Preepiglottic space and it's importance
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content to deliver a thorough answer. Let me compile the response:
Preepiglottic Space (PES)
Anatomy
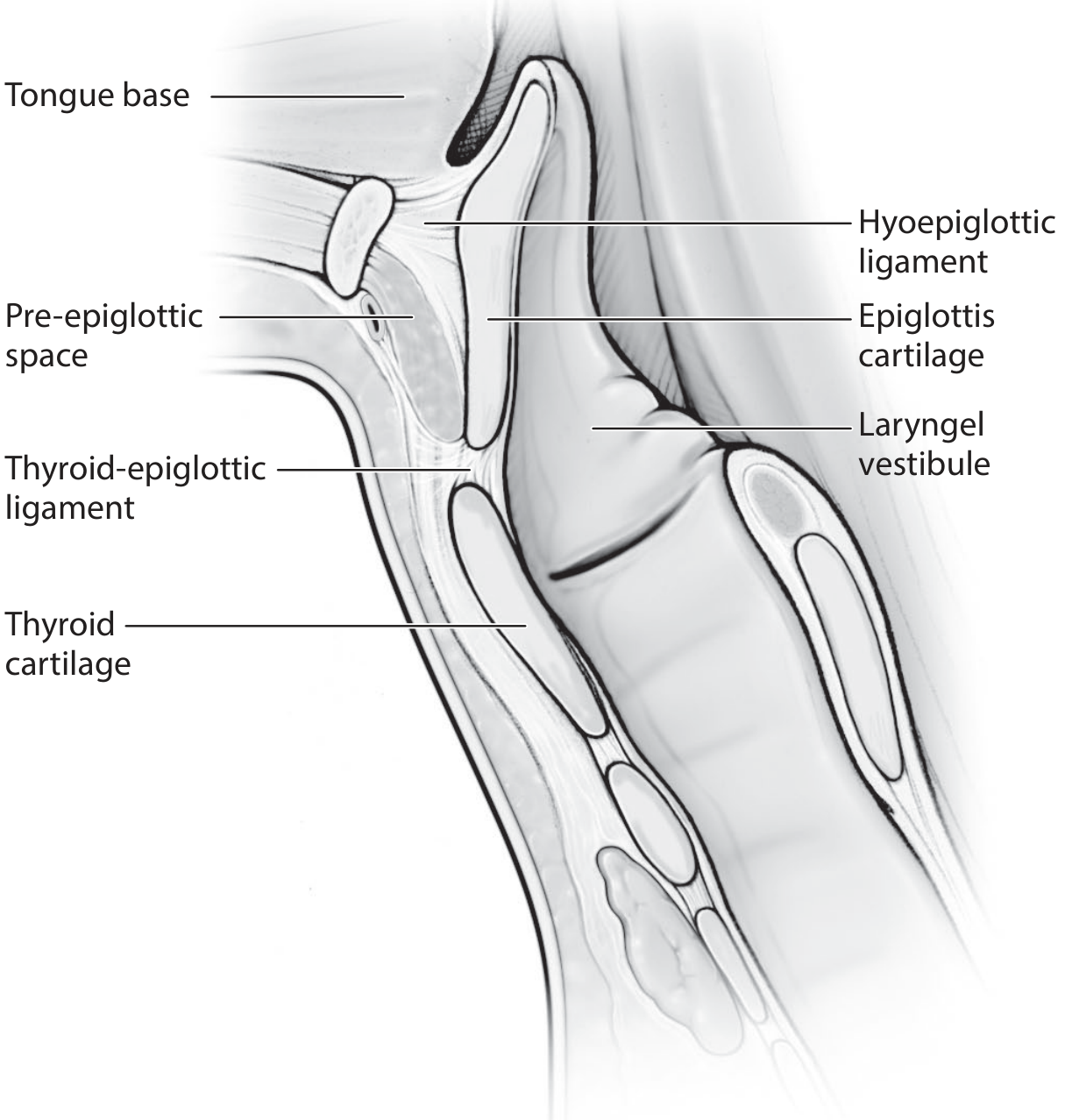
The preepiglottic space is the superiormost space of the larynx. It is filled with fibrofatty tissue traversed by blood vessels and lymphatics.
