Small bowel obstruction according to Bailey and love
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to write a comprehensive answer from Bailey & Love Chapter 78. Here is the full structured response:
Small Bowel Obstruction - Bailey and Love's Short Practice of Surgery (28th Edition, Chapter 78)
Classification
Intestinal obstruction is classified into two types:
- Dynamic (mechanical): peristalsis works against a mechanical obstruction. May be acute or chronic.
- Adynamic: no mechanical obstruction; peristalsis is absent or inadequate (e.g. paralytic ileus, pseudo-obstruction).
Causes of Small Bowel Obstruction
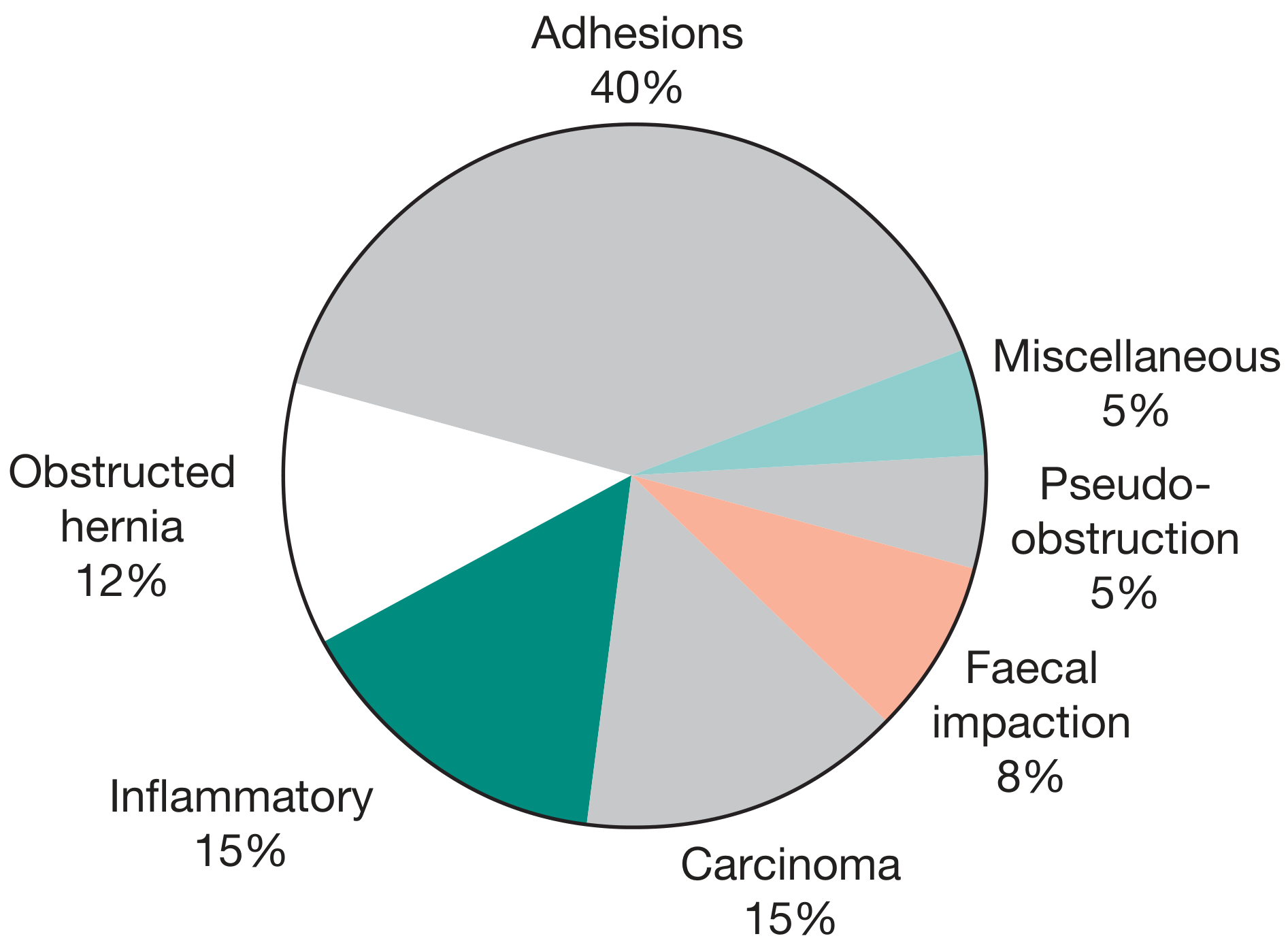
Figure 78.1 - Relative frequencies of causes of intestinal obstruction (Bailey & Love, Ch. 78)
By location of the obstruction:
| Category | Examples |
|---|---|
| Intraluminal | Faecal impaction, foreign bodies, bezoars, gallstones |
| Intramural | Stricture, malignancy, intussusception, volvulus |
| Extramural | Bands/adhesions, hernia |
Adhesions account for ~40% of cases; inflammatory causes (e.g. Crohn's disease) 15%; carcinoma 15%; obstructed hernia 12%; faecal impaction 8%.
