topical (Mild-Moderate Cutaneous LP)
| Agent | Notes |
|---|---|
| Topical corticosteroids | First-line; superpotent under occlusion for hypertrophic LP; intralesional for nail/hypertrophic LP |
| Topical calcineurin inhibitors (tacrolimus 0.1%, pimecrolimus) | Especially effective for oral LP; symptomatic improvement within 1 month; relapse within weeks on cessation |
| Calcipotriene (calcipotriol) | Equal efficacy to corticosteroids in trials |
| Topical sirolimus | Complete/partial remission in refractory erosive oral LP |
| Antihistamines | For pruritus control |
Systemic (Moderate-Severe LP)
| Agent | Notes |
|---|---|
| Oral prednisone | Effective for acute severe LP; minimum 15-20 mg/day; 2-6 weeks then taper |
| Systemic retinoids (acitretin) | Effective, especially for hypertrophic LP |
| Methotrexate | For recalcitrant/widespread LP |
| Azathioprine | Steroid-sparing |
| Mycophenolate mofetil | For refractory vulvovaginal LP |
| Antimalarials (hydroxychloroquine) | Effective in some LP subtypes |
| NB-UVB / PUVA | Phototherapy for widespread cutaneous LP |
| TNF inhibitors (adalimumab) | Reports of improvement; used in recalcitrant LP |
Therapeutic Ladder (Dermatology 5e):
| Level | Cutaneous | Oral | Scalp (LPP) |
|---|---|---|---|
| Topical | Corticosteroids (superpotent), calcineurin inhibitors, calcipotriene | Corticosteroids (first-line), calcineurin inhibitors | Corticosteroids, calcineurin inhibitors |
| Systemic | Retinoids, MTX, azathioprine, prednisone | Prednisone, MTX, retinoids, antimalarials | Hydroxychloroquine, MTX, retinoids |
10. Side-by-Side Comparison: Psoriasis vs Lichen Planus
| Feature | Psoriasis | Lichen Planus |
|---|---|---|
| Nature | Autoimmune; T-cell mediated | Autoimmune; T-cell (CD8+) mediated |
| Key cytokine axis | IL-23/Th17/IL-17 | Th1/IFN-γ; CD8+ cytotoxic |
| Primary lesion | Erythematous plaque with silver scale | Violaceous, flat-topped, polygonal papule |
| Scale | Thick silvery (micaceous) | Scant, adherent; Wickham striae |
| Koebner phenomenon | Yes | Yes |
| Pruritus | Variable (often mild) | Often prominent; may precede lesions |
| Sites | Extensor (elbows, knees), scalp, sacrum | Flexor (wrists), genitalia, oral mucosa |
| Nails | Pitting, oil-drop, onycholysis | Longitudinal ridging, pterygium |
| Oral involvement | Rare | Common (~70%); reticulate white lesions |
| Arthritis | Yes (psoriatic arthritis in 5-30%) | No |
| Histology - hallmark | Munro microabscess, Kogoj pustule | Civatte bodies, saw-tooth rete ridges |
| Granular layer | Absent (hypogranulosis) | Prominent (hypergranulosis) |
| Parakeratosis | Yes | No (orthokeratosis) |
| Malignancy risk | Increased lymphoma risk (severe/treated) | Oral and vulvar SCC (~1-3%) |
| Natural history | Chronic, relapsing-remitting; rarely remits | 2/3 clear in 1-2 years; mucosal more chronic |
| Systemic disease | Cardiovascular, metabolic syndrome | Dyslipidemia, T2DM, thyroid disease |
Sources:
- Dermatology, 2-Volume Set, 5th Edition (Griffiths/Barker/Bleiker) - Chapters 8, 11
- Fitzpatrick's Dermatology, Volumes 1 & 2 - Chapters 12, 78
- Andrews' Diseases of the Skin - Clinical Dermatology - Chapters 12 (LP), relevant psoriasis sections
- Robbins & Kumar Basic Pathology - Chapter 22
This is a shared conversation. Sign in to Orris to start your own chat.