Boundaries
| Wall | Structure |
|---|---|
| Superior | Hyoepiglottic ligament / vallecular mucosa + hyoid bone |
| Anterior | Thyrohyoid membrane + thyroid cartilage |
| Posterior | Anterior surface of the epiglottis |
| Inferolateral | Thyroepiglottic ligament |
| Posterolateral | Continuous with the superior paraglottic space on each side |
A key anatomical fact: the infrahyoid epiglottis communicates anteriorly with the PES, whereas the suprahyoid epiglottis does not. This distinction drives cancer staging logic.
— KJ Lee's Essential Otolaryngology; Cummings Otolaryngology
Contents
- Fibrofatty tissue (fat-filled)
- Blood vessels and lymphatic channels — clinically significant as these form rich drainage pathways
- The space is contiguous laterally with the paraglottic space, allowing bidirectional tumor spread
Clinical Importance
1. Tumor Spread Pathway
The PES is a critical route for submucosal spread of laryngeal carcinoma:
- Supraglottic tumors overlying epiglottic cartilage have a strong tendency (≈9/10 cases, Kirchner & Carter) to extend into the PES
- Kirchner showed that carcinoma invades PES with a "pushing edge," nearly encapsulated by the elastic membranes of the space — this partly explains the oncologic safety of hyoid-bone preservation during supraglottic surgery
- From PES, tumor can spread to the tongue base (via the hyoepiglottic ligament) and into the paraglottic space → transglottic spread
- The thyrohyoid membrane is thin and, once PES is invaded, extralaryngeal extension becomes possible
2. TNM Staging
PES invasion upstages a supraglottic tumor to T3 (AJCC classification):
T3 supraglottic = vocal fold fixation OR invasion of adjacent structures (postcricoid, pre-epiglottic space, paraglottic space, inner cortex of thyroid cartilage)
A bulge or mass at the thyrohyoid membrane level on clinical examination suggests massive PES invasion.
— KJ Lee's Essential Otolaryngology, p. 820
3. Imaging Assessment
CT or MRI of the neck is used to assess PES invasion, particularly in advanced or radiation-recurrent lesions. Because PES is filled with fat, replacement of the fat signal/density by tumor is readily identifiable on cross-sectional imaging. This directly influences surgical planning.
4. Surgical Implications
| Procedure | Role of PES |
|---|---|
| Supraglottic laryngectomy | Oncologically sound for T1/T2; feasible when PES is not massively invaded |
| SCPL-CHP (Supracricoid partial laryngectomy with cricohyoidopexy) | Indicated when PES is involved — en bloc resection of bilateral paraglottic spaces, entire PES, and thyroid cartilage |
| Contraindication to SCPL | Massive PES involvement with vallecular extension; arytenoid fixation; subglottic extension >10 mm anteriorly |
| Transoral laser microsurgery (TLM) | Contraindicated with massive PES invasion |
The oncologic success of SCPL-CHP is specifically attributed to en bloc resection of the bilateral paraglottic spaces + PES + entire thyroid cartilage.
— Cummings Otolaryngology Head & Neck Surgery
5. Lymphatic Significance
The PES contains significant lymphatic drainage pathways from the supraglottis. This is one reason supraglottic tumors have higher rates of bilateral cervical nodal metastasis compared to glottic tumors:
- T1: 10%, T2: 29%, T3: 38%, T4: ~57% nodal metastasis rates
- Risk of contralateral neck involvement is higher with centrally located/PES-invading tumors
Summary of Key Points
- Location: Anterior to epiglottis, filled with fat and lymphatics; bounded by the hyoepiglottic ligament superiorly, thyrohyoid membrane anteriorly, and epiglottis posteriorly
- Continuity: Contiguous with the paraglottic space — facilitates transglottic spread
- Only infrahyoid epiglottis communicates with PES
- Staging: Invasion = T3 supraglottic disease
- Surgery: PES invasion mandates wider resection (SCPL-CHP over supraglottic laryngectomy); massive invasion with vallecular involvement contraindicates SCPL
- Imaging: Fat replacement on CT/MRI is the diagnostic hallmark
Sources: Cummings Otolaryngology Head & Neck Surgery (9780323612173); KJ Lee's Essential Otolaryngology (9781260122237); Sabiston Textbook of Surgery (9780443124341)
This is a shared conversation. Sign in to Orris to start your own chat.