Fluoroquinolones in detail for bds 2nd yr with reference to kd tripathi book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the information needed to write a thorough, exam-oriented answer. Note: KD Tripathi's "Essentials of Medical Pharmacology" is not in the library, but the content from Katzung's Basic and Clinical Pharmacology covers the same topics in comparable depth - and I'll frame the answer in KD Tripathi's style (generations, classification, uses relevant to dental practice).
Fluoroquinolones - Detailed Notes for BDS 2nd Year
(Based on Katzung's Basic & Clinical Pharmacology, aligned with KD Tripathi's Essentials of Medical Pharmacology)
1. Introduction
Fluoroquinolones are synthetic, fluorinated analogs of nalidixic acid (a quinolone). Addition of a fluorine atom at position 6 of the quinolone nucleus dramatically expanded their antibacterial spectrum, improved tissue penetration, and allowed systemic use - unlike nalidixic acid, which was limited to urinary tract infections.
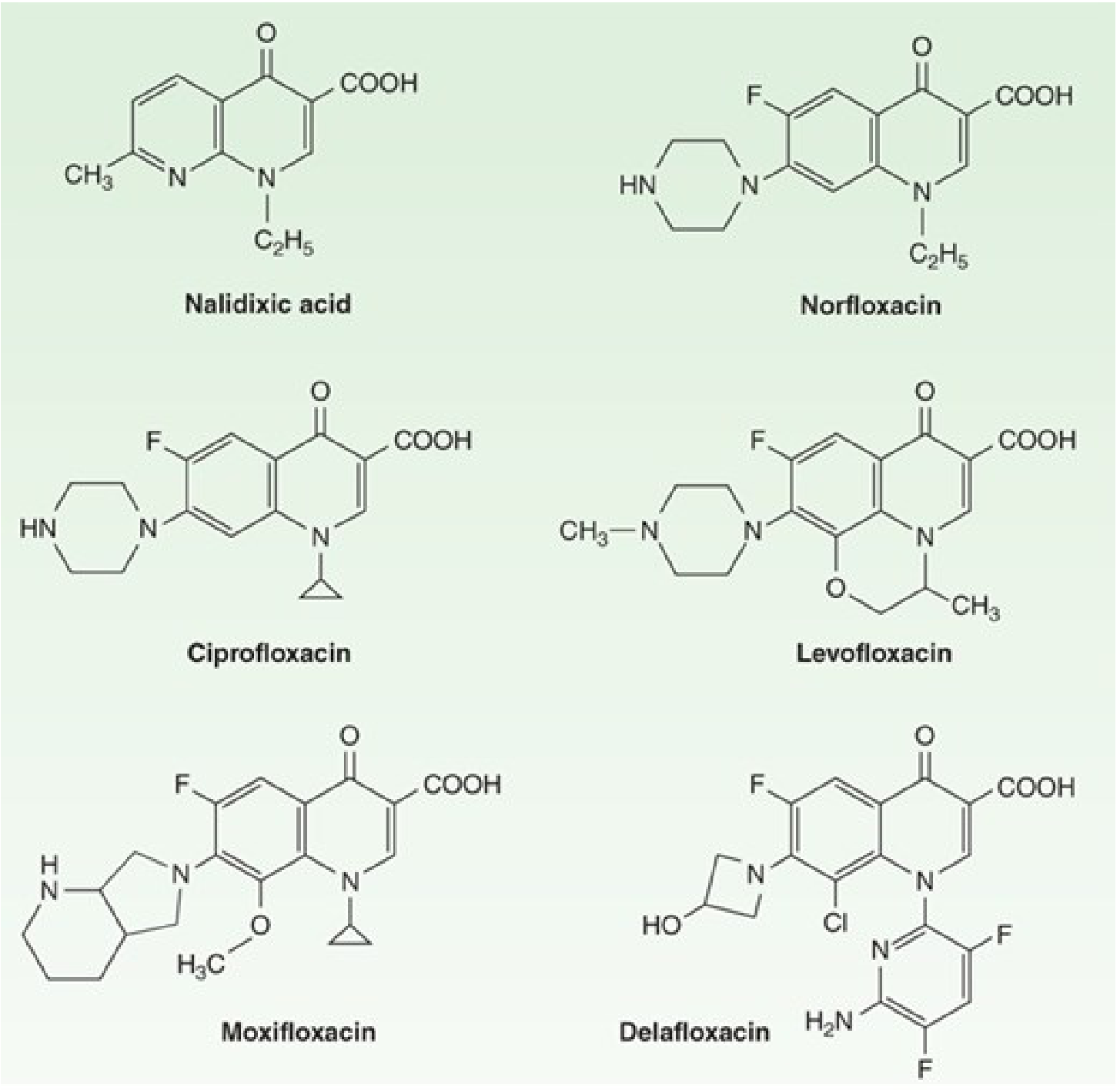
2. Classification (Generations)
KD Tripathi classifies quinolones into generations based on antibacterial spectrum:
| Generation | Drug(s) | Spectrum |
|---|---|---|
| 1st | Nalidixic acid, Cinoxacin | Only gram-negative, urinary tract only |
| 2nd | Norfloxacin, Ciprofloxacin, Ofloxacin, Lomefloxacin | Broad gram-negative, some gram-positive, systemic use |
| 3rd (Respiratory FQs) | Levofloxacin, Sparfloxacin, Gatifloxacin | Enhanced gram-positive + atypical organisms |
| 4th | Moxifloxacin, Gemifloxacin | Broadest spectrum including anaerobes |
- Ciprofloxacin - most potent anti-pseudomonal fluoroquinolone
- Levofloxacin, Moxifloxacin - "respiratory fluoroquinolones," excellent against pneumococci and atypicals
3. Mechanism of Action
Fluoroquinolones are bactericidal. They act by inhibiting two essential bacterial enzymes:
-
DNA gyrase (Topoisomerase II) - primary target in gram-negative bacteria
- DNA gyrase introduces negative supercoils into DNA, relieving tension ahead of the replication fork
- Fluoroquinolones inhibit DNA gyrase → prevent relaxation of positively supercoiled DNA → block DNA transcription and replication
-
Topoisomerase IV - primary target in gram-positive bacteria
- Required for separation (decatenation) of replicated chromosomal DNA into daughter cells
- Inhibition prevents daughter-cell separation → cell death
Mnemonic: "Gyrase for Gram-negatives, topo IV for Gram-positives"
Both enzymes are unique to bacteria (mammalian cells use topoisomerase I and II which are insensitive to quinolones), explaining selective toxicity.
