Enumerate, uh, the viruses, virus causing hepatitis. Name the markers of hepatitis B vi- virus infection. And their interpretation. How is he- hepatitis B virus infection prevented?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from the textbooks to write a full, well-organized answer covering all three questions.
Viruses Causing Hepatitis
At least six viruses are specifically designated as hepatitis viruses. Other viruses (EBV, CMV, yellow fever) can cause incidental liver inflammation, but the primary hepatitis viruses are:
| Virus | Family | Genome | Transmission | Chronicity |
|---|---|---|---|---|
| HAV (Hepatitis A) | Picornaviridae (Hepatovirus) | ssRNA (+) | Fecal-oral | None |
| HBV (Hepatitis B) | Hepadnaviridae | dsDNA (encodes reverse transcriptase) | Parenteral, sexual, perinatal | ~10% adults; ~90% neonates |
| HCV (Hepatitis C) | Flaviviridae | ssRNA (+) | Parenteral, sexual | ~85% |
| HDV (Hepatitis D / Delta) | Deltaviridae | ssRNA (-), circular | Parenteral, sexual (requires HBV) | 50-80% |
| HEV (Hepatitis E) | Hepeviridae (calici-like) | ssRNA (+) | Fecal-oral | Rare (severe in pregnancy) |
| HGV (Hepatitis G / GBV-C) | Flaviviridae | ssRNA | Parenteral | Not associated with clinical disease |
Key distinguishing features:
- HAV and HEV: fecal-oral, acute only, no carrier state
- HBV, HCV, HDV: spread via blood, body fluids, and sexual contact; all can become chronic
- HDV is a defective virus requiring HBsAg from HBV to form its envelope; HBV vaccination prevents HDV
- HCV causes chronicity in ~85% of patients, highest risk for cirrhosis and hepatocellular carcinoma (HCC) after long-term infection
(Sherris & Ryan's Medical Microbiology 8e, p. 479; Medical Microbiology 9e, Ch. 55)
Markers of Hepatitis B Virus Infection and Their Interpretation
The Markers
| Abbreviation | What it is |
|---|---|
| HBsAg | Hepatitis B surface antigen - envelope protein; forms 22 nm spherical and tubular particles in serum in excess; four subdeterminants (adw, ayw, adr, ayr) |
| HBcAg | Core antigen (nucleocapsid); found in nucleus of infected hepatocytes only - NOT detectable in serum directly |
| HBeAg | Glycoprotein associated with the core; best correlate of active viral replication and high infectivity; present only when HBsAg is also present |
| Anti-HBs | Antibody to HBsAg; protective; marker of resolved infection or successful vaccination |
| Anti-HBc (IgM) | Early antibody to core antigen; marker of ACUTE infection; present during the "window period" when HBsAg has cleared but anti-HBs not yet appeared |
| Anti-HBc (IgG) | Persists for life; marker of past or chronic infection; does NOT develop in response to vaccine |
| Anti-HBe | Antibody to HBeAg; appears as HBeAg clears; suggests reduced viral replication and lower infectivity |
(Sherris & Ryan's Medical Microbiology 8e, Table 13-2; Medical Microbiology 9e)
Serology Interpretation by Clinical State
The sequence of marker appearance in acute self-limiting HBV infection:
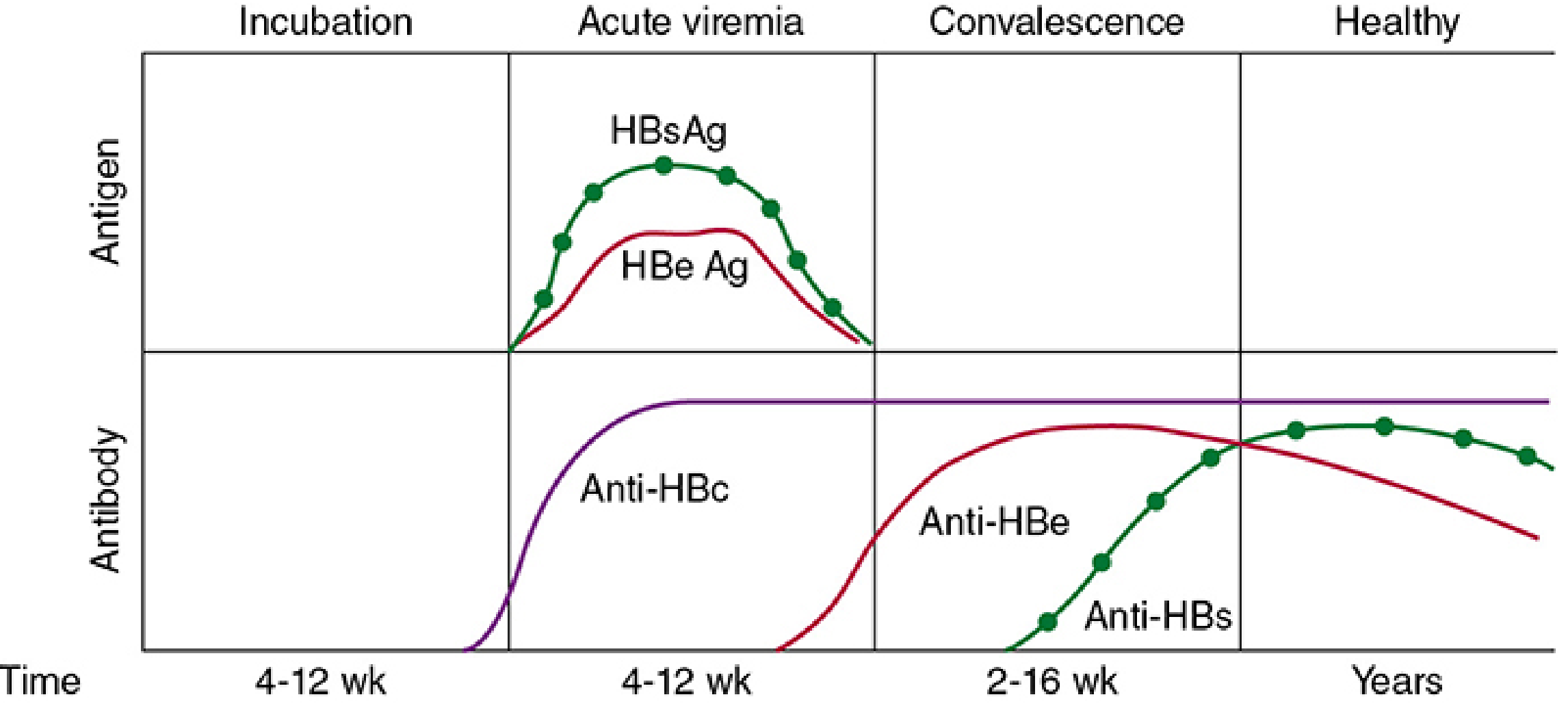
| Clinical State | HBsAg | HBeAg | Anti-HBc | Anti-HBe | Anti-HBs | Interpretation |
|---|---|---|---|---|---|---|
| Early (presymptomatic) | + | - | - | - | - | Earliest detectable marker; active infection |
| Early acute | + | + | - | - | - | Active replication; highly infectious |
| Acute (symptomatic) | + | + | + (IgM) | - | - | Classic acute hepatitis B |
| Window period | - | - | + (IgM) | +/- | - | HBsAg cleared, anti-HBs not yet appeared; only anti-HBc detectable |