Pathophysiology
In mechanical (dynamic) obstruction:
- Bowel proximal to the obstruction dilates; bowel distal empties and collapses.
- Initially, peristalsis increases to overcome obstruction; if unrelieved, the bowel continues to dilate, eventually becoming flaccid and paralysed.
Two main factors cause proximal distension:
- Gas: Bacterial overgrowth produces gas, predominantly nitrogen (90%) and hydrogen sulphide.
- Fluid accumulation: Approximately 3 litres of digestive juice enters the gut per day (saliva 500 mL, bile 500 mL, pancreatic secretions 500 mL, gastric secretions 1 litre). This accumulates as absorption is retarded.
Causes of dehydration and electrolyte loss:
- Reduced oral intake
- Defective intestinal absorption
- Vomiting
- Sequestration in the bowel lumen
- Transudation of fluid into the peritoneal cavity
Strangulation
Strangulation is the most dangerous complication, when the blood supply to the obstructed bowel is compromised.
Causes of strangulation:
| Mechanism | Cause |
|---|---|
| Direct pressure on bowel wall | Hernial orifices, adhesions/bands |
| Interrupted mesenteric blood flow | Volvulus, intussusception |
| Increased intraluminal pressure | Closed-loop obstruction |
The sequence: venous return is compromised first → raised capillary pressure → impaired local perfusion → arterial supply impaired → haemorrhagic infarction. Bacteria and toxins pass through the ischaemic wall into the peritoneal cavity, causing peritonitis.
Cardinal Clinical Features
The four cardinal features of acute intestinal obstruction (Summary box 78.7):
- Abdominal pain
- Distension
- Vomiting
- Absolute constipation
Features vary by level
| Feature | High SBO | Low SBO | Large Bowel |
|---|---|---|---|
| Vomiting | Early, profuse, rapid dehydration | Later, faeculent | Late |
| Distension | Minimal | Central (periumbilical) | Pronounced, early |
| Pain | Predominant, periumbilical | Severe, colicky | Less severe |
| Radiograph | Minimal dilated loops | Multiple dilated loops centrally | Colon distended |
Pain
- First symptom; sudden onset, severe
- Colicky, centred on the umbilicus in small bowel obstruction
- Coincides with peristaltic waves
- As distension increases, colicky pain is replaced by constant diffuse pain
- If obstruction persists without ischaemia, pain may diminish
Vomiting
- In high SBO: immediate, profuse; initially gastric contents, then bile-stained
- In low SBO: delayed and faeculent (reflux of bowel contents)
Distension
- Absent in high obstruction; central/periumbilical in low SBO
- Visible peristalsis ("ladder pattern") may be seen in thin patients
Absolute constipation
- A reliable sign once bowel contents distal to obstruction are evacuated
- NOT present in: Richter's hernia, gallstone ileus, mesenteric vascular occlusion, functional obstruction with pelvic abscess, all partial obstructions (where diarrhoea may occur)
Other Manifestations
- Dehydration: Seen especially in SBO due to repeated vomiting and fluid sequestration. Signs: dry skin/tongue, poor venous filling, sunken eyes, oliguria. Blood urea and haematocrit rise.
- Hypokalaemia: Not common in simple mechanical obstruction. Raised serum potassium, amylase, or lactate dehydrogenase - and leukocytosis or leukopenia - may indicate strangulation.
- Pyrexia: Suggests ischaemia onset, intestinal perforation, or inflammation/abscess from the obstructing disease. Hypothermia indicates septicaemic shock.
- Abdominal tenderness: Localised tenderness = impending ischaemia. Peritonism/peritonitis = infarction/perforation.
Clinical signs of strangulation (Bailey & Love):
- Presence of shock suggests underlying ischaemia
- In impending or established strangulation, pain is never completely absent
- Localised tenderness requires frequent reassessment
- Generalised tenderness and rigidity indicate the need for early laparotomy
- When pain persists despite conservative management, strangulation should be presumed
- In external hernia: lump is tense, tender, irreducible with no expansile cough impulse; erythema or purple discolouration of overlying skin indicates ischaemia
Special Types of Mechanical SBO
Closed-Loop Obstruction
Occurs when both ends of a bowel loop are obstructed (e.g. a band compressing a loop). This is life-threatening because the closed segment cannot decompress proximally. Strangulation risk is high.