Reference: Katzung Basic & Clinical Pharmacology 16e, Chapter 46
4. Antibacterial Spectrum
| Organism Group | Coverage |
|---|---|
| Gram-negative enteric bacteria | Excellent (E. coli, Klebsiella, Salmonella, Shigella, Proteus, Enterobacter) |
| Pseudomonas aeruginosa | Ciprofloxacin (best), levofloxacin |
| Gram-positive cocci | Variable; 3rd/4th gen > 2nd gen |
| Atypical organisms | Chlamydia, Mycoplasma, Legionella - levofloxacin, moxifloxacin |
| Mycobacteria | Ciprofloxacin, levofloxacin, moxifloxacin (used in MDR-TB) |
| Anaerobes | Moxifloxacin only (among standard FQs) |
| Organisms NOT covered | MRSA, Enterococcus, Bacteroides (except moxifloxacin) |
5. Pharmacokinetics
| Drug | Oral Bioavailability | Half-life (h) | Peak Serum (mcg/mL) | Excretion |
|---|---|---|---|---|
| Ciprofloxacin | 70% | 3-5 | 2.4 | Renal |
| Levofloxacin | 99% | 6-8 | 5.7 | Renal |
| Moxifloxacin | 90% | 9-10 | 3.1 | Hepatic + Renal |
| Norfloxacin | 30-40% | 3-4 | 1.5 | Renal |
| Gemifloxacin | 70% | 8 | - | Renal |
Key pharmacokinetic features:
- Excellent oral bioavailability (except norfloxacin) - widely used orally
- Wide tissue distribution - penetrate well into bone, lung, prostate, CSF (levofloxacin)
- Concentration-dependent killing - efficacy linked to Cmax/MIC and AUC/MIC ratios
- Long half-lives of newer agents allow once-daily dosing (levofloxacin, moxifloxacin)
- Primarily renal excretion (except moxifloxacin which undergoes hepatic metabolism)
- Absorption reduced by antacids, iron, zinc, calcium (chelation - must be given 2 hrs apart)
6. Clinical Uses
General Uses
- UTIs - ciprofloxacin, levofloxacin (not moxifloxacin - low urinary levels)
- Lower respiratory tract infections - "respiratory FQs" (levofloxacin, moxifloxacin, gemifloxacin)
- Traveler's diarrhea / GI infections - ciprofloxacin (Shigella, Salmonella, E. coli, Campylobacter)
- Typhoid fever - ciprofloxacin, ofloxacin
- Soft tissue, bone, joint infections - ciprofloxacin, levofloxacin
- Anthrax prophylaxis and treatment - ciprofloxacin (drug of choice)
- MDR-TB - levofloxacin, moxifloxacin as part of regimens
- Prostatitis - ciprofloxacin, levofloxacin (excellent prostatic penetration)
- Neutropenic fever prophylaxis - ciprofloxacin, levofloxacin
Dental / Oral Surgical Relevance (BDS Focus)
- Orofacial infections not responding to penicillin/metronidazole - ciprofloxacin as alternative (particularly when gram-negative coverage is needed)
- Osteomyelitis of the jaw - ciprofloxacin/levofloxacin (excellent bone penetration)
- Periapical abscess with systemic spread - adjunct when anaerobic-targeted therapy is insufficient; moxifloxacin has anaerobic cover
- Not first-line for routine dental infections (which are predominantly anaerobic/streptococcal - better managed with penicillin + metronidazole)
- Used in immunocompromised patients with odontogenic infections
7. Adverse Effects
Common
- GI disturbances - nausea, vomiting, diarrhea (most common)
- CNS effects - headache, dizziness, insomnia, occasionally seizures (especially in elderly, with NSAIDs)
Serious / Important
| Adverse Effect | Details |
|---|---|
| Cartilage toxicity / Arthropathy | Damages growing cartilage in animal models; avoid in children <18 yrs (avoid in pregnant women); can be used if necessary (e.g., Pseudomonas in cystic fibrosis) |
| Tendinitis / Tendon rupture | Achilles tendon most common; risk ↑ with age, corticosteroids, renal insufficiency; stop drug if tendon pain occurs |
| QT prolongation | Gatifloxacin, levofloxacin, moxifloxacin, gemifloxacin; avoid with Class IA/III antiarrhythmics, hypokalemia, tricyclic antidepressants |
| Photosensitivity | Lomefloxacin, pefloxacin; advise patients to avoid sun exposure |
| CNS excitation / Seizures | Lower seizure threshold; avoid with NSAIDs (synergistic CNS excitation); caution in epileptics |
