Amebiasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"amebiasis"[MeSH Terms] AND ("treatment" OR "management")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to write a thorough response on Amebiasis. Let me compile it:
Amebiasis
Definition
Amebiasis is infection caused by the enteric protozoan parasite Entamoeba histolytica. It can manifest as asymptomatic colonization, diarrhea, dysentery, colitis, or spread extraintestinally to cause liver abscess and, rarely, brain abscess. - Goldman-Cecil Medicine
The Pathogen
E. histolytica has a low infectious dose (<100 organisms), is resistant to chlorine, and is environmentally stable. It has two morphologic forms:
| Feature | Trophozoite | Cyst |
|---|---|---|
| Role | Tissue invasion (pathogenic form) | Transmission (infective form) |
| Survival | Degenerates rapidly outside the body; destroyed by gastric acid | Environmentally stable; resistant to chlorination |
| Nuclei | 1 | 1-4 (mature = 4) |
| Size | 12-50 µm | 10-20 µm |
| Chromatoidal bars | N/A | Rounded ends (vs. E. coli's splintered ends) |
| Karyosome | Central, sharp | Central, sharp |
| Ingested RBCs | Present (pathognomonic) | Absent |
The tissue-destructive properties give the organism its name "histolytica." Certain genotypes are linked to colonization, while others drive invasion. - Medical Microbiology 9e
Related species (morphologically identical but non-pathogenic): E. dispar, E. moshkovskii, E. bangladeshi - these cannot be distinguished by microscopy alone but do not cause invasive disease.
Trichrome-stained stool showing E. histolytica cyst (CDC/Dr. Mae Melvin):
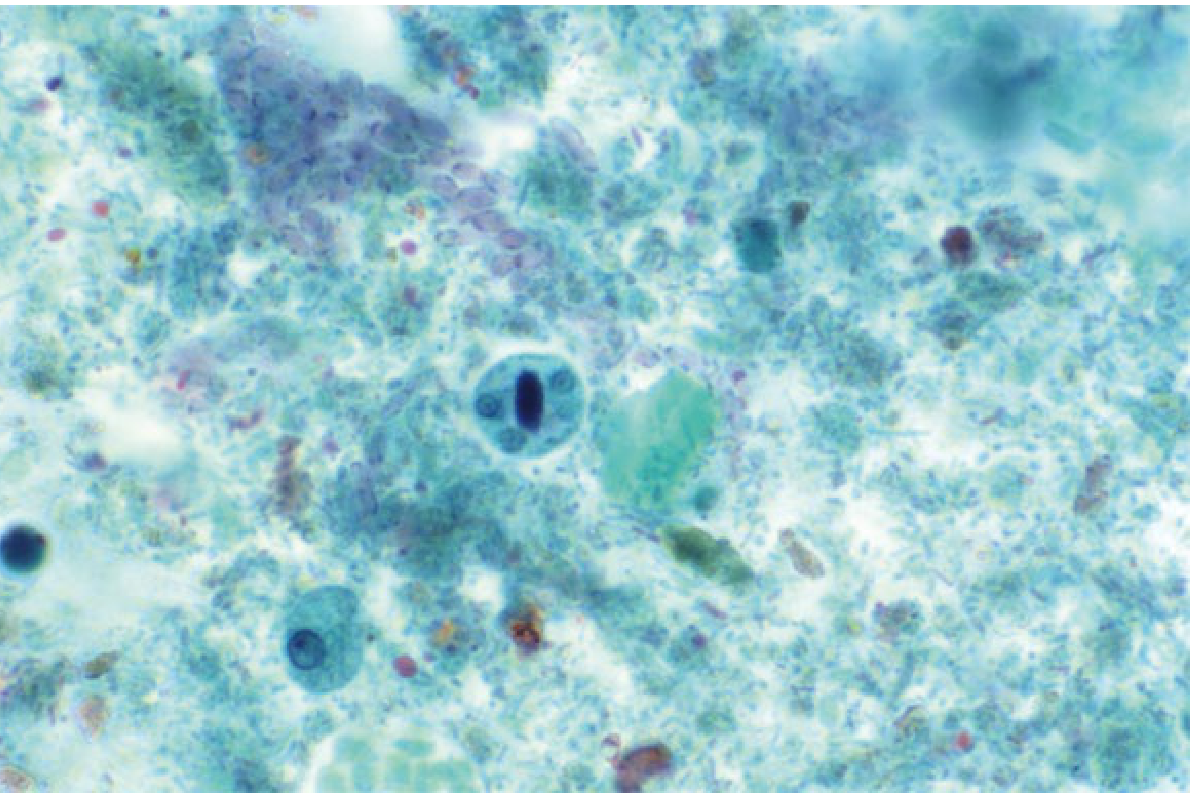
The mature cyst in the center displays an oblong chromatoid body and four nuclei (9-25 µm diameter) each with a centrally situated karyosome. - Yamada's Textbook of Gastroenterology
Life Cycle
- Ingestion of cysts from fecally contaminated food/water
- Excystation in the duodenum (stimulated by gastric acid) - each quadrinucleate cyst yields 8 trophozoites
- Trophozoites colonize the large intestine; multiply by binary fission
- In the colon, trophozoites can encyst - cysts are shed in feces