Adhesive Intestinal Obstruction
The most common cause. Adhesions form after previous abdominal surgery or peritoneal inflammation. Most resolve with conservative management. Conservative treatment should not be prolonged beyond 72 hours. At operation:
- If a single causative adhesion is found, divide that only
- Multiple adhesions: dissect from duodenojejunal junction to caecum
- Serosal injuries should be repaired or oversewn with absorbable seromuscular sutures
- Laparoscopic adhesiolysis may be considered in highly selected cases but is an advanced procedure
For recurrent obstruction from adhesions, options include: repeat adhesiolysis (enterolysis), Noble's plication, Childs-Phillips transmesenteric plication, or intestinal intubation (the last three are now rarely performed).
Obstruction from Enteric Strictures (Crohn's Disease)
Subacute/chronic presentation. Management: resection and anastomosis to establish histological diagnosis. Strictureplasty may be considered for short multiple strictures in Crohn's disease without active sepsis.
Bolus Obstruction
Causes: gallstones, food, trichobezoar, phytobezoar, stercoliths, worms.
- Gallstone ileus: Elderly patients. A large gallstone erodes through the gallbladder into the duodenum and impacts ~60 cm proximal to the ileocaecal valve. Rigler's triad on AXR: SBO + pneumobilia + ectopic gallstone shadow (pathognomonic when 2 of 3 present, seen in 40-50%). At laparotomy, milk the stone proximally, crush or enterotomy; check for additional stones if faceted. Do not explore the gallbladder region.
- Food bolus: After partial/total gastrectomy. Intraluminal crushing usually successful.
- Bezoars: Trichobezoar (hair) from hair chewing - may indicate psychiatric disorder. Phytobezoar (fruit/vegetable fibre) associated with high fibre intake, previous gastric surgery, hypochlorhydria.
Acute Intussusception
- One bowel segment invaginates into the adjacent segment - invariably proximal into distal.
- Most common in infants aged 5-10 months; 90% idiopathic (hyperplasia of Peyer's patches as initiating event)
- In adults: almost invariably has a lead point (polyp, Peutz-Jeghers, submucosal lipoma)
- Classic presentation in infants: episodes of screaming and drawing up of legs, pale, listless between attacks, vomiting, then "redcurrant jelly" stool (blood and mucus)
- Examination: sausage-shaped lump in right upper abdomen with concavity toward umbilicus, sign of Dance (emptiness in right iliac fossa), blood-stained mucus on PR
Investigations
Blood tests
- FBC: leukocytosis may indicate strangulation
- U&E: assess dehydration and electrolytes
- Raised amylase, lactate dehydrogenase, serum potassium: associated with strangulation
Radiology
Plain AXR (erect and supine):
- SBO: central dilated loops with valvulae conniventes (haustrations absent), air-fluid levels in step-ladder pattern
- Gasless abdomen in strangulated obstruction or proximal high SBO
- Rigler's triad in gallstone ileus
CT scan:
- Now the imaging of choice for diagnosing SBO and identifying the cause
- Can identify site, level, and aetiology
- Can detect strangulation (loss of mural enhancement, mesenteric oedema)
- For intussusception: "target" or "sausage"-shaped soft-tissue mass with layering; diagnostic accuracy 58-100%
Ultrasound:
- High diagnostic sensitivity for intussusception in children (doughnut/concentric ring appearance in transverse section)
Treatment
Three main measures (Summary box 78.11):
- Gastrointestinal drainage via nasogastric tube (NG decompression)
- Fluid and electrolyte replacement (IV resuscitation)
- Relief of obstruction
Surgical treatment is necessary for most cases but should be delayed until resuscitation is complete, provided there is no sign of strangulation or evidence of closed-loop obstruction.
Conservative Management
- NG tube drainage + IV fluid resuscitation
- Appropriate for adhesive SBO where strangulation is excluded
- Should not be continued beyond 72 hours
- Any deterioration, persistent pain, rising inflammatory markers, or failure to resolve = proceed to surgery
Surgical Indications (emergency/urgent laparotomy):
- Signs of strangulation (persistent pain, tenderness, fever, shock)
- Closed-loop obstruction
- Failure of conservative management
- Generalised peritonitis or peritonism
- Irreducible hernia with obstructed bowel
Operative approach:
- Divide causative adhesion(s)
- Assess bowel viability; non-viable bowel must be resected
- Doubtful viability: invaginate with seromuscular suture or resect
- Laparoscopic approach: possible in selected cases by experienced surgeons
Bailey and Love's Short Practice of Surgery, 28th Edition - Chapter 78: Intestinal Obstruction
This is a shared conversation. Sign in to Orris to start your own chat.