Tell me about cryptochordism
Reading File
Finding Sources
Searching PubMed
cryptorchidism undescended testis
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks plus visual aids. Let me compile a thorough answer.
Cryptorchidism (Undescended Testis)
Note on spelling: You wrote "cryptochordism" - this likely refers to cryptorchidism (from Greek kryptos = hidden, orchis = testis), also called undescended testis. That's what this answer covers.
Definition
Cryptorchidism is the complete or partial failure of one or both testes to descend into the scrotal sac before birth. It is the most common genital defect in neonatal males.
Epidemiology
| Group | Prevalence |
|---|---|
| Premature male infants | ~30% |
| Full-term male newborns | ~3-5% |
| By 1 year of age (after spontaneous descent) | <1-1.5% |
- Unilateral in ~75% of cases; bilateral in ~25%
- Most commonly the testis arrests in the inguinal canal (most frequent site)
- Intra-abdominal arrest accounts for only ~5-10% of cases
- Robbins, Cotran & Kumar Pathologic Basis of Disease; The Developing Human (Clinically Oriented Embryology)
Embryology & Pathophysiology
Testicular descent occurs in two phases:
-
Transabdominal phase - The testes descend from the posterior abdominal wall to the brim of the pelvis. This is controlled by Mullerian-inhibiting substance (MIS/AMH).
-
Inguinoscrotal phase - The testes pass through the inguinal canal into the scrotum. This phase is androgen-dependent, mediated by androgen-induced release of calcitonin gene-related peptide (CGRP) from the genitofemoral nerve.
Additional molecular regulators include:
- INSL3 (insulin-like 3 gene)
- LGRF8 (relaxin/insulin-like family peptide receptor 2)
- HOX gene family receptors (HOX10)
Failure of any of these processes arrests descent, resulting in cryptorchidism. Androgens are also required to induce regression of the cranial suspensory ligament during the 4th month of gestation. The process is not complete until the third trimester, which explains the high prevalence in premature infants.
- Campbell-Walsh-Wein Urology
Possible Positions of an Undescended or Ectopic Testis
The diagram below shows positions (A = cryptorchid sites numbered 1-4 by frequency; B = ectopic sites):