- Invasive trophozoites penetrate the mucosa, enter the portal circulation, and reach the liver (most common extraintestinal site)
Humans are the only host; natural infection of primates also documented. - Yamada's Textbook of Gastroenterology
Epidemiology
- WHO estimate: ~50 million symptomatic cases and ~100,000 deaths annually worldwide
- Endemic in the Indian subcontinent, Southeast Asia, sub-Saharan Africa, Central and South America
- In the US: 3rd most common parasitic infection (after giardiasis and cryptosporidiosis); rate 1.2/100,000
- 2nd most common cause of diarrhea in returning travelers
- High-risk groups: young children, elderly, malnourished, pregnant women, corticosteroid users
- Typical amebic liver abscess patient in the US: 20- to 40-year-old Hispanic male immigrant
- Transmitted by fecal-oral route; flies and cockroaches can serve as mechanical vectors - Goldman-Cecil Medicine
Pathogenesis
Host cell killing occurs via a sequential process:
- Adherence - via the Gal/GalNAc lectin (galactose- and N-acetyl-D-galactosamine-specific), which binds host intestinal epithelium
- Amebic trogytosis - a nibbling-like process
- Contact-dependent cytotoxicity - trophozoites induce apoptosis in host cells by activating caspase-3; caspase-3-deficient mice are resistant
- Phagocytosis of host cell corpse - requires recognition via multiple ligands (Gal/GalNAc lectin, phosphatidylserine receptor, SREHP, collectins)
- Cysteine proteinases (>44 genes) - degrade colonic mucin, extracellular matrix, hemoglobin, and inactivate IL-18
- Flask-shaped ulcerations form in the intestinal mucosa with hemorrhage and potential secondary bacterial infection
Immune response:
- Innate: lymphoid type-2 cells, neutrophils (within 1-2 days), macrophages/T cells (by day 3)
- Acquired: protective IFN-γ response; mucosal IgA against Gal/GalNAc lectin - children with anti-lectin IgA have 86% fewer new infections
- TH2 response (IL-4) is deleterious; TH1 (IFN-γ) is protective
- The IL-33/ILC2 pathway is an important host defense mechanism
Clinical Syndromes
1. Asymptomatic Carriage
Most infections (especially with E. dispar/moshkovskii) are asymptomatic. Carriers pass infectious cysts and are the main reservoir.