| Late acute / Convalescence | + | - | + | +/- | - | HBeAg cleared; resolving |
| Resolved | - | - | + (IgG) | +/- | + | Immunity; past infection |
| Chronic (>6 months HBsAg+) | + | + | + (IgG) | - | - | No anti-HBs; persistent viral replication |
| Vaccinated | - | - | - | - | + | Anti-HBs only (no anti-HBc - key distinction from resolved natural infection) |
(Medical Microbiology 9e, Table 55.2)
Key interpretive rules:
- HBsAg present >6 months + IgG anti-HBc = chronic HBV infection
- IgM anti-HBc = acute infection (also present during window period)
- Anti-HBs alone (no anti-HBc) = vaccination only
- Anti-HBs + IgG anti-HBc = resolved natural infection
- HBeAg = best single marker of infectivity and active replication; its persistence in chronic disease signals ongoing high infectivity
- HBsAg and anti-HBs can never be detected simultaneously (antigen-antibody complexes block detection)
- HBV DNA by PCR is used to quantify viral load, monitor antiviral therapy, and detect occult infection
Prevention of Hepatitis B Virus Infection
Prevention operates at three levels: pre-exposure active immunization, post-exposure prophylaxis, and general infection-control measures.
1. Active Immunization (Vaccine)
- The HBsAg subunit vaccine is the cornerstone of prevention
- Original vaccine: derived from 22-nm HBsAg particles purified from plasma of chronically infected people
- Current recombinant vaccine: the S gene for HBsAg is inserted into yeast (Saccharomyces cerevisiae); the protein self-assembles into virus-like particles (VLPs) with alum adjuvant
- Schedule: three doses at 0, 1, and 6 months - produces protective anti-HBs (IgG)
- Heplisav-B: a newer adult vaccine (age ≥18) combining yeast-derived HBsAg with a CpG-ODN (TLR-9 stimulating) adjuvant - only two doses 1 month apart required, with improved immunogenicity
- Who should be vaccinated: all infants (universal), children, adolescents, and high-risk adults (healthcare workers, IV drug users, people with multiple sexual partners, household contacts of HBsAg carriers, hemodialysis patients, travellers to endemic areas)
- HBV vaccination also prevents HDV (since HDV requires HBsAg to replicate)
2. Post-Exposure Prophylaxis (PEP)
- Hepatitis B Immune Globulin (HBIG): provides passive short-term protection (3-6 months); given within 1 week of exposure
- HBIG + HBV vaccine combination is used for:
- Newborns of HBsAg-positive mothers (given at birth; prevents ~90% of perinatal transmission)
- Healthcare workers after needle-stick exposure to HBsAg-positive blood
- Sexual partners of newly diagnosed HBV cases
- Without intervention, >90% of perinatally infected infants develop chronic infection
3. General Prevention and Infection Control
- Blood supply screening: donated blood is routinely screened for HBsAg and anti-HBc, greatly reducing transfusion-transmitted HBV
- Safe sex practices: condom use reduces sexual transmission
- Harm reduction: avoiding needle sharing among IV drug users
- Universal precautions: gloves, protective clothing, and eye protection when handling blood or body fluids; special care with needles and sharps
- Disinfection: HBV-contaminated materials can be disinfected with 10% bleach; note that unlike most enveloped viruses, HBV is NOT readily inactivated by simple detergents
(Medical Microbiology 9e, Ch. 55; Sherris & Ryan's Medical Microbiology 8e, p. 502)
This is a shared conversation. Sign in to Orris to start your own chat.