Anrep effect
Reading File
Finding Sources
Searching PubMed
"Anrep effect" cardiac contractility afterload
Reading File
Reading File
Reading Article
PMID: 38175910
Reading File
Loading Image
Now I have comprehensive information. Here is a full explanation:
The Anrep Effect
Definition
The Anrep effect (described by G.V. Anrep in 1912) is a slow, intrinsic increase in myocardial contractility that occurs in response to an abrupt, sustained rise in afterload (aortic pressure). It is also called homeometric autoregulation because it restores stroke volume without requiring a change in fiber length (i.e., it is independent of the Frank-Starling mechanism).
Two-Phase Response to Acute Afterload Increase
When aortic pressure rises suddenly, the heart responds in two distinct phases:
-
Immediate (Frank-Starling) phase: Ejection is transiently limited, causing end-diastolic volume (EDV) to increase. This stretch increases force at the next beat via the Frank-Starling (length-dependent) mechanism - a heterometric response.
-
Slow phase - the Anrep effect: Over the next seconds to minutes, the inotropic state of the heart gradually increases and Ca2+ transients grow larger, restoring stroke volume toward normal even as EDV returns toward baseline. This slow force response can be reproduced in isolated muscle strips, confirming it is a myocyte-intrinsic phenomenon.
- Braunwald's Heart Disease, p. 49
Mechanism
The molecular basis involves stretch-activated signaling at the cardiomyocyte level:
Classic understanding
- Increased afterload causes mechanical stretch of the myocardium
- Stretch activates autocrine/paracrine signaling pathways
- This leads to enhanced Ca2+ transients (greater Ca2+ release per beat)
- Result: increased force generation at the same fiber length
Current mechanistic model (Braunwald's):
- Increased systolic force is transmitted laterally via Z-discs and cytoplasmic actin to cytoskeletal proteins (focal adhesion complexes, dystrophin, integrin complexes) at cell-matrix junctions
- This activates mechano-signaling, including a NOS1- and CaMKII-dependent increase in Ca2+ transients
- The net result is the gradual inotropic effect
Newest hypothesis (Sequeira et al., Circ Res 2024, PMID: 38175910):
A compelling 2024 review proposes that the Anrep effect involves a two-phase transition of myosin from the super-relaxed (SRX) to the disordered-relaxed (DRX) state:
- Resting myosin exists in equilibrium between SRX (energy-conserving, not ready for force generation) and DRX (contraction-ready) states
- Acute afterload increase mobilizes myosin heads from SRX → DRX, making more cross-bridges available for force generation
- This provides a unified mechanistic explanation linking myosin head availability to the Anrep phenomenon
Comparison: Anrep Effect vs. Frank-Starling Mechanism vs. Bowditch Effect
| Feature | Frank-Starling | Anrep Effect | Bowditch Effect (Treppe) |
|---|---|---|---|
| Trigger | ↑ Preload (fiber length) | ↑ Afterload (aortic pressure) | ↑ Heart rate |
| Mechanism | Length-dependent ↑ Ca2+ sensitivity | Stretch-activated signaling, ↑ Ca2+ transients, SRX→DRX myosin | Frequency-dependent ↑ Ca2+ (less time for efflux) |
| Time course | Beat-to-beat, immediate | Seconds to minutes | Beat-to-beat |
| EDV change | Yes (increases) | Initially ↑, then normalizes | No |
| Type | Heterometric autoregulation | Homeometric autoregulation | Homeometric autoregulation |
Clinical Relevance
1. Normal cardiac adaptation: The Anrep effect helps the heart compensate acutely when aortic pressure rises (e.g., during transient hypertension or exercise).
2. Perioperative/anesthetic context: In aortic cross-clamping during surgery, the reduction in stroke volume may be due to limited preload reserve, myocardial ischemia, or inability of the heart to generate a pressure-induced increase in contractility (failure of the Anrep effect) - Braunwald's/Miller's Anesthesia.
3. Heart failure: In failing hearts, the mechanisms underpinning the Anrep effect (NOS1, CaMKII signaling, proper Ca2+ handling) may be impaired, reducing the heart's ability to adapt to pressure loads.
4. Hypertrophic cardiomyopathy (HCM): The 2024 Sequeira et al. review shows that in HCM, myosin is constitutively shifted toward the DRX state, essentially mimicking a persistent or overactive Anrep effect. This explains the hypercontractility seen in HCM and may provide a therapeutic target (e.g., mavacamten stabilizes the SRX state). Echocardiographic pressure-volume measurements in patients with hypertrophic obstructive cardiomyopathy before septal ablation showed a clinical "Anrep fingerprint": enhanced contractility (leftward shift and steepening of the end-systolic pressure-volume relationship) and prolonged systolic ejection time, which reversed after the procedure.