2. Amebic Colitis (Intestinal Amebiasis)
- Gradual onset over 1-3 weeks
- Bloody diarrhea, mucus in stool, crampy abdominal pain
- Fever is present in <40% of cases (distinguishes it from bacillary dysentery, which more often has high fever)
- Severe disease: fulminant colitis (1-4%) with toxic megacolon - high mortality; corticosteroids dramatically worsen this
- Ameboma: inflammatory mass (usually cecum or ascending colon) that can mimic carcinoma
3. Amebic Liver Abscess (ALA) - Most Common Extraintestinal Form
- Right lobe involved in >80% of cases
- Presents with fever, right upper quadrant pain, and hepatomegaly with elevation of the right hemidiaphragm
- "Chocolate sauce" (anchovy paste) pus on aspiration - odorless, acellular necrotic debris
- Only ~30% have concurrent intestinal symptoms; stool examination is often negative
- Serology is positive in virtually all patients with ALA
- Rarely: rupture into pleural space, pericardium, or peritoneum
4. Other Extraintestinal Sites
- Pleuropulmonary (via diaphragm from liver abscess): most common after ALA
- Brain abscess: rare but high mortality
- Cutaneous/genital amebiasis: direct contact with infected material
Diagnosis
Stool Microscopy
- Detection of trophozoites or cysts in stool
- Trophozoites with ingested RBCs are pathognomonic
- Must be distinguished from commensal amebae (see table above) and from PMNs
- Sensitivity is low: parasites are not homogeneously distributed; multiple specimens (3) increase yield
- Cannot distinguish E. histolytica from E. dispar/moshkovskii by morphology alone
Antigen Detection (Fecal ELISA)
- Detects E. histolytica-specific antigen (Gal/GalNAc lectin)
- Differentiates pathogenic from non-pathogenic species
- More sensitive and specific than microscopy
PCR / DNA Probes
- Most specific method for distinguishing E. histolytica from look-alike species
- Increasingly available commercially
Serology (Anti-amebic antibodies)
- Positive in >80% of intestinal amebiasis and virtually all ALA cases
- Less useful in endemic areas (background seropositivity)
- IgG remains positive for years - cannot distinguish active from past infection
Imaging (for ALA)
- Ultrasound: first-line - shows hypoechoic lesion, usually right lobe
- CT/MRI: better characterization; single round lesion with peripheral enhancement
- Aspiration: "chocolate pus" without organisms (amebae are at abscess margin, not center)
Treatment
Treatment depends on clinical form. - Katzung's Basic and Clinical Pharmacology
| Clinical Setting | Drug of Choice | Alternative |
|---|---|---|
| Asymptomatic intestinal infection | Luminal agent only: Paromomycin 10 mg/kg TID × 7 days OR Diloxanide furoate 500 mg TID × 10 days OR Iodoquinol 650 mg TID × 21 days | - |
| Mild-to-moderate colitis | Metronidazole 750 mg TID (or 500 mg IV q6h) × 10 days PLUS luminal agent OR Tinidazole 2 g/day × 3 days + luminal agent | Luminal agent + Tetracycline 250 mg TID × 10 days OR Erythromycin 500 mg QID × 10 days |
| Severe colitis/dysentery | Metronidazole 750 mg TID × 10 days OR Tinidazole 2 g/day × 3 days PLUS luminal agent | Luminal agent + Tetracycline 250 mg TID × 10 days |
| Liver abscess / ameboma / extraintestinal | Metronidazole 750 mg TID × 10 days OR Tinidazole 2 g/day × 5 days PLUS luminal agent | Chloroquine 500 mg BID × 2 days then 500 mg/day × 21 days + luminal agent |
Key principles:
- A luminal agent is always required after tissue amebicide therapy (to eradicate residual intestinal cysts and prevent relapse)
- Luminal agents alone (paromomycin, diloxanide, iodoquinol) are NOT effective against extraintestinal disease
- Asymptomatic carriers in non-endemic areas should be treated with a luminal amebicide
- Percutaneous aspiration of ALA is reserved for: large or left-lobe abscesses (risk of rupture into pericardium), failure to respond to metronidazole in 3-5 days, or bacterially superinfected abscess
Prevention and Control
- Safe water supply (boiling, iodination - NOT chlorination alone, since cysts are chlorine-resistant)
- Improved sanitation and fecal disposal
- Hand hygiene and food safety
- Avoid raw produce washed with contaminated water when traveling to endemic areas
- Screening and treatment of cyst-passers in food-handling or institutional settings
Sources: Goldman-Cecil Medicine | Medical Microbiology 9e | Yamada's Textbook of Gastroenterology | Katzung's Basic and Clinical Pharmacology, 16th ed.