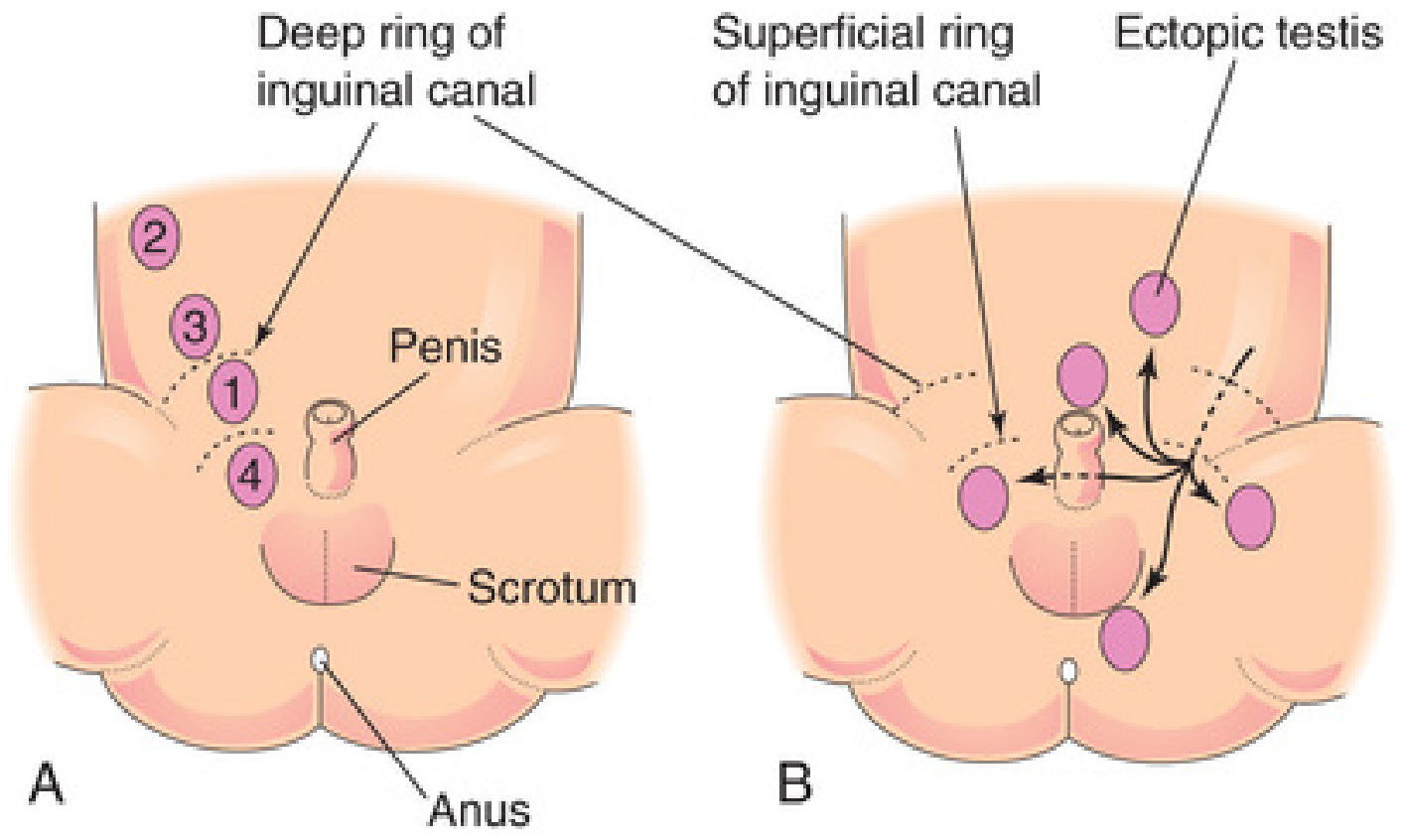
Fig. 12.48 - The Developing Human: Clinically Oriented Embryology
Ectopic testes (deviated from normal descent path) can be found in the:
- Interstitial/superficial inguinal region (most common ectopic site)
- Perineum
- Femoral canal
- Suprapubic region
- Contralateral scrotum
Pathology (Histologic Changes)
Changes begin as early as 2 years of age in the undescended testis:
- Thickening of the basement membrane of seminiferous tubules
- Loss of spermatogonia
- Sertoli cell-only tubules
- Scarred tubules with hyaline connective tissue
- Increased interstitial stroma
- Relative prominence of Leydig cells (relatively spared)
- Germ cell neoplasia in situ (GCNIS) may be present - a likely precursor to germ cell tumors
Importantly, similar histologic changes can occur in the contralateral descended testis in unilateral cryptorchidism, suggesting an underlying intrinsic gonadal developmental defect rather than purely a positional/thermal injury.
- Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
Clinical Features
- Usually asymptomatic - discovered when the scrotal sac is found empty
- Associated with inguinal hernia in 10-20% of cases (due to patent processus vaginalis)
- Risk of crush injury to a testis in the inguinal canal
- Associated conditions: hypospadias, Prader-Willi syndrome, Noonan syndrome
Complications
1. Infertility
- Bilateral cryptorchidism is the more serious fertility risk
- Paternity success rate after orchiopexy: 96% (unilateral) vs 70% (bilateral)
- Inhibin B levels (Sertoli cell/spermatogenesis marker) are significantly lower in bilateral cases (~1/3 of controls) vs unilateral (~2/3 of controls)
- Sperm density is lower even after correction; Leydig cell (testosterone) function is less affected
2. Testicular Cancer
- 4 to 10-fold increased risk of testicular germ cell tumors
- Risk falls to 2-3 fold if orchiopexy is performed prepubertally
- The contralateral normally descended testis is also at elevated malignant risk
- This bilateral risk supports the theory that cryptorchidism reflects an intrinsic (in utero) gonadal dysgenesis - not just a positional thermal insult