| Hypoglycemia / Hyperglycemia | Gatifloxacin (withdrawn from USA in 2006 due to this); caution in diabetics |
| Peripheral neuropathy | May be irreversible; FDA black box warning |
| Superinfection | Broad spectrum disrupts normal flora - risk of C. difficile colitis |
FDA Black Box Warnings (Fluoroquinolones)
The FDA has issued black box warnings for:
- Tendinitis and tendon rupture
- Peripheral neuropathy (may be permanent)
- CNS effects
- Exacerbation of myasthenia gravis
- Aortic aneurysm/dissection
8. Drug Interactions
| Drug | Interaction |
|---|---|
| Antacids (Al³⁺, Mg²⁺), Iron, Zinc, Calcium | Chelation → ↓ absorption of fluoroquinolone (give 2 hrs apart) |
| NSAIDs | Additive CNS excitation → seizures |
| Theophylline | Ciprofloxacin inhibits CYP1A2 → ↑ theophylline levels → toxicity |
| Warfarin | Ciprofloxacin inhibits CYP → ↑ anticoagulant effect; monitor INR |
| Class IA/III antiarrhythmics | Additive QT prolongation |
| Sucralfate | Reduces absorption - give 2 hrs apart |
| Corticosteroids | ↑ risk of tendon rupture |
9. Contraindications
- Children and adolescents <18 years (risk of arthropathy; exceptions exist)
- Pregnancy and lactation (cartilage risk to fetus/infant)
- Epilepsy / Seizure disorders (lowers seizure threshold)
- Myasthenia gravis (may worsen neuromuscular blockade)
- Known QT prolongation (with QT-prolonging fluoroquinolones)
- Hypersensitivity to any quinolone
10. Resistance Mechanisms
- Mutation in target enzymes - Altered DNA gyrase (gyrA, gyrB) or topoisomerase IV (parC, parE) genes - most common
- Reduced intracellular accumulation - Efflux pump overexpression (e.g., MexAB-OprM in Pseudomonas); decreased outer membrane permeability (porin mutations)
- Plasmid-mediated resistance - Qnr proteins protect target enzymes; AAC(6')-Ib-cr enzyme modifies certain FQs
11. Summary Table (KD Tripathi Style)
| Feature | Key Point |
|---|---|
| Class | Fluorinated quinolone antibiotics |
| MOA | Inhibit DNA gyrase (gram -ve) and Topoisomerase IV (gram +ve) → bactericidal |
| Spectrum | Broad gram-positive + gram-negative; respiratory FQs cover atypicals and gram+ve |
| Best anti-pseudomonal | Ciprofloxacin |
| Respiratory FQs | Levofloxacin, Moxifloxacin, Gemifloxacin |
| Only FQ with anaerobic cover | Moxifloxacin |
| Drug of choice in anthrax | Ciprofloxacin |
| Absorption interaction | Antacids/iron/zinc chelate → ↓ absorption |
| Enzyme inhibited by ciprofloxacin | CYP1A2 → ↑ theophylline, warfarin levels |
| Avoid in | Children <18, pregnancy, epilepsy, myasthenia gravis |
| Most serious adverse effects | Tendon rupture, QT prolongation, peripheral neuropathy, arthropathy |
| Withdrawn from market | Gatifloxacin (USA, 2006 - glycaemia disturbances) |
Important Points for Dental Students (BDS Exam)
- Fluoroquinolones are concentration-dependent killers (unlike time-dependent beta-lactams)
- Ciprofloxacin is the prototype - excellent gram-negative cover including Pseudomonas
- Moxifloxacin is preferred when anaerobic cover is needed (relevant in polymicrobial dental infections)
- Avoid fluoroquinolones as empirical first-line in dental infections - penicillin + metronidazole remains the standard; FQs are used when patients are penicillin-allergic or infections are severe/refractory
- Tendinopathy is clinically important - advise patients to stop the drug and seek medical help if they develop tendon pain
- Antacids (commonly prescribed alongside antibiotics) significantly reduce FQ absorption - counsel patients on timing
Reference: Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 46 (Quinolones & Fluoroquinolones) - content equivalent to KD Tripathi's Essentials of Medical Pharmacology, Chapter on Quinolones
This is a shared conversation. Sign in to Orris to start your own chat.