Recent literature note: A 2025 systematic review on cerebral amebiasis (PMID 40602053) highlights that rapid PCR-based diagnostics significantly improve outcomes in the rare but lethal CNS form of this disease. No recent meta-analyses challenge current first-line metronidazole-based management.
Tb ulcer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I have rich content now. Let me compile the comprehensive answer covering both the surgical (cutaneous/external) TB ulcer and the intestinal TB ulcer.
Tuberculous (TB) Ulcer
TB ulcers arise in two main clinical contexts: (1) external/cutaneous TB ulcer - from rupture of a caseous lymph node or cold abscess, and (2) intestinal TB ulcer - from direct mucosal invasion by Mycobacterium tuberculosis. Both are discussed below.
PART 1 - External (Cutaneous) Tuberculous Ulcer
Pathogenesis
The external TB ulcer most commonly results from the bursting of a caseous lymph node onto the skin surface, or from a cold abscess (from bone/joint TB) tracking to and breaking through the skin. The sites of predilection follow the regional lymph node groups: neck > axilla > groin. - S Das, Manual on Clinical Surgery
Classic Features of a TB Ulcer
Characteristic ulcer edge diagram from Bailey & Love's Surgery:
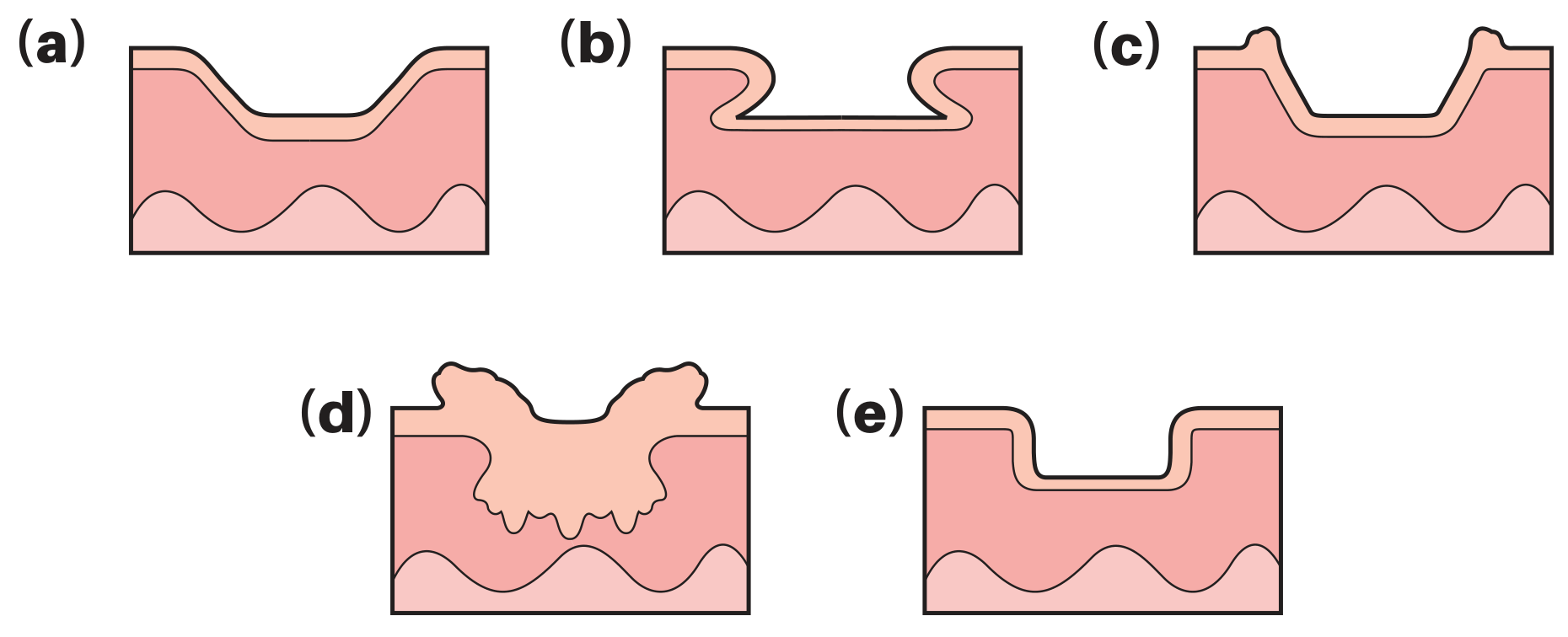
(b) in the diagram shows the pathognomonic undermined edge of a tuberculous ulcer.
| Feature | Description |
|---|---|
| Site | Neck, axilla, groin (lymph node areas); also scrotum (from tuberculous epididymitis) |
| Edge | Thin, bluish-red, and undermined - the hallmark feature |
| Floor | Pale granulation tissue ("wash-leather" granulations) |
| Discharge | Scanty, serosanguineous; thin and watery |
| Base | Slight induration (indicates chronicity) |
| Pain | Slightly painful (less painful than acute septic ulcer) |
| Regional lymph nodes | Enlarged, non-tender, matted (due to underlying TB lymphadenitis) |
Clinical photo of a cervical tuberculous ulcer (Bailey & Love's Surgery):

Tongue TB Ulcer
On the tongue, the TB ulcer is shallow, often multiple, greyish-yellow with a slightly red undermining margin. These typically result from contamination with infected sputum. - S Das
Key Differential: TB Ulcer vs. Other Ulcer Types
| Type | Edge | Floor | Base | Discharge |
|---|---|---|---|---|
| TB ulcer | Thin, bluish, undermined | Pale granulations | Slightly indurated | Serosanguineous |
| Non-specific (pyogenic) | Shelving/sloping | Granulation tissue | Soft | Purulent |