The Figure Below: Length-Dependent Ca²⁺ Activation
This Braunwald's figure illustrates the foundation of length-dependent contractile enhancement - relevant to how the initial Frank-Starling component of the response works. At a shorter sarcomere length (SL = 1.65 μm, top), the Ca2+ transient is large but force (F) is modest. At near-maximal length (SL = 2.15 μm, bottom), nearly the same Ca2+ transient produces dramatically greater force - because myofilament Ca2+ sensitivity is higher at longer lengths:
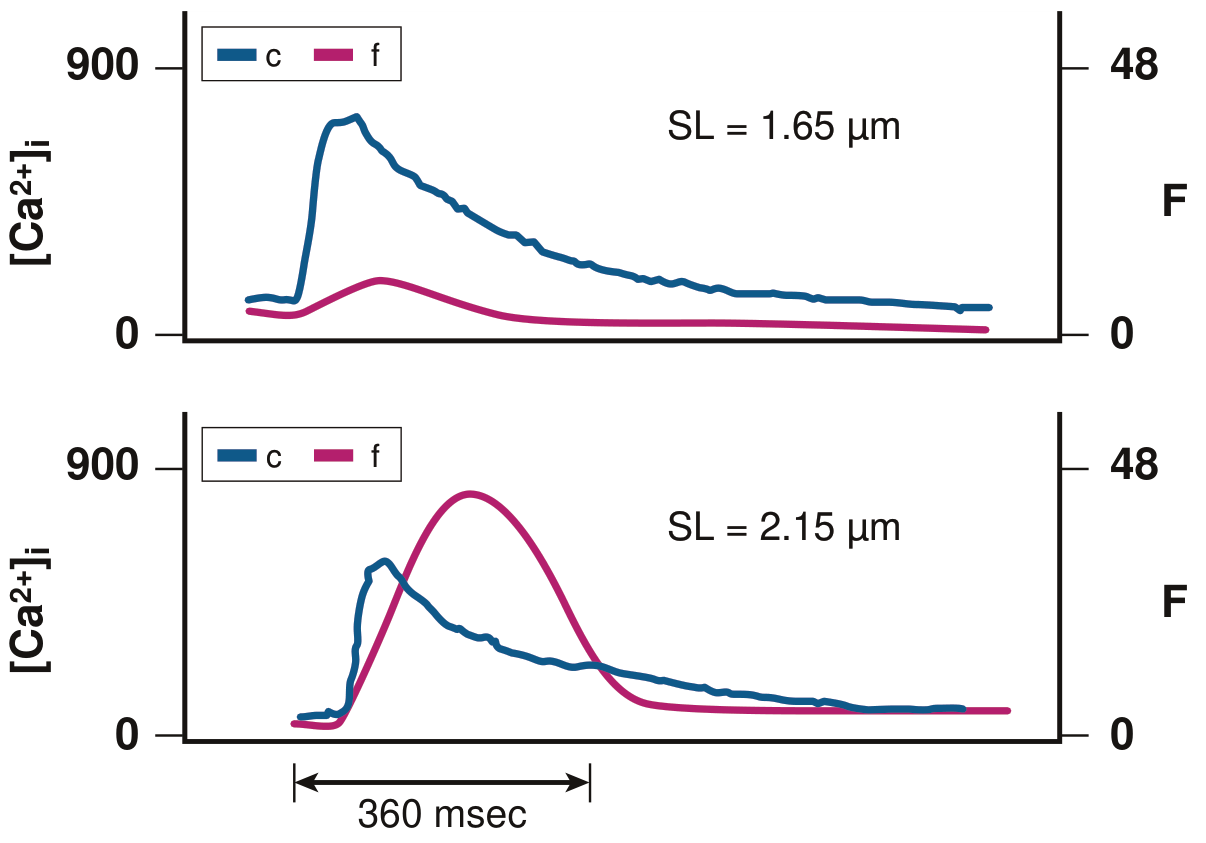
Figure from Braunwald's Heart Disease - Length-dependent enhancement of myofilament Ca2+ sensitivity. Top: SL = 1.65 μm produces modest force despite large Ca2+ transient. Bottom: SL = 2.15 μm produces much greater force with a nearly unchanged Ca2+ transient.
Summary
The Anrep effect is a slow (seconds-to-minutes) homeometric autoregulation where the heart intrinsically increases its contractile force after an acute afterload rise, independent of fiber length changes. The mechanism involves stretch-activated Ca2+ signaling (NOS1/CaMKII pathway) and, per the latest evidence, a transition of myosin heads from the energy-sparing super-relaxed state to the contraction-ready disordered-relaxed state. Pathological overactivation of this mechanism likely underlies the hypercontractility of hypertrophic cardiomyopathy.
This is a shared conversation. Sign in to Orris to start your own chat.