- Campbell-Walsh-Wein Urology; Robbins Pathology
Management
Palpable Undescended Testis (e.g., in inguinal canal)
- Standard dartos pouch orchiopexy at 6-12 months of age
- Most inguinal cryptorchid testes that haven't spontaneously descended by 6 months are unlikely to do so
Nonpalpable Undescended Testis
The algorithm below guides management:
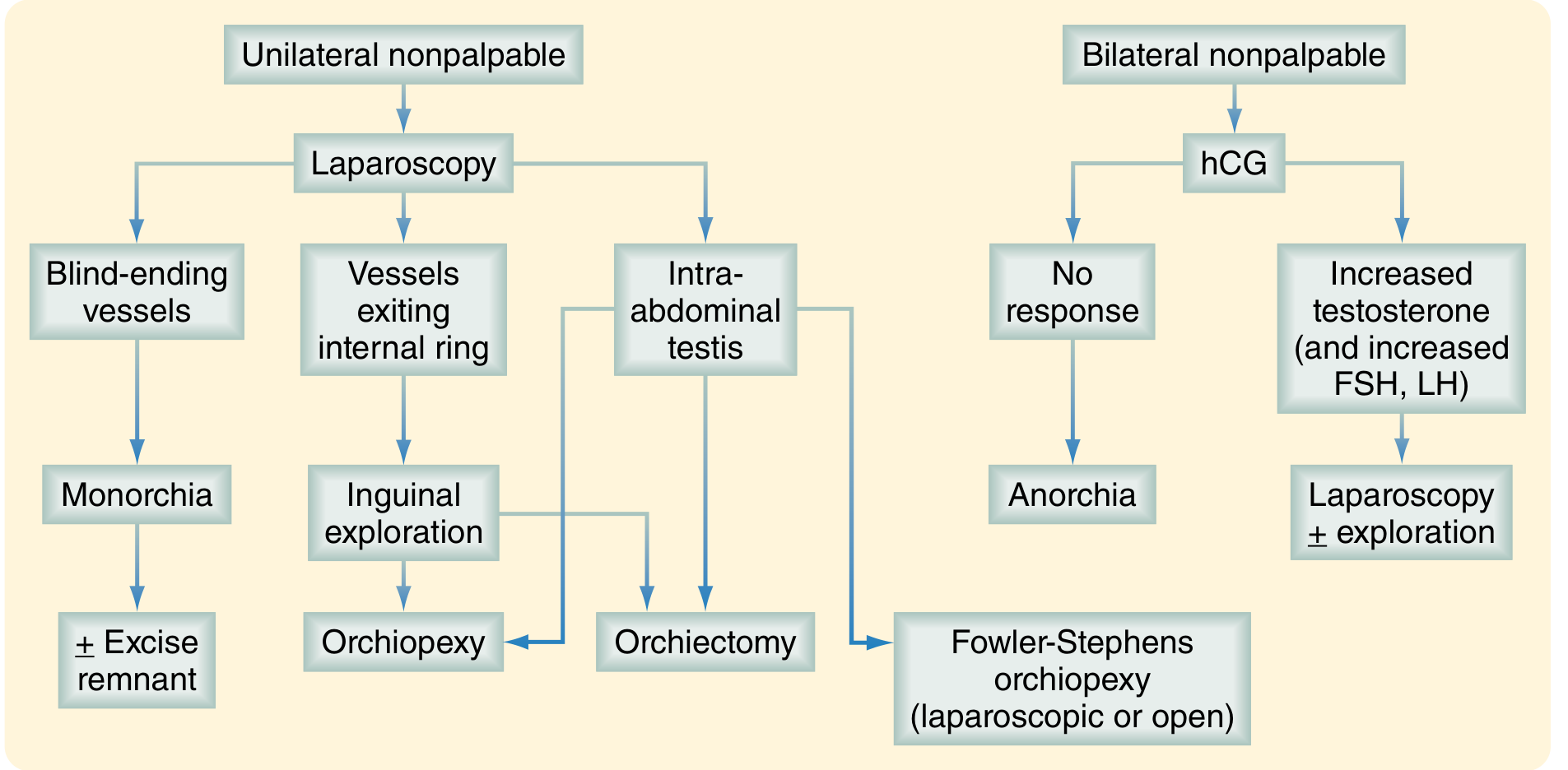
FIGURE 117.20 - Sabiston Textbook of Surgery
Key steps:
- Diagnostic laparoscopy for unilateral nonpalpable testis
- Blind-ending vessels → monorchia (absent testis) → ± excise remnant
- Vessels exiting internal ring → inguinal exploration → orchiopexy
- Intra-abdominal testis → Fowler-Stephens orchiopexy or orchiectomy
- hCG stimulation test for bilateral nonpalpable (to distinguish anorchia from bilateral intra-abdominal testes)
- Two-stage Fowler-Stephens orchiopexy for intra-abdominal testis: ligation of testicular vessels first (stage 1) → allow 6 months for collateral development → orchiopexy (stage 2)
- Laparoscopic orchiopexy has become a popular single-stage option for intra-abdominal testes
Medical (Hormonal) Treatment
- hCG or GnRH injections can be tried before surgery for inguinal/low testes
- Limited efficacy (~15-20% success) and mostly of historical interest now
- Current practice favors early surgical correction
- Sabiston Textbook of Surgery; Campbell-Walsh-Wein Urology
Key Points Summary
| Feature | Detail |
|---|---|
| Prevalence | 3-5% term; 30% preterm; <1.5% by age 1 |
| Most common site of arrest | Inguinal canal |
| Bilateral | ~25% of cases |
| Histologic changes begin | By 2 years of age |
| Fertility risk | Bilateral >> Unilateral |
| Cancer risk | 4-10x increased (falls to 2-3x with prepubertal orchiopexy) |
| Ideal treatment age | 6-12 months |
| Standard surgery | Dartos pouch orchiopexy |
| For intra-abdominal testis | Fowler-Stephens orchiopexy |
Early orchiopexy (by 6-12 months) is recommended to minimize histologic damage and reduce - though not eliminate - the elevated cancer risk. Orchiopexy does not fully restore the cancer risk to baseline, since the underlying gonadal dysgenesis persists.
This is a shared conversation. Sign in to Orris to start your own chat.