| Syphilitic (chancre) | Punched-out | Wash-leather slough | Hard, indurated ("button") | Serous |
| Basal cell carcinoma | Rolled, pearly | - | - | Minimal |
| Squamous cell carcinoma | Everted/heaped-up | Irregular | Hard | Variable |
Lupus Vulgaris (Cutaneous TB)
A special form - occurs commonly on the face and hands in children and young adults. Starts as single/multiple cutaneous nodules that ulcerate superficially. Active at the periphery (spreads outward) while healing centrally. The name "lupus" (wolf) refers to its peripheral destructive nature. Squamous cell carcinoma can develop from the scar of lupus vulgaris (Marjolin's ulcer). - S Das
Investigations
- Discharge microscopy: Acid-fast bacilli (ZN stain); guinea pig inoculation test
- Mantoux test (TST) or IGRA (Interferon-gamma release assay) - supersedes Mantoux in endemic areas
- Raised ESR and CRP, low haemoglobin
- Excision biopsy of lymph node (if in adenitis stage) - sent fresh to lab
- Aspiration of cold abscess for culture and sensitivity (ZN stain)
- Chest X-ray - to identify pulmonary focus
- Sputum for culture and ZN staining - Bailey & Love's Surgery
PART 2 - Intestinal Tuberculous Ulcer
Pathogenesis & Location
- Organism: usually Mycobacterium tuberculosis; occasionally M. bovis (from contaminated dairy)
- Route: direct penetration of intestinal mucosa by swallowed organisms in sputum or contaminated food
- Ileum and cecum are most commonly involved (75% of cases)
- Both sides of the ileocecal valve are typically affected - causing valve incompetence (a key feature distinguishing TB from Crohn's disease, which does not usually involve the valve)
Gross Morphology - Three Types
| Type | Frequency | Description |
|---|---|---|
| Ulcerative | 60% | Multiple superficial lesions confined to the epithelial surface |
| Hypertrophic | 10% | Scarring, fibrosis, heaped-up mass lesions - can mimic carcinoma |
| Ulcero-hypertrophic | 30% | Mucosal ulcerations combined with healing and scar formation |
Key morphologic feature of intestinal TB ulcer: The ulcers are oriented transversely (circumferentially) along the bowel, perpendicular to the long axis - because TB spreads along the lymphatics which run in the transverse folds (Peyer's patches and lymphoid tissue). This contrasts with Crohn's disease, which produces longitudinal/linear ulcers along the bowel axis. - Sleisenger & Fordtran
Healing of ulcers leads to fibrosis and stricture formation, the most common complication.
Histology
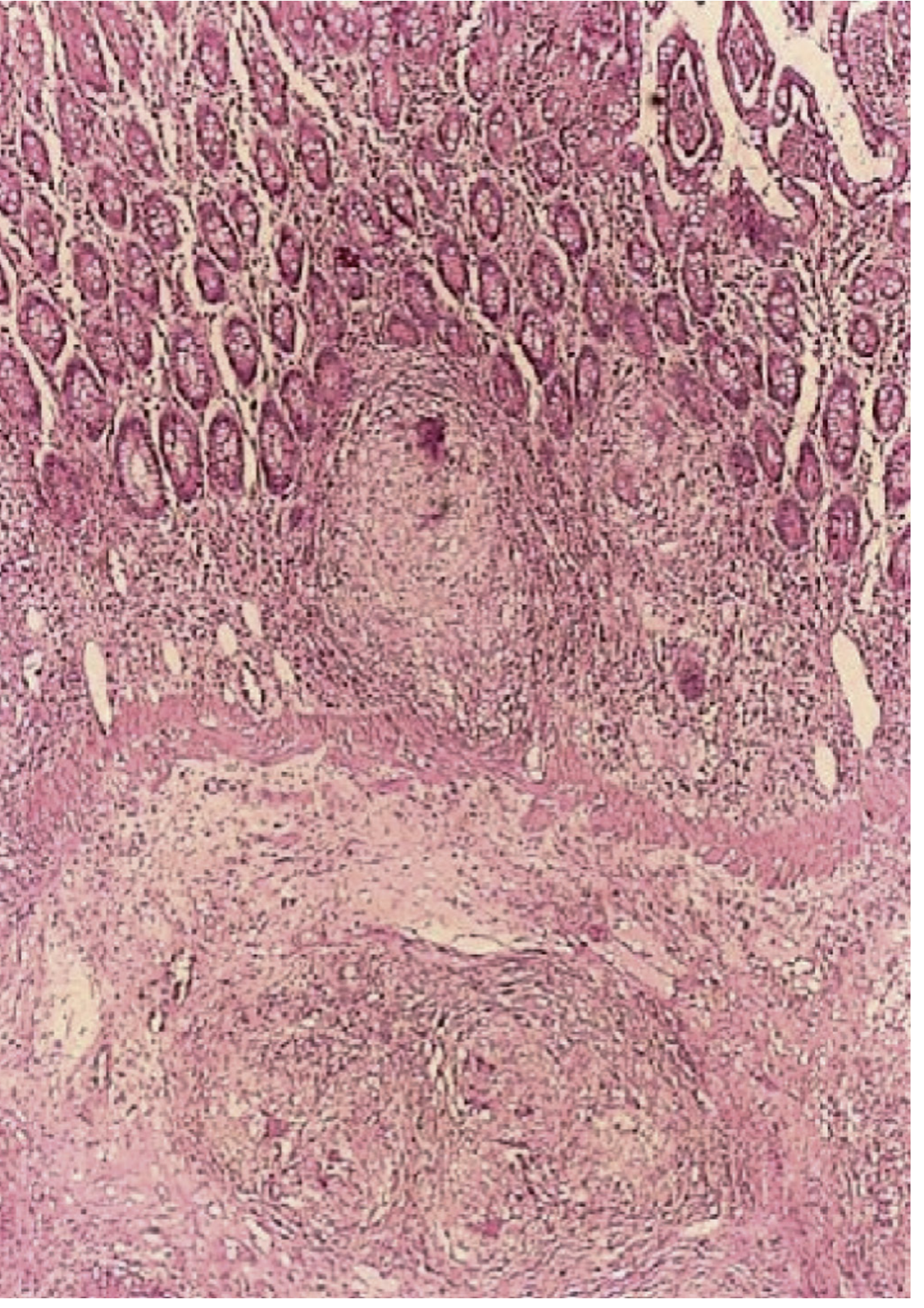
The distinguishing histological lesion is the caseating granuloma, seen in 50-80% of cases. Caseation is common but not always present. AFB are detected by acid-fast stain in ~20% of mucosal samples; PCR is more sensitive (~65%). - Sleisenger & Fordtran
Clinical Features
- Chronic non-specific abdominal pain (80-90% of patients)
- Weight loss, malaise, evening fever (constitutional TB symptoms)
- Alternating diarrhea and constipation
- Blood in stool
- Palpable RLQ mass in 25-50% of patients (ileocecal involvement)
- Doughy feel of abdomen on palpation
- Perianal disease and fistula formation may occur
Emergency presentations:
- Features of small bowel obstruction (the most common complication) - pain, distension, bilious vomiting
- Peritonitis from perforation of a tuberculous ulcer (rare) - Bailey & Love's Surgery
Differentiating from Crohn's Disease
| Feature | Intestinal TB | Crohn's Disease |
|---|---|---|
| Ulcer orientation | Transverse/circumferential | Longitudinal/linear |
| Ileocecal valve | Incompetent (both sides involved) | Usually spared |
| Stierlin sign | Present (conification of cecum) | Absent |
| Lymph nodes on CT | Large (>1 cm), hypodense/caseous | Smaller, reactive |
| Granulomas | Caseating | Non-caseating |
| Perianal disease | Less common | Very common |
| AFB stain/PCR | Positive (if present) | Negative |
Investigations
- Colonoscopy with biopsy - most useful; sends for histopathology, ZN stain, PCR, and culture with drug sensitivities
- Barium meal follow-through / CT enterography - shows strictures, ulcers, bowel wall thickening, calcified mesenteric lymph nodes
- CT abdomen - ileocecal wall thickening, large hypodense mesenteric nodes, asymmetric bowel thickening; Stierlin sign (cecal conification with incompetent ileocecal valve) is characteristic
- Sputum AFB + culture (may not show active pulmonary disease at diagnosis)
- IGRA / Mantoux - positive does not equal active disease; negative in HIV or elderly
- PCR on tissue or stool - most sensitive (~65%) for identifying M. tuberculosis
Treatment of Intestinal TB
Standard anti-TB chemotherapy:
- 2 months of HRZE (isoniazid + rifampicin + pyrazinamide + ethambutol) - intensive phase
- 4 months of HR (isoniazid + rifampicin) - continuation phase = total 6 months
- Surgical intervention may be required for obstruction (even during drug therapy), perforation, or fistula - Sleisenger & Fordtran, Bailey & Love's Surgery
TB is a reportable disease; public health authorities should be notified when suspected. Isolation precautions (masks) are required in the endoscopy suite.
Sources: S Das - A Manual on Clinical Surgery, 13th ed. | Bailey & Love's Short Practice of Surgery, 28th ed. | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.